You can’t be both a virulent source AND not have symptoms.
dr. Michael Yeadon
bivši podpredsednik Pfizer
Ne morete biti vir okužbe in NE imeti simptomov
21.11. 2020
https://twitter.com/MichaelYeadon3/status/1330264395344203785
*
"Smešna domenva je, da osebe brez simptomov prenašajo okužbe"
vodilni imunolog na svetu, švicarski profesor dr. Beda Stadler:
(3.18 minuta): https://www.countdowntothekingdom.com/following-the-experts/?fbclid=IwAR2uqcJYWgwR6S0h0dK5iAaeLzvpd-ZzrxZmOAGkvBFoBa87CNr6f6DRrLA
*
Dr. Anthony Fauci, vodja kriznega štaba v ZDA:
asimptomatični ljudje ne širijo okužbe in maske niso potrebne, epidemijo vedno poganjajo osebe s simptomi
https://www.facebook.com/marija.stoj.1/videos/182890243627041
Dr Fauci: (2.30 minut): https://www.countdowntothekingdom.com/following-the-experts/?fbclid=IwAR2uqcJYWgwR6S0h0dK5iAaeLzvpd-ZzrxZmOAGkvBFoBa87CNr6f6DRrLA
*
zdravniki o nesmislu asimptomačinih prenosov (slovenski prevod)
https://www.facebook.com/101017414921399/videos/274795491025512
*
Dr Fauci, WHO in strokovnjaki: asimptomatični ljudje ne širijo okužbe COVID-19 (od 2.30 minute dalje)
https://www.youtube.com/watch?v=wjkzsZG3V1o
*
Predstavnica Svetovne zdravstvene organizacije (WHO) dr. Maria van Kerkhove je 8.junija 2020 sporočila:
Eno izmed vprašanj, ki ste jih postavili, je poročilo o številu asipmtomatičnih primerov. Iz številnih držav slišimo, da x %, nezano število teh oseb nima simptomov bolezni ali pa so v pred simptomatski fazi, to je nekaj dni preden razvijejo resne simptome. V številnih državah za nazaj ugotavljamo, kako so identificirali te primere. Mnoge so identificirali preko sledenja stikov (contact tracing), ko imate znan primer bolezni in nato sledite stikom bolnika z drugimi, za katere upamo, da so že v karanteni in so nekateri bili testirani. In potem izberete ljudi, ki so brez simptomov, ali pa imajo blage simptome.
Ko ugotavljamo za nazaj, koliko izmed njih je bilo resnično brez simptomov, ugotavljamo da je imela večina resnično zelo blage simptome, ki niso COVID-19 bolezen. To pomeni, da še nimajo vročine, kašlja, zadihanosti, ali pa imajo blago obliko bolezni. Tako vemo, da so ljudje, ki so resnično brez simptomov in so pozitivni na PCR testu .
Vaše vprašanje je bilo tudi, kakšen delež ljudi brez simptomov prenaša okužbo s koronavirusi SARS CoV-2?
Potrebno je skrbno spremeljanje teh ljudi, ko so prepoznani in ali pride do sekunadrne transmisije. Imamo poročila iz držav, ki zelo podrobno izvajajo sledenje stikov (contact tracing). Sledijo osebam brez simptomov, njihovim stikom in niso našli sekundarnih transmisij, oziroma je to zelo redek primer. Večina teh podatkov ni objavljena v literaturi. Med študijami, ki so objavljene, imamo eno iz Singapurja, ki je preučila infrastrukturo za dolgoročno oskrbo, imamo tudi nekaj študij o prenosu znotraj družine, ki so sledile osebam nekaj časa in ugotavljali, ali je prišlo do prenosa okužbe na druge. Ves čas spremljamo te podatke in poskušamo dobiti več podatkov iz držav, da bi resnično lahko odgovorili na to vprašanje.
Tako se še vedno zdi, da je zelo redko, da bi asimptomatična oseba v resnici prenesla okužbo naprej na druge ljudi. Na kar se resnično želimo osredotočiti, je sledenje oseb, ki imajo simptome. Če bi sledili vsem osebam, ki imajo simptome, ker je to respiratorni patogen, ki prehaja od okužene osebe preko kapljičnega prenosa, in bi dali osebe, ki so bile v stiku v karanteno, bi drastično znižali število bolnikov. Želela bi vam dati dejansko število, koliko transmisij bi resnično ustavili, a res bi dramtično znižali število prenosov okužbe, če bi se osredotočili na zmanjšanje prenosa. Na podlagi podatkov, ki jih imamo, se zdi izjemno redko, da bi oseba brez simptomov dejansko prenesla okužbo naprej na drugo osebo.
https://www.youtube.com/watch?fbclid=IwAR2gPKLoeS-LQqkds9a0CM7EOR-fHL7EsuQDgzKWcF1aDSMz3n6iR339msk&v=NQTBlbx1Xjs&app=desktop&ab_channel=BloombergMarketsandFinance
Vir: WHO (2.55 minuta): https://www.countdowntothekingdom.com/following-the-experts/?fbclid=IwAR2uqcJYWgwR6S0h0dK5iAaeLzvpd-ZzrxZmOAGkvBFoBa87CNr6f6DRrLA
https://pubmed.ncbi.nlm.nih.gov/32513410/
Stalni izbruh koronavirusne bolezni 2019 (COVID-19) se je razširil po vsem svetu.
Vprašljivo je, ali so asimptomatski nosilci virusa COVID-19 prenašalci okužbe. Tu
poročamo o primeru asimptomatskega bolnika in predstavljamo klinične značilnosti 455
stikov, katerih cilj je preučiti nalezljivost asimptomatskih nosilcev.
455 stikov, ki so bili izpostavljeni asimptomatskemu nosilcu virusa COVID-19, je postalo
predmet naše raziskave. Razdeljeni so bili v tri skupine: 35 bolnikov, 196 družinskih
članov in 224 bolniških uslužbencev. Preučili smo njihove epidemiološke podatke, klinične
evidence, rezultate pomožnih pregledov in terapevtske sheme.
Povprečje kontaktnega časa za bolnike je bilo štiri dni, za družinske člane pa pet dni.
Kardiovaskularne bolezni so predstavljale 25% med prvotnimi boleznimi bolnikov. Poleg
bolnišničnega osebja so bili medicinsko izolirani tako bolniki kot družinski člani. Med
karanteno so se pri sedmih bolnikih in enem družinskem članu pojavili novi respiratorni
simptomi, pri katerih je bila najpogostejša vročina. Število krvnih preiskav v večini stikov
je bilo v mejah normale. Vse slike CT niso pokazale znakov okužbe s COVID-19. Pri testu
nukleinske kisline pri 455 stikih niso odkrili hudih okužb z akutnim respiratornim
sindromom s koronavirusom 2 (SARS-CoV-2).
Vir: str 17: https://drive.google.com/file/d/1Od3pbCnAspzxp_XKR6jrq9cN8eJXhcPR/view
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7219423/
https://www.youtube.com/watch?v=XMRoFy-y1a8&feature=emb_logo
Prenosljivost SARS CoV-2 pri osebah brez simpotov je izredno nizka. Epidemiološki podatki kažejo, da ni prenosa virusov 5 dni po okužbi. Ostanki virusa lahko ostanejo v epitelnih celicah še nekaj tednov ( opomba: in potem je PCR test lažno pozitiven)
Vir: predavanje dr. Mateje Logar nov 2020 https://drive.google.com/drive/folders/1fmoFdjOYyo541QHhLK46fORHTyt_jkbg?fbclid=IwAR06uQwP1u0Ctzh4bMEMS0n1B0-lRit7m8dYzfx2ZCJadZ0uYbdQg5W4_TM
*
Asimptomatski prenos je izumljen leta 2020. Nikoli prej v zgodovini ni obstajal
Bivši podpredsenik Pfizerja, dr. Michael Yeadon
(4.10 min):
*
Med 1.174 tesnimi stiki asimptomatskih primerov ni bilo pozitivnih testov. Kulture virusov so bile negativne za vse asimptomatske pozitivne in repozitivne primere, kar kaže na to, da v tej študiji v pozitivnih primerih ni bilo nobenega "aktivnega virusa". Vsi tesni stiki asimptomatskih pozitivnih primerov so bili negativni, kar kaže, da asimptomatsko pozitivni primeri, odkriti v tej študiji, verjetno ne prenašajo okužbe s koronavirusi SARS CoV-2.
https://www.nature.com/articles/s41467-020-19802-w
*
Povzetek
V Wuhanu so bili med 23. januarjem in 8. aprilom 2020 uvedeni strogi nadzorni ukrepi COVID-19. Ocene razširjenosti okužbe po sprostitvi omejitev bi lahko bile informacije o obvladovanju pandemije po koncu zaustavitve (lockdown). Tu opisujemo presejalni program za odkrivanje nukleinske kisline za SARS-CoV-2 med 14. majem in 1. junijem 2020 v mestu Wuhan. Uključeni so bili prebivalci mesta, stari šest let ali več in sodelovalo je 9.899.828 (92,9%) ljudi. Niso ugotovili novih simptomatskih primerov in najdeno je bilo 300 asimptomatskih primerov (stopnja odkrivanja 0,303 / 10.000, 95% IZ 0,270–0,339 / 10.000). Med 1.174 tesnimi stiki asimptomatskih primerov ni bilo pozitivnih testov. Od 34.424 bolnikov, ki so okrevali po COVID-19, je bilo znova pozitivnih 107 (ponovna pozitivna stopnja 0,31%, 95% IZ 0,423–0,574%). Razširjenost okužbe s SARS-CoV-2 v Wuhanu je bila zato pet do osem tednov po koncu zaklepanja (lockdown) zelo majhna. Uvod Koronavirusna bolezen 2019 (COVID-19) je bila prvič prijavljena decembra 2019, Svetovna zdravstvena organizacija pa jo je 11. marca 2020 (1) označila za pandemijo. Po strogih ukrepih zapiranja je bila epidemija COVID-19 na splošno pod nadzorom na Kitajskem in celotna država je napredovala v fazo po zaustavitvi (post-lockdown). V tej fazi se države soočajo z novimi težavami in izzivi, med drugim s tem, kako natančno oceniti tveganje epidemije COVID-19 po zaustavitvi, kako se izogniti novim valom izbruhov COVID-19 in kako olajšati obnovitev gospodarstva in normalnega socialnega življenja. Kot mesto, ki ga je COVID-19 najbolj prizadel na Kitajskem, je imel Wuhan od 23. januarja do 8. aprila 2020 ukrepe zaklepanja (lockdown). V prvih dveh mesecih po ponovnem odprtju mesta je bilo v Wuhanu le nekaj občasnih primerov COVID-19 (šest na novo potrjenih primerov od 8. aprila do 10. maja 2020(2)). Še vedno pa je obstajala zaskrbljenost zaradi tveganja za COVID-19 v Wuhanu, kar je resno vplivalo na obnovitev industrijske proizvodnje in storitev ter oviralo normalno življenje prebivalcev. Da bi ugotovila trenutno stanje epidemije COVID-19, je mestna vlada Wuhana od 14. maja do 1. junija 2020 izvedla celovit presejalni pregled nukleinske kisline z okužbo s SARS-CoV-2. Preverjanje okužbe s SARS-CoV-2 v mestu v mestu Wuhan je program množičnega presejanja po zaklepanju, ki ponuja neprecenljive izkušnje ali lekcije z mednarodnim pomenom, saj več držav in mest po vsem svetu vstopa v fazo po zapori. V tej študiji poročamo o organizacijskem postopku, podrobnih uporabljenih tehničnih metodah in rezultatih tega preverjanja nukleinskih kislin v mestu. Rezultati
V Wuhanu je bilo upravičenih 10.652.513 ljudi, starih ≥ 6 let (94,1% celotnega prebivalstva). Pregled nukleinske kisline je bil končan v 19 dneh (od 14. maja 2020 do 1. junija 2020) in skupaj je bilo testiranih 9.899.828 oseb od 10.652.513 upravičenih (stopnja udeležbe 92,9%). Od 9.899.828 udeležencev jih 9.865.404 ni imelo predhodne diagnoze COVID-19, 34.424 pa je bilo okrevanih bolnikov s COVID-19. Pri pregledu 9.865.404 udeležencev brez anamneze COVID-19 ni bilo mogoče ugotoviti nobenega na novo potrjenega primera COVID-19, ugotovili pa so 300 asimptomatskih pozitivnih primerov s stopnjo odkrivanja 0,303 (95% IZ 0,270–0,339) / 10.000. Mediane vrednosti Ct stratificiranih asimptomatskih primerov so prikazane v dodatni tabeli 1. Od 300 asimptomatskih pozitivnih primerov sta dva primera prišla iz ene družine, druga dva pa iz druge družine. V teh dveh družinah ni bilo predhodno potrjenih bolnikov s COVID-19. Sledili so skupno 1174 tesnim stikom asimptomatskih pozitivnih primerov in vsi so bili negativni za COVID-19. Bilo je 34.424 okrevanih primerov COVID-19, ki so sodelovali v pregledu. Od 34.424 udeležencev z anamnezo COVID-19 jih je 107 znova bilo pozitivnih na testu, pri čemer je bila ponovno pozitivna stopnja 0,310% (95% IZ 0,423–0,574%). Kulture virusov so bile negativne za vse asimptomatske pozitivne in ponovno pozitivne primere, kar kaže na to, da v tej študiji v pozitivnih primerih ni bilo nobenega "živega virusa". Vsi asimptomatski pozitivni primeri, znova pozitivni primeri in njihovi tesni stiki so bili izolirani vsaj 2 tedna, dokler niso bili rezultati testov nukleinske kisline negativni. Noben od odkritih pozitivnih primerov ali njihovih tesnih stikov med izolacijo ni postal simptomatičen ali na novo potrjen s COVID-19. V tem presejalnem programu je bilo opravljeno enojno oziroma mešano testiranje za 76,7% oziroma 23,3% zbranih vzorcev. Asimptomatske pozitivne stopnje so bile 0,321 (95% IZ 0,282–0,364) / 10.000 oziroma 0,243 (95% IZ 0,183–0,315) / 10.000. Med 300 asimptomatsko pozitivnimi osebami, starimi od 10 do 89 let, je bilo 132 moških (0,256 / 10 000) in 168 žensk (0,355 / 10 000). Asimptomatska pozitivna stopnja je bila najnižja pri otrocih ali mladostnikih, starih 17 let in manj (0,124 / 10.000), najvišja pa pri starejših, starih 60 let in več (0,442 / 10.000) (tabela 1). Asimptomatska pozitivna stopnja pri ženskah (0,355 / 10.000) je bila višja kot pri moških (0,256 / 10 000). Asimptomatski pozitivni primeri so bili predvsem domači in brezposelni prebivalci (24,3%), upokojeni starejši odrasli (21,3%) in delavci v javnih službah (11,7%) (slika 1).
Asimptomatska pozitivna stopnja v mestnih okrožjih je bila v povprečju 0,456 / 10.000, od 0,317 / 10.000 v Hongshanu do 0,807 / 10.000 v okrožju Wuchang. V primestnih okrožjih so ugotovili nižjo stopnjo asimptomatskih pozitivnih primerov (0,132 / 10.000), in sicer od 0,047 / 10.000 v Xinzhou do 0,237 / 10.000 v okrožju Jiangan (slika 2).
Med 7280 stanovanjskimi skupnostmi v Wuhanu so bili v 265 (3,6%) skupnostih ugotovljeni asimptomatsko pozitivni primeri (v 246 skupnostih je bil odkrit le en primer), v drugih 96,4% skupnosti pa niso našli nobenega asimptomatsko pozitivnega primera.
Testiranje protiteles proti virusu SARS-CoV-2 je bilo pozitivno na IgG (+) v 190 od 300 asimptomatskih primerov, kar kaže, da je bilo dejansko okuženih 63,3% (95% IZ 57,6–68,8%) asimptomatsko pozitivnih primerov. Delež asimptomatsko pozitivnih primerov z IgM (-) in IgG (-) je bil 36,7% (95% IZ: 31,2–42,4%; n = 110), kar kaže na možnost okužbe ali lažno pozitivne rezultate testiranja nukleinske kisline (Tabela 2).
V okrožjih Wuchang, Qingshan in Qiaokou je bila višja stopnja odkrivanja asimptomatsko okuženih oseb, razširjenost predhodno potrjenih primerov COVID-19 pa je bila v treh okrožjih 68.243 / 10.000, 53.767 / 10.000 oziroma 100.047 / 10.000. Slika 3 kaže, da so okrožja z visoko stopnjo odkrivanja asimptomatsko pozitivnih oseb na splošno imela visoko prevalenco potrjenih primerov COVID-19 (rs = 0,729, P = 0,002).
Razprava
Pregled nukleinske kisline za okužbo s SARS-CoV-2 v Wuhanu je uključil skoraj 10 milijonov ljudi in ni odkril nobenih potrjenih primerov s COVID-19. Stopnja odkrivanja asimptomatsko pozitivnih primerov je bila zelo nizka in ni bilo dokazov o prenosu od asimptomatsko pozitivnih oseb na izsledene tesne stike. V 96,4% stanovanjskih skupnosti ni bilo asimptomatskih pozitivnih primerov. Prejšnje študije so pokazale, da so bili asimptomatski posamezniki, okuženi z virusom SARS-CoV-2, nalezljivi (3) in bi lahko kasneje postali simptomatski (4). V primerjavi s simptomatskimi bolniki imajo asimptomatsko okužene osebe na splošno majhno količino virusnih obremenitev in kratkotrajno prenašanje virusov, kar zmanjša tveganje za prenos SARS-CoV-2 (5). V tej študiji so virusno kulturo izvedli na vzorcih iz asimptomatsko pozitivnih primerov in niso odkrili nobenega aktivnega virusa SARS-CoV-2. Vsi tesni stiki asimptomatskih pozitivnih primerov so bili negativni, kar kaže, da asimptomatsko pozitivni primeri, odkriti v tej študiji, verjetno niso nalezljivi. Pri okrevanih bolnikih s COVID-19 v Wuhanu je bila nizka stopnja ponovne pozitivnosti. Rezultati gojenja virusov in sledenja kontaktov niso odkrili dokazov, da so bili pozitivni primeri pri okrevanih bolnikih s COVID-19 nalezljivi, kar je v skladu z dokazi iz drugih virov. Študija v Koreji ni pokazala nobenega potrjenega primera COVID-19 s spremljanjem 790 stikov 285 ponovno pozitivnih primerov (6). Uradni nadzor nad okrevanimi bolniki s COVID-19 na Kitajskem prav tako ni razkril nobenih dokazov o nalezljivosti ponovno pozitivnih primerov (7). Glede na močno okužbo s COVID-19 (8,9,10) se pričakuje, da je število potrjenih primerov povezano z nevarnostjo okužbe v skupnostih. Ugotovili smo, da so bile asimptomatske pozitivne stopnje v različnih okrožjih Wuhana povezane z razširjenostjo predhodno potrjenih primerov. To je v skladu s časovnim in prostorskim razvojem (zlasti dolgoročne) nalezljivih bolezni (11). Obstoječe laboratorijske kulture virusnih študij in genske študije (9,10) so pokazale, da lahko virulenca virusa SARS-CoV-2 sčasoma slabi, na novo okužene osebe pa so bile bolj verjetno brez simptomov in z nižjo virusno obremenitvijo kot prej okuženi primeri. S centralizirano izolacijo in zdravljenjem vseh primerov COVID-19 v obdobju zaklepanja v Wuhanu se je tveganje, da bi bili prebivalci okuženi v skupnosti, močno zmanjšalo. Ko so dovzetni prebivalci izpostavljeni majhnim odmerkom virusa, so lahko zaradi lastne imunosti brez simptomov. Ko so dovzetni prebivalci izpostavljeni majhnim odmerkom virusa, so lahko zaradi lastne imunosti brez simptomov. Testiranje seroloških protiteles v sedanji študiji je pokazalo, da je bilo le 63% asimptomatsko pozitivnih primerov dejansko okuženih z virusom SARS-CoV-2. Kljub temu je prezgodaj za zadovoljstvo zaradi obstoja asimptomatskih pozitivnih primerov in visoke stopnje dovzetnosti prebivalcev v Wuhanu. Ukrepi javnega zdravja za preprečevanje in nadzor epidemije COVID-19, vključno z nošenjem mask, zagotavljanjem varne socialne oddaljenosti v mestu Wuhan naj se nadaljujejo. Še posebej je treba še naprej ustrezno varovati ranljive populacije z oslabljeno imunostjo ali sočasnimi boleznimi ali oboje. Ugotovitve te študije kažejo, da je bil COVID-19 v času presejalnega programa v Wuhanu dobro nadzorovan. Po dveh mesecih od presejalnega programa (do 9. avgusta 2020) v Wuhanu ni bilo na novo potrjenih primerov COVID-19. Izvedena so bila nadaljnja testiranja SARS-CoV-2 v vzorcih, zbranih v tržnih okoljih v Wuhanu in niso našli nobenih pozitivnih rezultatov po preverjanju skupno 52.312 vzorcev iz 1795 tržnih okoljij med 13. junijem in 2. julijem 2020 (12). Ta študija ima več omejitev, o katerih je treba razpravljati. Prvič, to je bil presečni presejalni program in sprememb asimptomatsko pozitivnih in ponovnih operativnih rezultatov skozi čas ne moremo oceniti. Drugič, čeprav pozitiven rezultat testiranja nukleinske kisline razkriva obstoj virusnih RNK, je verjetno prišlo do nekaterih lažno negativnih rezultatov, zlasti zaradi razmeroma nizke stopnje obremenitve z virusom pri asimptomatsko okuženih posameznikih, neustreznega zbiranja vzorcev in omejene natančnosti tehnologije testiranja (13). Čeprav presejalni program ni predložil neposrednih dokazov o občutljivosti in specifičnosti uporabljene testne metode, je metaanaliza poročala o združeni občutljivosti 73% (95% IZ 68–78%) za testiranje brisov nazofaringa in žrela na COVID-19 (14). Vlada je javno kupila preskusne komplete, uporabljene v presejalnem programu, ki so jih pogosto uporabljali na Kitajskem in v drugih državah. Sprejeti so bili številni ukrepi za zmanjšanje lažno negativnih rezultatov presejalnega programa. Na primer, izvedeno je bilo standardno usposabljanje zdravstvenih del za odvzem vzorcev, da se zagotovi kakovost vzorcev. Postopki poskusov, vključno z odvzemom vzorcev, ekstrakcijo in PCR, so bili v skladu z uradnimi smernicami (dodatna opomba 1). Za oceno RT-PCR v realnem času sta bila hkrati testirana dva ciljna gena. Kljub temu so lažni negativni rezultati še vedno bili možni, tako kot v drugih programih množičnega presejanja. Tudi če bi bila občutljivost testa le 50%, in bi bila dejanska razširjenost dvakrat večja, kot so poročali v tej študiji, bi bila še vedno zelo nizka. Približno 7,1% upravičenih prebivalcev ni sodelovalo v mestnem presejanju nukleinske kisline in presejalni program ni zbral podrobnih podatkov o razlogih za neudeležbo, kar je omejitev te študije. Čeprav ni bilo uradnih statističnih podatkov, je veliko število delavcev migrantov in študentov pred zaprtjem zapustilo Wuhan in se pridružilo svojim družinam v drugih mestih ali provincah zaradi tradicionalnega kitajskega novega leta. Zato je verjetno, da večina udeležencev v času programa ni bila v Wuhanu. Glavni cilj presejalnega programa je bil oceniti tveganje za epidemijo COVID-19 pri prebivalcih, ki so dejansko živeli v Wuhanu po koncu zaklepanja. Zato na ocenjene pozitivne stopnje verjetno ne bo bistveno vplivala neudeležba prebivalcev, ki niso bili v Wuhanu, ali nekaterih prebivalcev, ki niso sodelovali iz drugih razlogov. Poleg tega so bili ljudje, ki so zapustili Wuhan, ciljna populacija za spremljanje v drugih provincah in mestih in so morali opraviti testiranje nukleinskih kislin. Čeprav v tej populaciji ni bilo uradnih statističnih podatkov, ki bi prikazovali pozitivno stopnjo testiranja nukleinske kisline, ni poročila, ki bi pokazalo višjo pozitivno stopnjo testiranja nukleinske kisline od naših ugotovitev.
Če povzamemo, stopnja odkrivanja asimptomatsko pozitivnih primerov v Wuhanu po zaustavitvi je bila zelo nizka (0,303 / 10.000) in ni bilo dokazov, da so ugotovljeni asimptomatski pozitivni primeri prenašali okužbo na druge. Te ugotovitve so odločevalcem omogočile prilagoditev strategij preprečevanja in nadzora v obdobju po koncu zaklepanja. Potrebne so nadaljnje študije za popolno oceno vplivov in stroškovne učinkovitosti programov za preverjanje s SARS-CoV-2 na zdravje prebivalstva, zdravstveno vedenje, gospodarstvo in družbo.
*
https://www.nature.com/articles/s41467-020-19802-w.pdf
*
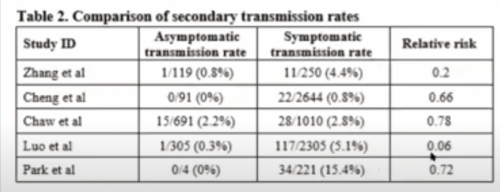
Študija: Asimptomatski prenos: Metaanaliza 54 študij, ki so preučujele okužbe v hišah, kjer ljudje živijo skupaj, v katere je bilo vključenih skoraj 78.000 udeležencev, je pokazala, da ima asimptomatsko ali pred simptomatsko prenašanje virusov indeks 0,7 %. Z drugimi besedami, 1 asimptomatična oseba bi morali srečati približno 140 ljudi ZNOTRAJ HIŠE, da bi okužili drugega. Možnost okužbe na večjih območjih (npr. trgovinah) in zlasti kadar je zunaj verjetno veliko manj, če boste morda morali naleteti na tisoče ljudi, preden okužite drugega.
https://pubmed.ncbi.nlm.nih.gov/33315116/
-----------------------------
In a separate, larger meta-analysis of 79 studies, asymptomatic transmission was 1.4%, which is double the previous meta-analysis but still incredibly small.
https://pubmed.ncbi.nlm.nih.gov/32960881
*
https://www.technocracy.news/mercola-asymptomatic-people-do-not-spread-covid-19/
According to media reports, COVID-19 “cases,” meaning positive PCR test results, are soaring across the U.S. and around the world, leading to the implementation of measures that in some cases are stricter than what we endured during the initial wave.
However, as detailed in several recent articles, including “Why COVID-19 Testing Is a Tragic Waste,” PCR tests are being used incorrectly, resulting in the false appearance of widespread transmission.
In reality, the vast majority of people who end up with a positive test will not develop symptoms and aren’t infectious. Needless to say, if you’re not infectious, you pose no health risk to anyone, and being placed under what amounts to house arrest is nothing but cruel and unusual punishment for no reason whatsoever.
Positive Test Rates Have No Bearing on Mortality Rates
In The Highwire report above, Del Bigtree breaks down how excessively high test sensitivity leads to falsely elevated “case” numbers that in reality tell us nothing about the situation at hand. As noted by Bigtree, what’s missing from the COVID-19 conversation is the actual death rate.
“If COVID is a deadly virus, what should we see when cases increase?” he asks. The answer, of course, is an increase in deaths. However, that’s not what’s happening.
Aside from a small bump at the beginning, when doctors were unsure of the appropriate treatment and some states recklessly and irresponsibly sent infected patients into ill equipped nursing homes, the death rate has remained relatively flat while positive test rates have dramatically risen and fallen in intervals.
In the video, Bigtree features a November 4, 2020, tweet1 by White House coronavirus adviser Dr. Scott Atlas showing the number of positive tests (aka “cases”) in blue and COVID-19 related deaths in red, since the start of the pandemic up until the end of October 2020. As you can see, there’s no correlation between the positive test rate and subsequent deaths.
Vast Majority of ‘COVID-19 Patients’ Are Asymptomatic
One of the explanations for why positive test rates and mortality do not go hand in hand is the simple fact that a vast majority of those testing positive for SARS-CoV-2 are asymptomatic. They simply aren’t sick. The PCR test is merely picking up inactive (noninfectious) viral particles.
In one study,2 which looked at pregnant women admitted for delivery, 87.9% of the women who tested positive for the presence of SARS-CoV-2 had no symptoms. Another study3 looked at a large homeless shelter in Boston. After a cluster of COVID-19 cases was observed there, researchers conducted symptoms assessments and testing among all guests residing at the shelter over a two-day period.
Of 408 people tested, 147, or 36%, were positive, yet symptoms were conspicuously absent. Cough occurred in only 7.5% of cases, shortness of breath in 1.4% and fever in 0.7%. All symptoms were “uncommon among COVID-positive individuals,” the researchers noted.
Asymptomatic Transmission Is Very Rare
During a June 8, 2020, press briefing, Maria Van Kerkhove, the World Health Organization’s technical lead for the COVID-19 pandemic, made it very clear that asymptomatic transmission is very rare, meaning an individual who tests positive but does not exhibit symptoms is highly unlikely to transmit live virus to others.
“We have a number of reports from countries who are doing very detailed contact tracing. They’re following asymptomatic cases, they’re following contacts, and they’re not finding secondary transmission … it’s very rare, and much of that is not published in the literature,” Van Kerkhove said.
Just one day later, Dr. Mike Ryan, executive director of the WHO’s emergencies program, backpedaled Van Kerkhove’s statement, saying the remarks were “misinterpreted.”4 Needless to say, when you’re trying to justify the implementation of a vast surveillance network, it’s no good to admit a vast majority of people are having their privacy infringed upon for no good reason whatsoever.
Asymptomatic People Pose No Risk to Others
Most recently, a study5 in Nature Communications assessed the risk posed by asymptomatic people by looking at the data from a mass screening program in Wuhan, China.
The city had been under strict lockdown between January 23 and April 8, 2020. Between May 14 and June 1, 2020, 9,899,828 residents of Wuhan city over the age of 6 underwent PCR testing. In all, 92.9% of the entire city population participated in the testing. Of these, 9,865,404 had no previous diagnosis of COVID-19 and 34,424 were recovered COVID-19 patients.
Not a single one of the 1,174 people who had been in close contact with an asymptomatic individual tested positive.
In all, there were zero symptomatic cases and only 300 asymptomatic cases detected. (The overall detection rate was 0.3 per 10,000.) Importantly, not a single one of the 1,174 people who had been in close contact with an asymptomatic individual tested positive.
Additionally, of the 34,424 participants with a history of COVID-19, 107 individuals (0.310%) tested positive again, but none were symptomatic. As noted by the authors:6
“Virus cultures were negative for all asymptomatic positive and repositive cases, indicating no ‘viable virus’ in positive cases detected in this study … The 300 asymptomatic positive persons aged from 10 to 89 years …
The asymptomatic positive rate was the lowest in children or adolescents aged 17 and below (0.124/10,000), and the highest among the elderly aged 60 years and above (0.442/10,000). The asymptomatic positive rate in females (0.355/10,000) was higher than that in males (0.256/10,000).”
Asymptomatic People Have Low Viral Load
Interestingly, when they further tested asymptomatic patients for antibodies, they discovered that 190 of the 300, or 63.3%, had actually had a “hot” or productive infection resulting in the production of antibodies. Still, none of their contacts had been infected.
In other words, even though asymptomatics were (or had been) carriers of apparently live virus, they still did not transmit it to others. As noted by the authors, “there was no evidence of transmission from asymptomatic positive persons to traced close contacts.” They further added:7
“Compared with symptomatic patients, asymptomatic infected persons generally have low quantity of viral loads and a short duration of viral shedding, which decrease the transmission risk of SARS-CoV-2.
In the present study, virus culture was carried out on samples from asymptomatic positive cases, and found no viable SARS-CoV-2 virus. All close contacts of the asymptomatic positive cases tested negative, indicating that the asymptomatic positive cases detected in this study were unlikely to be infectious.”
Reinfected Individuals Are Not Infectious Either
The same held true for people who tested positive a second time after having recovered from an active infection.
“Results of virus culturing and contract [sic] tracing found no evidence that repositive cases in recovered COVID-19 patients were infectious, which is consistent with evidence from other sources,” the authors said.8
The researchers also pointed out that virus cultures and genetic studies have shown the virulence of SARS-CoV-2 appears to be weakening over time, and that newly infected individuals are more likely to be asymptomatic and have a lower viral load than the cases seen earlier in the outbreak.
What does all of this tell us? It tells us there’s no reason to panic simply because the number of positive tests are on the rise. Remember, the more people you test using a PCR test that is set to an excessive cycle threshold, the more false positives you’ll get.
As explained in “Asymptomatic ‘Casedemic’ Is a Perpetuation of Needless Fear,” by using an excessive cycle threshold that amplifies the viral RNA to the point that it detects inactive (noninfectious) particles is at the heart of this so-called pandemic. It’s what keeps the pandemic narrative going, when in fact it’s long since over.
CDC Uses Questionable Sources to Counter China Study
Interestingly, the same day the China study came out, the U.S. Centers for Disease Control and Prevention updated its guidance9,10 on mask wearing, claiming asymptomatic people account for more than half of all transmissions. Where did they get that from?
The two references listed as support for that claim include a study11 from July 2020, and CDC data that haven’t even been published yet.12 It just says it was “submitted” for publication sometime in 2020, therefore, we are unable to provide any source link. The CDC makes no mention of the China study, which included nearly 10 million individuals.
CNN, which reported the CDC’s update, parroting the idea that asymptomatic spread is why it’s so important to wear a mask, also made no mention of the landmark study from China. Curious, don’t you think? It’s almost as though the CDC doesn’t want us to know we have nothing to fear from healthy people.
Many doctors, scientists and lawyers have now become wise to the fact that it is these flawed tests, and their fraudulent use, that is keeping the fear narrative alive — and they're taking action.
In the video above, Ben Swann talks to Dr. Reiner Fuellmich,13 a consumer protection trial lawyer14 and founding member of the German Corona Extra-Parliamentary Inquiry Committee (Außerparlamentarischer Corona Untersuchungsausschuss15),16,17 which is seeking to expose how fraudulent testing has been and continues to be used to engineer the appearance of a dangerous pandemic when in fact there is none.
The committee is now filing the first of many lawsuits to come, this one against so-called fact checkers on social media. They opted to file a defamation lawsuit on behalf of Dr. Wolfgang Wodarg, a former member of the German Congress and the Council of Europe who has been an outspoken critic of PCR testing, as it cannot be used to diagnose infection.
Social media companies have labeled Wodarg's statements as "false," and by filing a defamation suit, the burden of proof now falls on the fact checkers to prove that they are correct. In other words, to win, the fact checkers must prove that PCR tests diagnose active infection. The scientific evidence proves they don't, so this case could turn out to be pivotal in the fight against the big tech censorship that keeps the fearmongering alive.
COVID-19 Pandemic — The Greatest Psyop in History?
While Fuellmich and his team make no claims about WHY the pandemic is being kept alive using fraudulent science, they are unequivocal in their assertion that it is in fact a fake pandemic and that it has had devastating health and economic consequences around the world.
For the why, we have to turn to the geopolitical scene to see what narratives have rolled out in tandem with the pandemic. What we find is that leaders across the world are now calling for a "reset" of the global economy in the wake of the destruction brought by the pandemic. In reality, of course, it is the global response to the pandemic that created the economic devastation, not the virus itself.
Either way, the call to "build back better" is being heard around the world, and such plans include the elimination of conventional capitalism, free enterprise and private ownership, replacing them with a technocratic resource-based economic system in which energy and social engineering run the economy rather than pricing mechanisms such as supply and demand.
Leaders are also calling for invasive health surveillance, and there appear to be plans in place to use biometric surveillance via vaccines, all of which feed into the technocratic system in which this kind of mass surveillance is not only paramount but also foundational.
The reason surveillance is so crucial is because the functioning of this system hinges on artificial intelligence-driven social engineering and manipulation of the masses. Unless people are locked into what could be described as a digital prison, they won't comply with what's coming.
Hook everyone up to a digital centralized banking system, a digital ID and a social credit score, however, and few will have the fortitude to object or speak out against the unelected rulers. Your entire life could easily be upended with the push of a button.
We've already seen how many people have not only been deplatformed for speaking out against one thing or another this past year, they've also had their digital payment accounts closed down, effectively destroying their ability to earn a living. Imagine if there were nothing but a centralized digital currency system and your accounts got shut down. How would you live?
Fear Is a Highly Effective Manipulation Tool
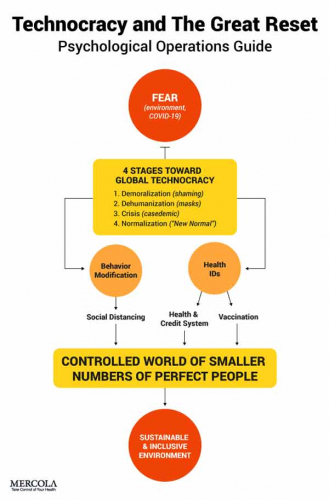
No person in their right mind would agree to this Great Reset plan if they were aware of all the details and its ultimate implications for humanity as a whole. So, to roll it out, they had to use psychological manipulation, and fear is the most effective tool there is.
As explained by psychiatrist Dr. Peter Breggin, there's an entire school of public health research that focuses on identifying the most effective ways to frighten people into accepting desired public health measures.
By adding confusion and uncertainty to the mix, you can bring an individual from fear to anxiety — a state of confusion in which you can no longer think logically — and in this state, you are more easily manipulated. The following graphic illustrates the central role of fearmongering for the successful rollout of the Great Reset.
In closing, testing asymptomatic people and isolating people who test positive even when they have no symptoms is a key strategy that keeps the fear level high. There simply aren't enough hospitalized COVID-19 patients to keep the ruse going, and far too few actually die to make the narrative work. That's why we hear nothing about those statistics anymore.
Instead, all we hear about are the "cases" — the positive tests which have no bearing on mortality rates. Fear of asymptomatics also drive the narrative that we must all wear face masks everywhere we go, because you don't know who might be infected and not know it. It instills fear of others, as even seemingly healthy people might make you deathly ill.
The featured study from Wuhan demonstrates the fallacy of such fears. People who test positive but have no symptoms are not infectious and pose no risk to others. They don't need to wear masks and they don't need to be isolated. In short, we don't need to fear each other.
*
https://www.aier.org/article/asymptomatic-spread-revisited/
The conclusion is not that asymptomatic spread is rare or that the science is uncertain. The study revealed something that hardly ever happens in these kinds of studies. There was not one documented case. Forget rare. Forget even Fauci’s previous suggestion that asymptomatic transmission exists but not does drive the spread. Replace all that with: never. At least not in this study for 10,000,000.
From what I can tell, there was only one news story that was posted about this. It was on Russia Today. I’ve not been able to find another one. People not following the right accounts on Twitter wouldn’t even know about it at all.
*
Dr. Michael Yeadon: V medicini ne obstaja asimptomatični prenos, to je izmišljeno za potrebe lockdowna:
https://rumble.com/vfr30h-michael-yeadon-iluzija-covida.html?fbclid=IwAR1UrlVyG3nL0o4qQe9Pxc0tBCntS00TKUaL_LSt7emrrPghRYuMHO2THbk
*
Intra-Household and Close-Contact SARS-CoV-2 Transmission Among Children - a Systematic Review
https://pubmed.ncbi.nlm.nih.gov/33898355/
Abstract
Introduction: The outbreak of the novel coronavirus disease (COVID-19) caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) has led to a range of emergency measures worldwide. Early in the pandemic, children were suspected to act as drivers of the COVID-19 spread in the population, which was based on experiences with influenza virus and other respiratory pathogens. Consequently, closures of schools and kindergartens were implemented in many countries around the world, alongside with other non-pharmaceutical interventions for transmission control. Given the grave and multifaceted consequences of contact restriction measures for children, it is crucial to better understand the effect size of these incisive actions for the COVID-19 pandemic. Therefore, we systematically review the current evidence on transmission of SARS-CoV-2 to and by children. Data Sources: PubMed and preprints uploaded on medRxiv. Study Selection: Original research articles, case reports, brief communications, and commentaries were included into the analysis. Each title or abstract was independently reviewed to identify relevant articles. Studies in other languages than English were not included. Data Extraction: Two reviewers independently reviewed the selected studies. Extracted data included citation of each study, type of healthcare setting, location of the study, characteristics of patient population, and reported outcomes. Results: Data on transmission of SARS-CoV-2 on or by children is scarce. Several studies show a lower seropositivity of children compared to adults, suggesting a lower susceptibility of especially younger children. Most insight currently comes from household studies suggesting, that children are predominantly infected by their household contacts. The contagiousness however, seems to be comparable between children and adults, based on our meta-analysis of included studies. Conclusions: Larger and systematic studies are urgently needed to better understand the age dependent patterns of SARS-CoV-2 transmission and thereby design more effective non-pharmaceutical interventions to reduce disease transmission.
*
https://www.naturalnews.com/2021-05-17-cdc-lying-about-outdoor-covid-transmission.html
*
*
ne obstaja asimptomatični prenos: https://www.facebook.com/ines.sugar/videos/1459801594357860
*
Dr. Fauci: asimptomatski prenosi niso nikoli bili vir okužb: https://www.facebook.com/Jasonshurka26/videos/3023011528021029/?extid=NS-UNK-UNK-UNK-AN_GK0T-GK1C
*
Asimptomatski prenos je laž: dr. Fauci, prof. Sucharit Bhakdi
https://www.facebook.com/stoplaznivimmedijem/videos/3418109271624246
*
Zasad neevaluirani članak kineskih znanstvenika, ukazao je da PCR testovi daju lažno negativne rezultate i to uglavnom kod pacijenata s blažim simptomima. Procjena je da bi lažno negativnih rezultata mogla biti trećina kod osoba s lakšim oboljenjem. Harlan Krumholz, profesor medicine s Yalea, smatra da je taj udio možda i veći.
https://www.medrxiv.org/content/10.1101/2020.02.11.20021493v2
Ipak, spomenuto istraživanje kineskih znanstvenika moguće je pronaći po naslovu i ono doista govori o “47 posto ili više lažno pozitivnih testova kod asimptomatičnih osoba”.
Ne radi se, dakle, o osobama koje su bolesne, nego onima koje su bile u kontaktu s oboljelima od Covida-19 i ne pokazuju simptome. Priča je utoliko zanimljivija kada se vidi da je izdavač odlučio povući ovaj znanstveni rad.
https://pubmed.ncbi.nlm.nih.gov/32133832/
Editor office’s response for Ahead of Print article withdrawn The article “Potential false-positive rate among the ‘asymptomatic infected individuals’ in close contacts of COVID-19 patients” was under strong discussion after pre-published. Questions from the readers mainly focused on the article’s results and conclusions were depended on theoretical deduction, but not the field epidemiology data and further researches were needed to prove the current theory. Based on previous discussions, the article was decided to be offline by the editorial board from the pre-publish lists. Objective: As the prevention and control of COVID-19continues to advance, the active nucleic acid test screening in the close contacts of the patients has been carrying out in many parts of China. However, the false-positive rate of positive results in the screening has not been reported up to now. But to clearify the false-positive rate during screening is important in COVID-19 control and prevention. Methods: Point values and reasonable ranges of the indicators which impact the false-positive rate of positive results were estimated based on the information available to us at present. The false-positive rate of positive results in the active screening was deduced, and univariate and multivariate-probabilistic sensitivity analyses were performed to understand the robustness of the findings. Results: When the infection rate of the close contacts and the sensitivity and specificity of reported results were taken as the point estimates, the positive predictive value of the active screening was only 19.67%, in contrast, the false-positive rate of positive results was 80.33%. The multivariate-probabilistic sensitivity analysis results supported the base-case findings, with a 75% probability for the false-positive rate of positive results over 47%. Conclusions: In the close contacts of COVID-19 patients, nearly half or even more of the 'asymptomatic infected individuals' reported in the active nucleic acid test screening might be false positives.
*
*
Sep 28, 2020



