
Even a Military-Enforced Quarantine Can’t Stop the Virus, Study Reveals


The New England Journal of Medicine has published a study that goes to the heart of the issue of lockdowns. The question has always been whether and to what extent a lockdown, however extreme, is capable of suppressing the virus. If so, you can make an argument that at least lockdowns, despite their astronomical social and economic costs, achieve something. If not, nations of the world have embarked on a catastrophic experiment that has destroyed billions of lives, and all expectation of human rights and liberties, with no payoff at all.
[The earliest version of this article misstated the conditions of the control group. They were equally locked down with those who participated in the study. The difference between the two concerned testing frequency and the isolation response. This does not affect this article’s conclusion; indeed it strengthens it: even under extreme measures, the virus spread, and more so with the extra measure intended to control the virus. Nearly all infections were without symptoms.]
AIER has long highlighted studies that show no gain in virus management from lockdowns. Even as early as April, a major data scientist said that this virus becomes endemic in 70 days after the first round of infection, regardless of policies. The largest global study of lockdowns compared with deaths as published in The Lancet found no association between coercive stringencies and deaths per million.
To test further might seem superfluous but, for whatever reason, governments all over the world, including in the US, still are under the impression that they can affect viral transmissions through a range of “nonpharmaceutical interventions” (NPIs) like mandatory masks, forced human separation, stay-at-home orders, bans of gatherings, business and school closures, and extreme travel restrictions. Nothing like this has been tried on this scale in the whole of human history, so one might suppose that policy makers have some basis for their confidence that these measures accomplish something.
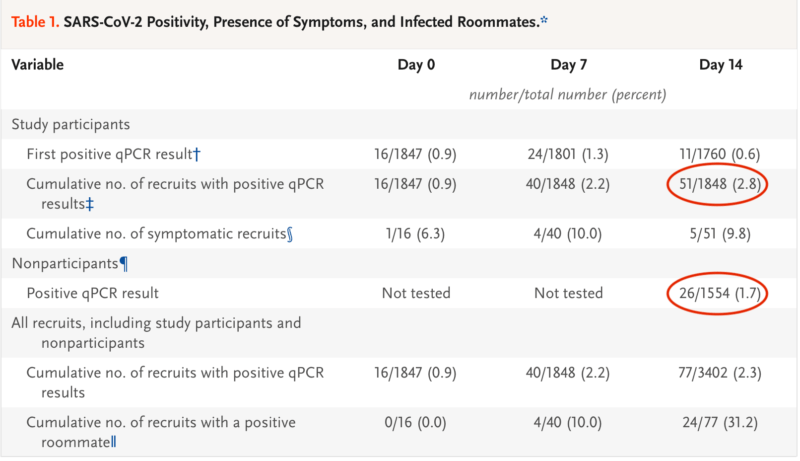
A study conducted by Icahn School of Medicine at Mount Sinai in cooperation with the Naval Medical Research Center sought to test lockdownsm along with testing and isolation. In May, 3,143 new recruits to the Marines were given the option to participate in a study of frequent testing under extreme quarantine. The study was called CHARM, which stands for COVID-19 Health Action Response for Marines. Of the recruits asked, a total of 1,848 young people agreed to be guinea pigs in this experiment which involved “which included weekly qPCR testing and blood sampling for IgG antibody assessment.” In addition, the CHARM study volunteers who did test positively “on the day of enrollment (day 0) or on day 7 or day 14 were separated from their roommates and were placed in isolation.”
What did the recruits have to do? The study explains, and, as you will see, they faced an even more strict regime that has existed in civilian life in most places. All recruits, even those not in the CHARM group, did the following.
All recruits wore double-layered cloth masks at all times indoors and outdoors, except when sleeping or eating; practiced social distancing of at least 6 feet; were not allowed to leave campus; did not have access to personal electronics and other items that might contribute to surface transmission; and routinely washed their hands. They slept in double-occupancy rooms with sinks, ate in shared dining facilities, and used shared bathrooms. All recruits cleaned their rooms daily, sanitized bathrooms after each use with bleach wipes, and ate preplated meals in a dining hall that was cleaned with bleach after each platoon had eaten. Most instruction and exercises were conducted outdoors. All movement of recruits was supervised, and unidirectional flow was implemented, with designated building entry and exit points to minimize contact among persons. All recruits, regardless of participation in the study, underwent daily temperature and symptom screening. Six instructors who were assigned to each platoon worked in 8-hour shifts and enforced the quarantine measures. If recruits reported any signs or symptoms consistent with Covid-19, they reported to sick call, underwent rapid qPCR testing for SARS-CoV-2, and were placed in isolation pending the results of testing.
Instructors were also restricted to campus, were required to wear masks, were provided with preplated meals, and underwent daily temperature checks and symptom screening. Instructors who were assigned to a platoon in which a positive case was diagnosed underwent rapid qPCR testing for SARS-CoV-2, and, if the result was positive, the instructor was removed from duty. Recruits and instructors were prohibited from interacting with campus support staff, such as janitorial and food-service personnel. After each class completed quarantine, a deep bleach cleaning of surfaces was performed in the bathrooms, showers, bedrooms, and hallways in the dormitories, and the dormitory remained unoccupied for at least 72 hours before reoccupancy.
The reputation of Marine basic training is that it is tough going but this really does take it to another level. Also, this is an environment where those in charge do not mess around. There was surely close to 100% compliance, as compared with, for example, a typical college campus.
What were the results? The virus still spread, though 90% of those who tested positive were without symptoms. Incredibly, 2% of the CHARM recruits still contracted the virus, even if all but one remained asymptomatic. “Our study showed that in a group of predominantly young male military recruits, approximately 2% became positive for SARS-CoV-2, as determined by qPCR assay, during a 2-week, strictly enforced quarantine.”
And how does this compare to the control group that was not tested and not isolated in the case of a positive case?
Have a look at this chart from the study:
Which is to say that the nonparticipants actually contracted the virus at a slightly lower rate than those who were under an extreme regime. Conversely, extreme enforcement of NPIs plus more frequent testing and isolation was associated with a greater degree of infection.
I’m grateful to Don Wolt for drawing my attention to this study, which, so far as I know, has received very little attention from any media source at all, despite having been published in the New England Journal of Medicine on November 11.
Here are four actual media headlines about the study that miss the point entirely:
- CNN: “Many military Covid-19 cases are asymptomatic, studies show”
- SciTech Daily: “Asymptomatic COVID-19 Transmission Revealed Through Study of 2,000 Marine Recruits”
- ABC: “Broad study of Marine recruits shows limits of COVID-19 symptom screening”
- US Navy: “Navy/Marine Corps COVID-19 Study Findings Published in New England Journal of Medicine”
No national news story that I have found highlighted the most important finding of all: extreme quarantine plus frequent testing and isolation among military recruits did nothing to stop the virus.
The study is important because of the social structure of control here. It’s one thing to observe no effects from national lockdowns. There are countless variables here that could be invoked as cautionary notes: demographics, population density, preexisting immunities, degree of compliance, and so on. But with this Marine study, you have a near homogeneous group based on age, health, and densities of living. And even here, you see confirmed what so many other studies have shown: lockdowns are pointlessly destructive. They do not manage the disease. They crush human liberty and produce astonishing costs, such as 5.53 million years of lost life from the closing of schools alone.
The lockdowners keep telling us to pay attention to the science. That’s what we are doing. When the results contradict their pro-compulsion narrative, they pretend that the studies do not exist and barrel ahead with their scary plans to disable all social functioning in the presence of a virus. Lockdowns are not science. They never have been. They are an experiment in social/political top-down management that is without precedent in cost to life and liberty.
[The earliest version of this article misstated the conditions of the control group. They were equally locked down with those who participated in the study. The difference between the two concerned testing frequency and the isolation response. This does not affect this article’s conclusion; indeed it strengthens it: even under extreme measures, the virus spread, and more so with the extra measure intended to control the virus. Nearly all infections were without symptoms.]
Vir: https://www.aier.org/article/even-a-military-enforced-quarantine-cant-stop-the-virus-study-reveals/?__FB_PRIVATE_TRACKING__=%7B%22loggedout_browser_id%22%3A%2270f7edab2d04ab2ca259abdbc62344db2203f5b5%22%7D&fbclid=IwAR0fFUWYfgGNk_DX3PRQ5dl0oICMMNnyf2LLtpe8ktLw4RuUZ0Q8rX_TxPk
*
Lockdown je napaka: https://www.aier.org/article/twelve-times-the-lockdowners-were-wrong/
*
30 študij o nekoristnosti zaklepanja (lockdowna) :
*
Ukrepi zaklepanja (lockdowna) nimajo vpliva na število smrti zaradi COVID-19. Krivulji sta podobni na Švedskem, kjer ni lockdowna in v Veliki Britaniji, ki ima lockdown, in na Švedskem je manj smrti.
https://www.youtube.com/watch?v=juzmwylbpSc&feature=youtu.be
*
https://www.datascienceassn.org/content/did-lockdown-work-economist’s-cross-country-comparison
4. Conclusions The lockdowns in most Western countries have thrown the world into the most severe recession since World War II and the most rapidly developing recession ever seen in mature market economies. They have also caused an erosion of fundamental rights and the separation of powers in large part of the world as both democratic and autocratic regimes have misused their emergency powers and ignored constitutional limits to policy-making (Bjørnskov and Voigt, 2020). It is therefore important to evaluate whether and to which extent the lockdowns have worked as officially intended: to suppress the spread of the SARS-CoV-2 virus and prevent deaths associated with it. Comparing weekly mortality in 24 European countries, the findings in this paper suggest that more severe lockdown policies have not been associated with lower mortality. In other words, the lockdowns have not worked as intended.
?
Gregor Repovž Mladina: ukrepi ne delujejo, nimamo prave strategije, samo represivne ukrepe- Politično s Tanjo Gobec 13.12. 2020
*
UK: It is clear that the COVID epidemic began 23rd Feb and was over by mid-May. Peaking after 5 weeks and lasting around 12 weeks puts it right in the expected range for a virus outbreak. In other words, interventions didn't change nature.


*
https://www.medrxiv.org/content/10.1101/2020.07.22.20160341v3
Claimed benefits of lockdown appear grossly exaggerated.
*
Deviation from the vertical axis indicates extent to which the labelled factor was associated with a change in covid19 death rates. As can be seen, lockdowns & other restrictions were not linked to reduced death rates. This paper doesn’t study negative impacts of measures, but...
https://twitter.com/MichaelYeadon3/status/1343491419286208513/photo/1

160 countries & 850,000 covid19 deaths were studied in excruciating detail. Age & obesity associated with more deaths. But nothing Govts did (principally lockdown & other restrictions) made any difference to deaths.
https://www.frontiersin.org/articles/10.3389/fpubh.2020.604339/full
Conclusion: Countries that already experienced a stagnation or regression of life expectancy, with high income and NCD rates, had the highest price to pay. This burden was not alleviated by more stringent public decisions. Inherent factors have predetermined the Covid-19 mortality: understanding them may improve prevention strategies by increasing population resilience through better physical fitness and immunity.
Obrtno podjetniška zbornica Slovenije poroča
Within Europe, death rates due to covid-19 vary greatly, with some countries being hardly hit while others to date are almost unaffected. It would be of interest to pinpoint the factors that determine a country’s susceptibility to a pandemic such as covid-19.
Here we present data demonstrating that mortality due to covid-19 in a given country could have been largely predicted even before the pandemic hit Europe, simply by looking at longitudinal variability of all-cause mortality rates in the years preceding the current outbreak. The variability in death rates during the influenza seasons of 2015-2019 correlate to excess mortality caused by covid-19 in 2020 (R2=0.48, p<0.0001). In contrast, we found no correlation between such excess mortality and age, population density, degree of urbanization, latitude, GNP, governmental health spendings or rates of influenza vaccinations.
These data may be of some relevance when discussing the effectiveness of acute measures in order to limit the spread of the disease and ultimately deaths. They suggest that in some European countries there is an intrinsic susceptibility to fatal respiratory viral disease including covid-19; a susceptibility that was evident long before the arrival of the current pandemic.
https://www.medrxiv.org/content/10.1101/2020.12.25.20248853v1
*
dr. Michael Yeadon Twitter 6.1. 2020: Sir Desmond is the only MP with the brains & spine to point out that, as lockdowns do not reduce lives lost, it is madness to continue to apply this medieval torture to society. frontiersin.org/articles/10.33 The evidence is strong that this policy is ineffective yet harmful.
Covid-19 Mortality: A Matter of Vulnerability Among Nations Facing Limited Margins of Adaptation
Results: Higher Covid death rates are observed in the [25/65°] latitude and in the [−35/−125°] longitude ranges. The national criteria most associated with death rate are life expectancy and its slowdown, public health context (metabolic and non-communicable diseases (NCD) burden vs. infectious diseases prevalence), economy (growth national product, financial support), and environment (temperature, ultra-violet index). Stringency of the measures settled to fight pandemia, including lockdown, did not appear to be linked with death rate.
Conclusion: Countries that already experienced a stagnation or regression of life expectancy, with high income and NCD rates, had the highest price to pay. This burden was not alleviated by more stringent public decisions. Inherent factors have predetermined the Covid-19 mortality: understanding them may improve prevention strategies by increasing population resilience through better physical fitness and immunity.
Vir: https://www.frontiersin.org/articles/10.3389/fpubh.2020.604339/full
*
*
Študija Stanford univerza 5.1. 2021: dr. Ionnidis: Več ukrepov ne pomeni manj COVID-19 primerov
Conclusions
While small benefits cannot be excluded, we do not find significant benefits on case growth of more restrictive NPIs. Similar reductions in case growth may be achievable with less restrictive interventions.
Vir: https://onlinelibrary.wiley.com/doi/10.1111/eci.13484
https://www.naturalhealth365.com/mandatory-lockdowns-stanford-3706.html
*
Dr. Michael Yeadon 13.1. 2021
A carefully written website by an expert who often provides expert advice in legal matters. Not a lightweight to be brushed aside. Those overseeing PCR mass testing have questions to answer & its perplexing that they’re not being addressed.
https://probabilityandlaw.blogspot.com/search/label/COVID?m=1
*
https://thecritic.co.uk/in-defence-of-lockdown-sceptics/
*
Študija o pandemiji gripe 2006: Ukrepi niso učinkoviti: An overriding principle. Experience has shown that communities faced with epidemics or other adverse events respond best and with the least anxiety when the normal social functioning of the community is least disrupted. Strong political and public health leadership to provide reassurance and to ensure that needed medical care services are provided are critical elements. If either is seen to be less than optimal, a manageable epidemic could move toward catastrophe.
*
https://www.facebook.com/100004006819810/videos/2263207247156147
Ph D, Professor Emeritus, University of Paris Descartes, Miroslav Radman is a geneticist and molecular biologist recognized for some of his ground-breaking work on DNA repair, recombination and mutation
"Teško je odgovoriti zašto se dogodio pad jer nema kontrolnog eksperimenta, no rad koji će uskoro izaći od grupe profesora na sveučilištu Stanford pokazuje da nema detektirane beneficije od striktnih, rigoroznih mjera s obzirom na ove osrednje, slabije", rekao je Miroslav Radman i za N1 dodatno pojasnio:
"Zatvaranje restorana, maske na otvorenom, po toj najkompetentnijoj studiji koju sam vidio, odgovor je da se ne isplati, da nema beneficija od toga. Jedva čekamo da taj rad izađe da se može komentirati", kaže Radman.
Smatra da bi do pada došlo i bez mjera.
https://www.seebiz.eu/drustvo/radman-ljudi-koji-su-umrli-u-vezi-s-infekcijom-korone-umrli-bi-i-bez-nje/249855/?fbclid=IwAR27ZhXWIKnqIMx_L_RJPhwgZG1D-RZbJ4dqpIUG1VrUAwxEktuo_Q8l8Zs
*
Zaklepanje COVID-a bo povzročilo več kot milijon "odvečnih smrti": Harvard, Duke, Johns Hopkins akademiki menijo, da lahko smrtni primeri, ki jih povzročijo dolgoročna zaklepanja, "daleč presegajo" tiste, ki jih povzroča dejanski virus SARS CoV-2.
*
Sedanja popolna stava razvitih držav na dolge lockdowne in cepljenje je absolutno kratkovidna in škodljiva tako za prebivalstvo kot za gospodarstvo in delovna mesta. Jožef P Damjan
*
*
Prvič, vladni ukrepi kljub omejitvam gibanja med občinami, kljub nošenju mask tudi na prostem, kljub prepovedi zbiranja, kljub zaprtju vseh nenujnih trgovin, kljub zaprtju vrtcev in šol in kljub policijski uri ne po šestih, ne po osmih in ne po dvanajstih tednih niso uspeli obrniti krivulje epidemije navzdol.
*
Assessing mandatory stay‐at‐home and business closure effects on the spread of COVID‐19
FUNDING INFORMATION:
The study was funded with support from the Stanford COVID‐19 Seroprevalence Studies Fund.
Abstract
Background and Aims
The most restrictive nonpharmaceutical interventions (NPIs) for controlling the spread of COVID‐19 are mandatory stay‐at‐home and business closures. Given the consequences of these policies, it is important to assess their effects. We evaluate the effects on epidemic case growth of more restrictive NPIs (mrNPIs), above and beyond those of less‐restrictive NPIs (lrNPIs).
Methods
We first estimate COVID‐19 case growth in relation to any NPI implementation in subnational regions of 10 countries: England, France, Germany, Iran, Italy, Netherlands, Spain, South Korea, Sweden and the United States. Using first‐difference models with fixed effects, we isolate the effects of mrNPIs by subtracting the combined effects of lrNPIs and epidemic dynamics from all NPIs. We use case growth in Sweden and South Korea, 2 countries that did not implement mandatory stay‐at‐home and business closures, as comparison countries for the other 8 countries (16 total comparisons).
Results
Implementing any NPIs was associated with significant reductions in case growth in 9 out of 10 study countries, including South Korea and Sweden that implemented only lrNPIs (Spain had a nonsignificant effect). After subtracting the epidemic and lrNPI effects, we find no clear, significant beneficial effect of mrNPIs on case growth in any country. In France, for example, the effect of mrNPIs was +7% (95% CI: −5%‐19%) when compared with Sweden and + 13% (−12%‐38%) when compared with South Korea (positive means pro‐contagion). The 95% confidence intervals excluded 30% declines in all 16 comparisons and 15% declines in 11/16 comparisons.
Conclusions
While small benefits cannot be excluded, we do not find significant benefits on case growth of more restrictive NPIs. Similar reductions in case growth may be achievable with less‐restrictive interventions.
https://onlinelibrary.wiley.com/doi/10.1111/eci.13484?fbclid=IwAR0ckWQHvfzszHdJA3MwHjE5O1JtKgVbnrb8Q8hvufIA0Geo9Gbu8cmDQ9Q
Prof. Ionnidis komentira študijo o COVID-19 ukrepih: lockdown ima škodljive posledice, zato ker varuje tiste, ki niso ogroženi in ne ne varuje tistih, ki so ogroženi in to so prebivalci domov za starejše občane: Poleg tega zaradi lockdowna ljudem niso bile dostopne zdravstvene storitve, kar je ogrožilo javno zdravje in življenja ljudi, ocenjuje se da bo zaradi tega umrlo 1.5 milijona ljudi zaradi zanemarjanja programov za tuberkulozo: 24.00 minut:
https://www.youtube.com/watch?v=9szCNNZrPK8
John P. A. Ioannidis, MD, DSc Professor of Medicine, Epidemiology and Population Health, Biomedical Data Science and Statistics Stanford University.
*
Jay Bhattacharya, Stanford Doctor, Calls Lockdowns the 'Biggest Public Health Mistake We've Ever Made'
8.3. 2021
Jay Bhattacharya, a professor at Stanford University Medical School, recently said that COVID-19 lockdowns are the "biggest public health mistake we've ever made...The harm to people is catastrophic."
Several U.S. states have started to ease their COVID-19 restrictions over the past few weeks.
Bhattacharya, who made the comments during an interview with the Daily Clout, co-authored the Great Barrington Declaration, a petition that calls for the end of COVID-19 lockdowns, claiming that they are "producing devastating effects on short and long-term public health."
As of Monday, the Great Barrington Declaration has received signatures from over 13,000 medical and public health scientists, more than 41,000 medical practitioners and at least 754,399 "concerned citizens."
"One is that people who are older have a much higher risk from dying from COVID than people who are younger...and that's a really important fact because we know who his most vulnerable, it's people that are older. So the first plank of the Great Barrington Declaration: let's protect the vulnerable," Bhattacharya said. "The other idea is that the lockdowns themselves impose great harm on people. Lockdowns are not a natural normal way to live."
*
Stats Canada claims lockdowns, not COVID-19, are now driving ‘excess deaths’
Abstract
I explore the association between the severity of lockdown policies in the first half of 2020 and mortality rates. Using two indices from the Blavatnik Centre’s COVID-19 policy measures and comparing weekly mortality rates from 24 European countries in the first halves of 2017–2020, addressing policy endogeneity in two different ways, and taking timing into account, I find no clear association between lockdown policies and mortality development.
https://academic.oup.com/cesifo/advance-article/doi/10.1093/cesifo/ifab003/6199605?fbclid=IwAR1ufZE0S5uWt8hIr3cgBcFyiQEXtHQyBxHlHlod0YD7hRqPuDZzfHrWWro
*
Primerjava med Kalifornijo in Florido
*
Mexico: López Obrador says pandemic lockdowns are the tactic of dictators
‘The fundamental thing is to guarantee liberty,’ says Mexican president when asked why he almost never wears a mask
https://www.theguardian.com/world/2020/dec/02/mexico-lopez-obrador-pandemic-lockdowns-dictatorship?fbclid=IwAR2V5QK0A5z31RRakoWkoZeeuQCL3vNGYnuWfJc1_O8JfLMGeCMo_ndSWes
* * *
Molekularni genetik prof.dr. Tomislav Terzin: Ne ubija nas virus, ampak ukrepi zaklepanja. Pod pretvezo virusa se ukinjajo vse človekove pravice.
https://www.facebook.com/stoplaznivimmedijem/videos/502177767475812
* * *
* * *
*
Prof. dr Valerije Vrček o Barrington deklaraciji, nesmislu ukrepov in PCT testu
https://www.youtube.com/watch?v=TaNj2pE9Qqw
*
*
http://web.archive.org/web/20210426005104/https://www.telegraph.co.uk/news/2021/04/24/lockdown-proponents-cant-escape-blame-biggest-public-health/
*
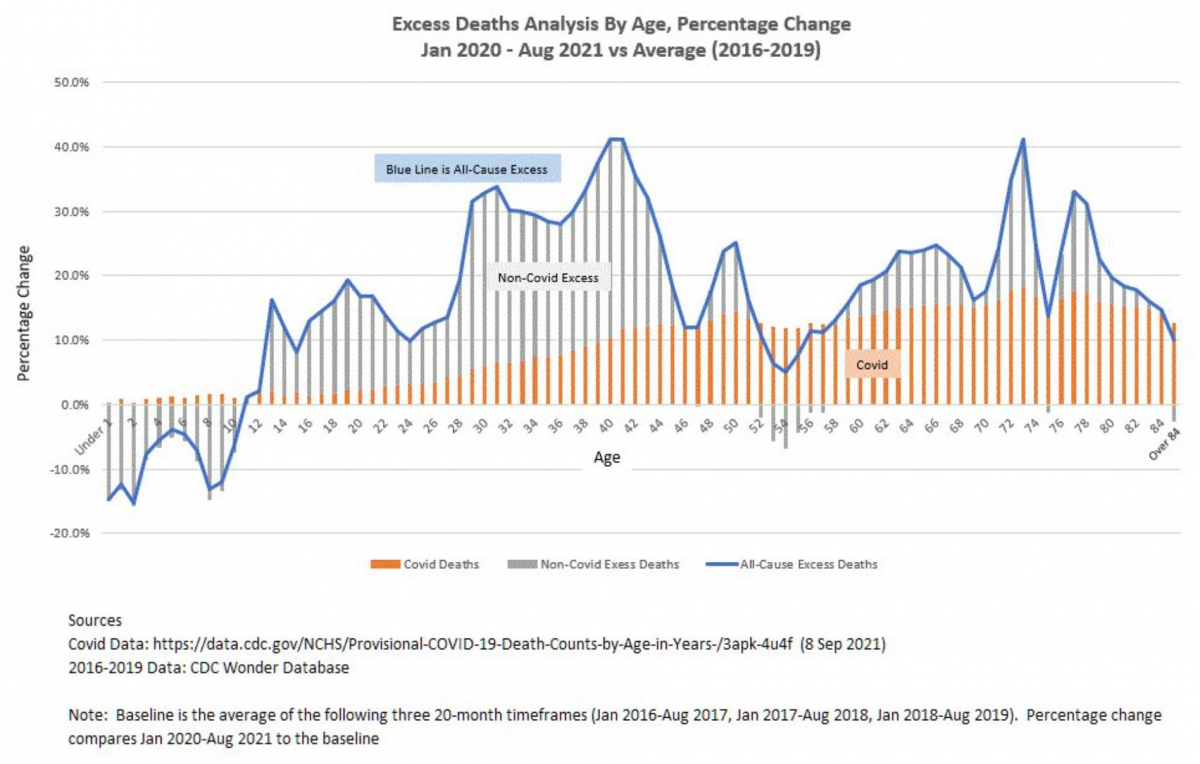
No kada pogledamo smrtnost u Europi, viškovi smrtnosti koje vidimo u 2020. i 2021. su evidentno prisutni, no nisu drastično veći no primjerice 2017. godine. Prema prvim procjenama smrtnosti to je trebalo izgledati puno gore. Da smo početkom 2020. znali stvarnu opasnost koja nam prijeti od ovog virusa, niti jedna zemlja ne bi uvodila drastične mjere zatvaranja kakve su provodili u većini zemalja. A da stvar bude još gora, te drastične mjere zatvaranja zapravo nisu imale gotovo nikakav učinak, što najbolje vidimo na primjerima Češke, Slovačke, Mađarske i Slovenije, koje su imale puno, puno strože mjere od Hrvatske, a na kraju su imali više umrlih od nas. Osobna odgovornost i oprez je naravno zaštitila velik broj ljudi od zaraze, no razne zabrane i ograničenja rada su tu imale vrlo mali učinak, a uzrokovali su puno štete. Gordan Lauc
*
Povečana smrtnost zaradi ukrepov v VB: Od svibnja 2020. do svibnja 2021. kod svoje kuće je umrlo čak 60 posto više ljudi oboljelih od dijabetesa, Parkinsonove bolesti, demencije i Alzheimerove bolesti u odnosu na prosjek od 2015. do 2019. godine. Smrtnost kod kuće oboljelih od najčešćih karcinoma skočila je za više od 40 posto, dok je u bolnicama istovremeno pala za gotovo 30 posto, a u hospicijima za 22 posto.
Postoje teze da su mnogi od tih ljudi na vlastiti zahtjev otišli kući iz bolnica ili domova za starije, ali kako navodi Telegraph, to ne objašnjava sav porast viška smrtnosti, a čak i da su doista svi ti pacijenti samo otišli kućama, i dalje postoji mogućnost da su umirali bez pristupa lijekovima za ublažavanje bolova, njegovateljima ili palijativnoj skrbi.
*
https://www.lifesitenews.com/news/lockdowns-are-the-single-biggest-mistake-in-public-health-history-stanford-medical-professor/?utm_source=telegram&fbclid=IwAR3sBKtgSDRZ3UUmV_-tvgBdGPisHsycnKLBnHH4eq28FzmavzcTyZ4bDG8
*
https://www.aier.org/article/covid-19-mandates-will-not-work-for-the-delta-variant/?fbclid=IwAR0vtqs6FjXYhmraRwZ_W06DfHrh5kzLbeFbduCT0PqpyO-6rtRQmMEhwI0
*
Figelj, dr. med: Epidemiološki ukrepi ubijajo: https://revijazarja.si/clanek/zgodbe/613681b68c38b/zmanipulirali-so-nas-v-otopelost?fbclid=IwAR3I4D7zFVCVPKuKisLBtfCysWldqF4CBD8jApn-hNp_mO7Wl9iVT7GXFls
Shaharova analiza?
Analiza se je ukvarjala z umrljivostjo na Švedskem v zadnjih dvajsetih letih. Pokazala je, da covid-19 praktično ni vplival na umrljivost Švedov. Čeprav je Švedska izbrala relativno blag način spopadanja z epidemijo, je njena presežna smrtnost za leto 2020 znašala 1,5 odstotka. Ta pribitek na večjo umrljivost Švedov je bil posledica zelo blage gripe in torej nižje umrljivosti leto pred tem. Opozoril pa bi na še eno pomembno dejstvo.
Katero?
Da je bila presežna smrtnost v letu 2020 pri nas občutno višja kot na Švedskem. In sicer 12-odstotna. Visoka presežna smrtnost je bila nasploh značilna za mnoge države, ki so se odločile za zelo restriktivne ukrepe. Iz razkoraka med našo in švedsko smrtnostjo je mogoče vsaj utemeljeno sumiti, da restriktivni epidemiološki ukrepi ubijajo.
Saj prav to že skoraj od začetka bega … Kako je za večino presežnih smrti kriv virus, ne pa recimo to, da smo razparali nebo in zemljo v imenu boja proti njemu.
Ljudem smo otežili dostop do zdravstvenih ustanov. Mnogi zdravstvene pomoči niso iskali zaradi strahu pred okužbo. Vsi, ki se ukvarjamo s paliativno medicino, dobro vemo, da izolacija za starostnike pomeni zgodnejšo smrt. Prav gotovo k napačni predstavi, kako ogrožajoč je covid-19, prispeva tudi dejstvo, da smo vsem, ki so imeli pred smrtjo pozitiven nosni bris, napisali, da so umrli zaradi covida. Velika večina teh ljudi je v resnici umrla zaradi napredovale krhkosti ali napredovale demence, zaradi napredovalega raka ali napredovale odpovedi organa. Če bi pravilno beležili vzroke smrti, bi bilo jasno, da zaradi covida ne umre tako veliko ljudi.
Da kot umrle zaradi covida rutinsko beležijo celo umrle za rakom, prometnimi nesrečami in samomori, je za našo revijo potrdil sam dr. Krek. Sam pa se zadnje čase čedalje bolj sprašujem o še enem pomembnem vidiku, in sicer o kužnosti asimptomatskih bolnikov. Torej tistih, ki so imeli pozitiven bris na virus, a so brez simptomov. Kaj pravijo zadnja medicinska dognanja o tem?
Asimptomatski bolniki ne okužijo skoraj nikogar. Tako je pokazala analiza 54 raziskav, ki so vključevale več kot 70.000 bolnikov s covidom. Ugotovljeno je bilo, da bolniki s simptomi okužijo 18 odstotkov družinskih članov. Asimptomatski ljudje, torej na virus pozitivni ljudje brez simptomov, pa okužijo le 0,7 odstotka družinskih članov. Manj kot en odstotek. Pozor: doma, kjer vemo, da se epidemioloških ukrepov ne držimo! Maske torej niso potrebne. Mi pa smo jih morali nositi celo zunaj, kjer vemo, da je možnost prenosa okužbe praktično nična.
Stopnjujejo se grožnje, da jih bomo morali spet nositi.
Res je, ustrahovanje kar ne pojenja. Menim, da je ustrahovanje ena izmed največjih tragedij epidemije. Zdravstveno osebje je dolžno pomagati ljudem. Ne sme ustrahovati. Dokazano je bilo, da kronični strah zelo slabi imunski sistem. In da ljudje, ki jih je strah, pogosteje zbolijo za kužnimi boleznimi ter imajo pogosteje težji potek bolezni. Strah je prav gotovo prispeval, da nas je več zbolelo. In da je bilo več težjih potekov bolezni.
*
https://www.delo.si/gospodarstvo/novice/zaskrbljeni-zaradi-novih-ukrepov/
*
Poslanec v hrvaškem parlamentu o škodljivosti lockdowna: https://www.facebook.com/zabasasa/videos/531866904520610
*
UKREPI ZAKLEPANJA SO POVEČALI PRESEŽNO SMRTNOST
Avtorji študije: Virat Agrawal, Jonathan H. Cantor, Neeraj Sood & Christopher M. Whaley
Številne države in zvezne države ZDA so za upočasnitev prenosa COVID-19 uvedle politiko zatočišča na kraju samem (SIP- priporočilo, da ljudje ostanejo doma, omejitve gibanja itd...). Vendar so učinki politik SIP na javno zdravje a priori dvoumni, saj imajo lahko nenamerne škodljive učinke na zdravje.
Učinki politik SIP na prenos COVID-19 in fizično mobilnost so različni. Da bi razumeli neto učinke politik SIP, smo merili spremembo presežka smrti po izvajanju politik SIP v 43 državah in vseh zveznih državah ZDA. Za količinsko opredelitev sprememb v številu prekomernih smrti po izvajanju politike SIP smo uporabili študije dogodkov.
Ugotovili smo, DA SE PO IZVAJANJU POLITIK SIP (OMEJITEV GIBANJA IN NAVODIL, DA OSEBE OSTANEJO DOMA) PRESEŽNA UMRLJIVOST POVEČA.
Povečanje prekomerne umrljivosti je statistično značilno v neposrednih tednih po uvedbi SIP (za mednarodno primerjavo) in se pojavi kljub dejstvu, da se je pred uvedbo politike število prekomerne umrljivosti zmanjšalo.
Na ravni ameriških zveznih držav se je presežna umrljivost povečala v neposrednih tednih po uvedbi SIP, nato pa je po 20 tednih izvajanja SIP padla pod ničlo. Nismo ugotovili, da bi bilo v državah ali zveznih državah ZDA, ki so politike SIP uvedle prej in v katerih so politike SIP delovale dlje časa, manj presežnih smrti kot v državah/državah ZDA, ki so politike SIP uvajale počasneje. Prav tako nismo opazili razlik v trendih presežka smrti pred in po izvajanju politik SIP na podlagi stopenj umrljivosti COVID-19 pred uvedbo SIP.
Vir: https://www.nber.org/papers/w28930?s=09
*
Ukrepi ubijajo: https://www.facebook.com/photo/?fbid=10227098405553852&set=a.10213803578511485
Hrvaški znanstvenik Gordan Lauc okt 2021: Nema nikakve sumnje da je SARS-CoV-2 ubio velik broj ljudi i to nitko normalan ne osporava.
Nažalost sve je više dokaza da je naš odgovor na pandemiju, ono što popularno zovemo "mjere", već do sada ubio barem jednako toliko ljudi koliko ih je ubio virus. Najnoviji primjer je analiza viška smrtnosti u SAD-u u posljednijh 18 mjeseci.
Nažalost te iste "mjere" koje su ubile ljude su spriječile vrlo malo virusom uzrokovanih smrti, a posljedice "mjera" ubijat će još godinama.
the financial press is starting to declare covid restrictions pointless
*
Impact of the COVID-19 pandemic on the oncologic activities (diagnosis, treatment, clinical trials enrollment) of a general hospital in a district with high prevalence of SARS-COV-2 in Italy https://pubmed.ncbi.nlm.nih.gov/34977981/
Support Care Cancer. 2022 Jan 3. doi: 10.1007/s00520-021-06667-y. Epub ahead of print. PMID: 34977981.
“Results: In 2020, a significant reduction in new cancer diagnosis was demonstrated when compared with 2019, with 17.4% fewer cancer diagnoses, 84.5% fewer patients enrolled in clinical trials, a 10.6% reduction in intravenous antitumor treatment, and a 42.7% increase in oral anticancer treatment. Conclusion: Our data indicate a significant reduction in cancer diagnosis, antitumor venous treatment, and patients enrolled in clinical research studies in 2020 compared with 2019, although there was a significant increase in oral treatment. These data suggest that the COVID-19 pandemic had a deep impact on the real-world management of cancer patients in a district of Italy with a high prevalence of COVID-19.”
Importance: Although this data is for Italy only, reports such as this have been rolling in worldwide over the past year. Clearly, we must re-imagine how patients can receive preventative health care as well as important medical treatments in the timely manner in the face of a chronic ongoing pandemic. Absence of innovative leadership is compromising health and wellness systems throughout the world. Telemedicine, mobile unites, send-out laboratory samples, age and disease specific out-patient centers are just some of the ways a society could buffer against the threat of a novel infectious disease or bio-warfare threat. Not to mention the need for innovative clinical research trial designs for rapidly repurposing drugs.
Dec 01, 2020
