Geert Vanden Bossche je pridobil svoj DVM na Veterinarski fakulteti v Ghentu in doktorat virologije na Univerzi v Hohenheimu v Stuttgartu. Po svojem postdoktorskem usposabljanju na področju virologije, imunologije in molekularne biologije na Free University of Berlin in Hohenheim v Nemčiji, je odšel v industrijo cepiv kot svetovalec za razvoj cepiv v GlaxoSmithKline Biologicals, Novartis Vaccines & Diagnostics in Solvay Biologicals. Nato se je pridružil Fundaciji Bill & Melinda Gates, da bi služil kot SPO pri Vaccine Discovery for Global Health. (GAVI) Bil je koordinator razvoja cepiva za Ebolo pri GAVI. Je ustanovitelj UNIVAC llc v ZDA in UNIVAC NV v Belgiji in je gostujoči znanstvenik na Inštitutu REGA, University of Leuven (Belgija). Geert Vanden Bossche je certificiran v virologiji in mikrobiologiji, avtor več kot 30 publikacij in izumitelj več patentnih prijav. Na več mednarodnih kongresih je predstavil teme, povezane s cepivi in adjuvanti. V nadaljevanju je predavanje, ki ga je dr. Bossche imel na vrhu o cepivih, ki je potekal od 1-3. marca 2021 v Ohio, ZDA. Naslov predavanja je: Zakaj cepiva za COVID-19 ne bi smela biti uporabljena za masovno cepljenje med pandemijo?
Bistvo je, da ne vidim, da masovno cepljenje ne bo vodilo v katastrofalno poslabšanje COVID-19 pandemije. Zdi se, da drugi tega ne opazijo. Namesto tega se strokovnjaki za cepiva, zdravniki in znanstveniki osredotočajo samo na pozitivne kratkoročne rezultate na individualnem nivoju. Nihče ne upošteva posledic in tveganj za človeško populacijo, ki se bodo po mojem razumevanju pojavile kmalu. Zakaj ni nihče zaskrbljen zaradi »imunološkega bega«, ko je COVID-19 že pobegnil človekovi prirojeni imunosti, kar se odraža v pojavu bolj nalezljivih inačic virusa (ki so verjetno nastale zaradi globalnih ukrepov za preprečevanje širjenja okužbe)? Uporaba cepiv za masovno imunizacijo bo zelo verjetno še povečala pridobljeni (adaptivni) imunski beg, ker nobeno od teh cepiv ne bo preprečilo replikacije/ transmisije virusnih inačic. Več cepiv bomo uporabljali za imunizacijo ljudi med pandemijo, bolj nalezljiv bo postal ta virus. S povečano nalezljivostjo se bo povečala tudi rezistenca virusa na cepiva. To je temeljno načelo, ki se ga učijo študentje v prvem letniku virologije: Ne sme se uporabljati v populaciji profilaktično cepivo med visoko nalezljivim pritiskom, ki se dogaja zdaj, ko se pojavljajo visoko nalezljive inačice virusa v mnogih delih sveta.
Za popoln pobeg selektivnemu imunskemu pritisku, ki ga vršijo protitelesa po cepljenju, mora visoko mutagen virus Covid-19 dodati samo še nekaj mutacij v svoji domeni, ki se veže na receptorje (v membrani celic) ...
*
*
Preveč sem zaskrbljen zaradi katastrofalnega vpliva, ki bi ga to imelo na našo človeško "raso". Ne samo, da bi ljudje izgubili zaščito, posredovano s cepivom, ampak tudi njihove dragocene, variantno nespecifične (!), prirojene imunitete ne bo več (to je zato, ker cepilna protitelesa nadvladajo naravna protitelesa za vezavo na virus Covid-19, tudi ko je njihova afiniteta do virusne inačice razmeroma nizka). Opozoril sem vse odgovorne zdravstvene in regulatorne organe, vključno s Svetovno zdravstveno organizacijo (WHO), Center za nadzor bolezni (CDC), Upravo za hrano in zdravila (FDA) itd. in prosil, da preučijo mojo zaskrbljenost in takoj začnejo razpravo o katastrofalnih posledicah, ki bi jih imel vsak nadaljnji imunski pobeg Covid-19. Seveda vem, da sedanje kampanje za množično cepljenje uživajo močno in svetovno podporo množice različnih strank/deležnikov. Vendar, razen če se ne dokaže, da se motim, to ne more biti izgovor za ignoriranje, da človeštvo trenutno spreminja precej neškodljiv virus v nekontrolirano pošast. Nikoli nisem bil tako resen glede izjave, ki sem jo podal.
- Profilaktična cepiva so za uporabo kot običajni profilaktični (preventivni) ukrep in NE med pandemijo
- Profilaktična cepiva je treba dajati pred nalezljivo izpostavljenostjo za zagotovitev popolne zaščite, preprečevanje poslabšanja bolezni (npr. Ebola cepljenje), za preprečitev imunskega bega in povečane nalezljivosti ter rezistence na cepiva – nekaj primerov hude oblike bolezni zaradi visoko nalezljivih inačih se je že pojavilo pri mlajših ljudeh
- Bilo je že več primerov popolnoma cepljenih ljudi s cepivom za Covid-19, ki so širili visoko nalezljive inačice virusa (nekateri so celo razvili blage simptome) Ali niso ti primeri dovolj prepričljivi, da pokažejo, kako lahko Covid-19 virusi zlahka pobegnejo gostiteljevi imuniteti? Splošno pravilo je: Replikacije virusov v okviru suboptimalnega imunskega odziva omogočajo imunski pobeg visoko mutagenih virusov
Trenutne tehnologije cepiva Covid-19:
• so usmerjene v indukcijo specifičnih protiteles (Abs) na S-beljakovine (S1- RBD), tako da nobeno cepivo ne preprečuje replikacije virusov, če je koncentracija protiteles premajhna ali imajo prenizko afiniteto do virusa
• ne morejo nadzirati replikacije bolj nalezljivih različic SARS CoV in lahko celo povzročijo imunski pobeg (npr. če so popolnoma cepljeni subjekti izpostavljeni virusnim variantam)
• niso varne za človeško populacijo, ki je izpostavljena pandemiji COVID-19 in niso učinkovite pri preprečevanju bolezni v populaciji, ki je izpostavljena pandemiji COVID-19
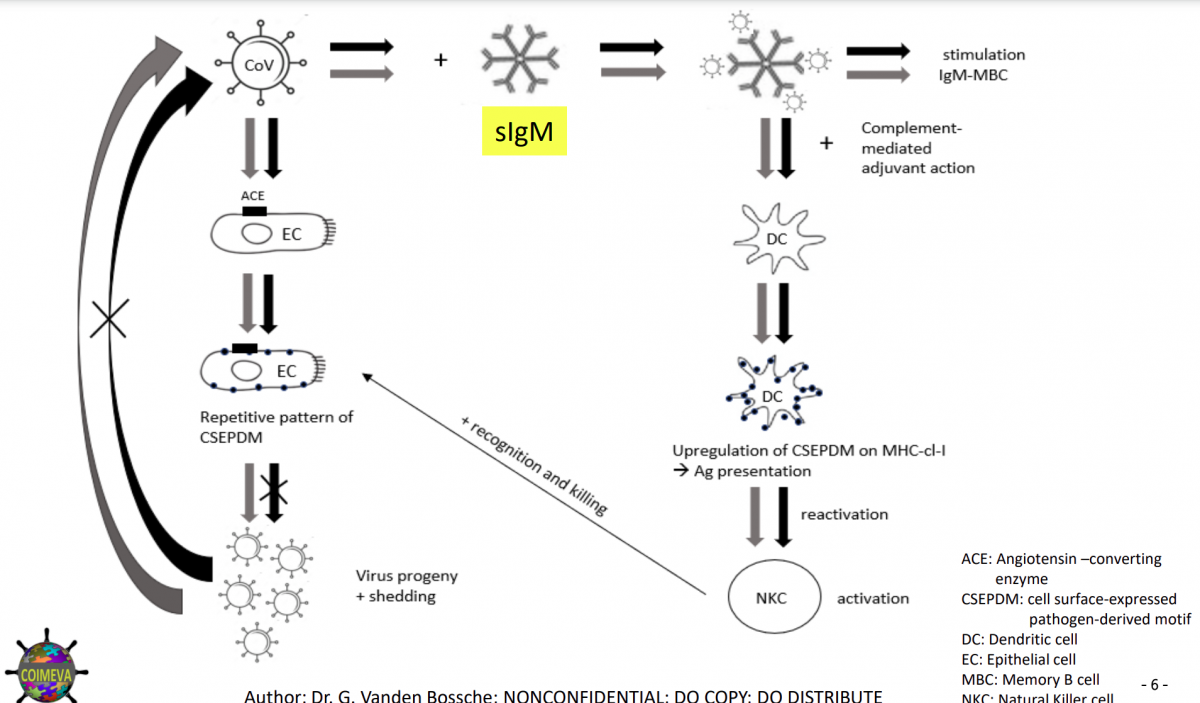
Naravni asimptomatični nosilci so subjekti, ki ne razvijejo kliničnih simptomov ali pa razvijejo blago obliko bolezni samo v zgornjih dihalih po primarni okužbi s korona virusi. Imajo naravna protitelesa (NABs) in celice naravne ubijalke (NK), ki dajejo naravno imunost z nespecifičnim ubijanjem antigenov. COVID-19 bolniki imajo šibko naravno/prirojeno imunost, to je šibko nevtralizacijo /ubijanje antigenov s pridobljenimi (adaptivnimi) protitelesi in so dovzetni za bolezen, ko antigenski titri izginejo.
Ker je replikacija virusov pri naravno asimptomatskih nosilcih pod nadzorom prirojenega imunskega sistema, virus lahko kompenzira izgubo možnosti replikacije/ transmisije tako, da poveča nelezljivost skozi selektiven imunski beg.
Stalni S-specifični titri protiteles zaradi cepljenja, bodo povzročili povečanje nalezljivosti virusa pri naravno asimptomatičnih nosilcih, dokler povratek pobeglih mutacij v simptomatskih nosilcih ne postane za virus relativno bolj ugoden.
Pobegle mutacije, specifične glede področja vezave na receptor (RBD), omogočajo virusu, da ustvari zadostno kapaciteto za replikacijo v simptomatskih osebah. Rezultat je imunski beg inačic virusa, ki so zdaj odporne na cepiva.
Povečana stopnja okužb/seropozitivnosti v naravno asimptomatskih in simptomatskih osebah podpira imunski pobeg. Povečana stopnja nalezljivosti vodi v povečano stopnjo seropozitivnosti v naravno asimptomatskih osebah.
Seropozitivnost zavira prirojeno naravno imunost, ker antigen-specifična protitelesa nadvladajo naravna protitelesa za vezavo na koronavirus v naravno asimptomatskihosebah in preprečijo šolanje naravnega imunskega sistema. Selektiven naraven imunski pobeg pri naravno asimptomatskih osebah vodi v povečano nalezljivost, kar vodi v selektiven prilagojen imunski pobeg pri simptomatskih osebah. (slika spodaj)
Množični ukrepi za preprečevanje širjenja okužbe in masovno cepljenje naravno asimptomatskih oseb pospeši prirojen imunski beg, pri čemer masovno cepljenje simptomatskih oseb pospeši prirojen in prilagojen/ pridobljen imunski beg.
Takojšnji preklic vseh tekočih kampanj za množično cepljenje proti COVID-19 bi moral postati zdaj najbolj nujna zdravstvena urgenca na mednarodnem nivoju.
Opomba prev.: Imunski pobeg onemogoča zdravilo Ivermectin, ki tudi preprečuje mutacije virusa SARS CoV-2. Vir: dr. Marc Wathelet, phD, Beligja min 50.00: https://www.youtube.com/watch?v=ypxrJhSg5xU
POVZETEK
Rokopis, ki je zdaj v postopku finalizacije, bi moral osvetliti, kako virus in zlasti njegova interakcija z imunskim sistemom gostitelja določa naravno smer (torej brez človeške intervencije) koronavirusne (CoV) pandemije. Prepletanje imunske obrambe gostitelja in virusnega imunskega pobega določa potek naravne CoV pandemije (vključno z naravno pandemijo COVID-19). Klinično je znano, da se virusni imunski pobeg pojavi, kadar nevtralizirajoča zmogljivost serumskih protiteles (Abs) ne zadošča za popolno odpravo visoko mutagenih virusov (npr. CoV) zaradi pomanjkanja njihove koncentracije ali afinitete.
V pandemični nastavitvi CoV se serokonverzija pojavi v ozadju visokega nalezljivega pritiska in je zato nagnjena k spodbujanju virusnega imunskega pobega. Prvi val bolezni (in umrljivosti) prizadene predvsem starejše osebe (ali kako drugače imunokompromitirane osebe). Selektivni (adaptivni/prilagodljivi) imunski pobeg naj bi povzročil prehod tega vala v hujši, drugi val v mlajših starostnih skupinah.
Posledično neselektiven (prirojen) in selektivni imunski pobeg vse bolj nalezljivih virusnih inačic sproži tretji val. Slednje bi vplivalo predvsem na osebe, ki so si opomogle po bolezni, ki so jih dobili med prvim valom, saj se njihove serumska neutralizirajoča protitelesa ne ujemajo več z novimi virusnimi inačicami v obtoku. Ta tretji val bolezni (in umrljivosti) bi se končal, ko bodo tisti, ki so si opomogli od bolezni, razvili nova funkcionalna protitelesa proti tem inačicam imunskega pobega.
Ker serokonverzija v tej populaciji zdaj pride veliko hitreje (zaradi odpoklica navzkrižno reaktivnih T spominskih celic pomagalk in ker bo večina mlade in srednje stare populacije bodisi seronegativna bodisi serokonvertirana že v času, ko se začne tretji val širiti, ima virus majhne možnosti da uide odzivu gostiteljevih protiteles.
Asimptomatski, seronegativni posamezniki (torej velika večina mladih in srednjih let) lahko širijo virus ob (ponovni) okužbi in s tem predstavljajo vir virusnega prenosa.
Vendar pa se okužba s koronavirusi pri teh asimptomatskih nosilcih po kratkem obdobju širjenja virusov ustavi. Virusno čiščenje pri teh osebah se lahko pojavi z aktivacijo NK celic naravnih ubijalk. Te lahko prepoznajo s koronavirusi povezane, antigensko nespecifične vzorce na površini epitelnih ciljnih celic, okuženih s koronavirusi.
Ker je ubijanje virusov s celicami naravnimi ubijalkami NK, zato ni antigen-specifično in je kot serokonverzija. Za namen rokopisa se "bolezen" nanaša na hudo bolezen COVID-19 z vključenimi nižjimi dihalnimi potmi. Za namen rokopisa se "asimptomatska" okužba nanaša na okužbo s koronavirusi, ki ne povzroča klinično pomembnih simptomov ali povzroča le blago obliko bolezni (to pomeni, da vključuje zgornje dihalne poti). Pri asimptomatsko okuženih osebah je bolezen le kratkotrajna, virusni imunski pobeg se običajno ne pojavi. Zato je malo verjetno, da bodo iz te populacije prihajale nove, bolj nalezljive variante virusa, dokler se virusna infekcija ne bo dramatično povečala.
Na točki "brez imunskega pobega" bo pandemija pod nadzorom in se bo spremenila v endemično okužbo. Vendar, dokler ni dosežena točka "brez imunskega pobega", bo vsak dodaten pritisk imunske selekcije, na primer zaradi suboptimalne koncentracije ali afinitete antigen-specifičnih protiteles (npr. specifičnih za beljakovinske bodice), omogočil, da bo virus hitro povzročil še več okužb z inačicami imunskega pobega.
Dodatni imunski selektivni pritisk, še posebej, ko se izvrši med drugim valom CoV pandemije, bo lahko manifestiral in okrepil virusni imunski pobeg. To bi lahko celo povzročilo, da se drugi in tretji val združita v en sam ogromen val umrljivosti in bolezni, ki bi prizadel vse skupine prebivalstva (morda z izjemo majhnih otrok). Zlasti kampanje množičnega cepljenja, zlasti kadar se izvajajo sredi pandemije, so nagnjene k izvajanju ogromnega imunskega pritiska na seve virusov v obtoku.
To je zato, ker se cepivo uporablja v vse bolj nalezljivem kontekstu (saj so variante virusnega pobega bolj nalezljive). Množične kampanje cepljenja bodo pospešile nastanek še bolj nalezljivih variant imunskega pobega. To je zato, ker se bo število prejemnikov cepiva, ki se v določenem časovnem obdobju serokonvertirajo, dramatično povečalo . Poleg tega bodo antigen-specifična, visoko afinitetna protitelesa, ki jih povzroči katero koli trenutno cepivo, premagala naravna, široko spektralno zaščitna mukozna protitelesa IgM, saj se slednja vežejo le z nizko afiniteto na receptor- vezujočo-domeno koronavirusa (RBD).
To bo še posebej vplivalo na naravno odpornost mlajših starostnih skupin, ki so se - zaradi dobro usposobljenega naravnega imunskega sistema- med prvim valom uspešno uprle bolezni. Nove variante koronavirusa v obtoku lahko zdaj celo pobegnejo gostiteljevi nespecificni liniji imunske obrambe na sluznici vstopa inačice koronavirusa. Te starostne skupine lahko zato postanejo bolj dovzetne za simptomatsko okužbo in širjenje virusa zaradi bolj nalezljivih variant.
Množične kampanje cepljenja pa bodo imele tudi hude posledice za tiste, ki so se prvi cepili (večinoma starejše ali osebe s pridruženo boleznijo ali tiste, ki so sicer imunokompromitirani). V zelo verjetnem primeru, da bo množično cepljenje kmalu povzročilo protivirusno odpornost (glejte spodaj), ti ljudje ne bodo imeli niti enega delca imunosti, na katerega bi se lahko zanašali. V nasprotju z nalezljivim virusom v obtoku, trenutna cepiva ne vsebujejo nobenega kritičnega motiva ubijalskih celic ali pa ne aktivirajo namenskih ubijalskih celic.
Zato bodo imunski odzivi, ki jih povzroči cepivo, neizogibno povzročili dramatično povečanje stopnje obolevnosti in umrljivosti v vseh skupinah človeške populacije (razen majhnih otrok?)
Poleg vsega navedenega bo nizka izpostavljenost sevom koronavirusa v obtoku (npr. zaradi strogih ukrepov zadrževanja širjenja virusa) vse bolj oslabila prirojeno naravno imunost sluznic zaradi pomanjkanja usposabljanja. To je še posebej pomembno za tiste, ki so se zaradi zadostne in ustrezne imunske obrambe v prvem valu izvlekli z asimptomatsko okužbo. Strogi in razširjeni ukrepi za preprečevanje okužb zdaj vse bolj ogrožajo njihovo prirojeno naravno imuniteto in jih s tem naredi še bolj dovzetne za simptomatsko okužbo.
Predvsem mlajše starostne skupine lahko zato končajo z razmeroma višjo stopnjo obolevanja in umrljivosti, tudi ne glede na pojav bolj nalezljivih virusnih variant. To pomeni, da bodo široko izvedeni ukrepi za preprečevanje okužb le še okrepili že tako škodljive posledice tekočih kampanj za množično cepljenje. Razumno je predpostavljati, da bo kombinacija neselektivnega in selektivnega imunskega pobega povzročila eksplozijo obolevanja in umrljivosti v mlajših starostnih skupinah (glejte sliko, priloženo na str.6 spodaj).
Bolj kot bo cepljenje za COVID-19 v mladih in srednjih skupinah populacije zamujalo (glede na uporabo cepiv pri starejših), bolj bo to povečalo umrljivost in smrtnost v mlajših skupinah: do začetka masovnoga cijepljenja u mlajših skupinah populacije, bo veliko teh ljudi že okuženih s COVID-19
Povečane stopnje okužbe z visoko nalezljivo virusno različico so zdaj znatno povečale verjetnost, da se ponovno okužijo, medtem ko so v procesu serokonvertiranja. Tako bo do začetka cepljenja v mlajših starostnih skupinah, virusni imunski pobeg v tej skupini že podžigal začarani krog povečane virusne infekcije, ki povzroči več serokonverzije in s tem več imunskega pobega.
Množične kampanje cepljenja v tej skupini bodo le dramatično poslabšale razmere, saj bodo povzročile hitro in množično povečanje števila asimptomatskih oseb, ki so v procesu serokonvertiranja v zelo nalezljivem ozadju in so zato podvržene spodbujanju virusnega imunskega pobega. Ker seveda ni razloga za njihovo izolacijo, bo veliko priložnosti, da se zelo nalezljivi, sevi v obtoku replicirajo v prisotnosti suboptimalnih titrov protiteles in zato uidejo imunskemu nadzoru gostitelja.
Zato, bolj bo kampanja za cepljenje v tej skupini zamujala, hitrejša bo selekcija še bolj nalezljivih virusnih variant. Eksponentno povečanje stopenj virusnega imunskega pobega bo na koncu omogočilo virusnim variantam celo preboj s cepivom posredne zaščite pri cepljenih starejših osebah. Ker so njihova protitelesa vedno manj skladna z vedno bolj nalezljivimi nastajajočimi variantami virusa, jim ne bo več uspelo nadzorovati virusne replikacije in širjenja virusa ter bodo hitro omogočili množični virusni imunski pobeg.
Ker serumska zaščitna protitelesa v prvi vrsti nudijo zaščito s ciljanjem na COVID-19 domeno za vezanje na receptor (RBD), bo virus zdaj vedno bolj izbiral mutacije v tem določenem delu beljakovinske bodice, saj takšne mutacije najhitreje omogočajo virusu pobegniti protitelesom, ki nastanejo s cepljenjem. To bo nedvomno povzročilo odpornost na cepivo.
Zaradi množičnega cepljenja ljudje, ki so prej dobili cepivo, nenadoma ne bodo več zaščiteni in kljub cepljenju bodo postali žrtev katastrofalne obolevnosti in umrljivosti. Zato ni dvoma, da sedanje strategije cepljenja še bolj katastrofalno vplivajo na kampanje množičnega cepljenja in le še večjo razsežnosti svetovne zdravstvene katastrofe.
Vendar pa množično cepljenje škoduje tudi zdravju posamznika, saj bodo protitelesa, ki jih povzroči cepivo, premagalo naravna variantno nespecifična mukozna protitelesa za vezavo na CoV variante in s tem prikrajšajo posameznike za njihove široko zaščitne naravne (življenjske) linije imunske obrambe. Ker bodo obsežne kampanje cepljenja v kombinaciji s trajnim izvajanjem več ukrepov zadrževanja le pospešile pojav mutacij virusnega pobega, je iluzorno upanje, da bi sedanja cepiva proti COVID-19 lahko ustvarila čredno imunost.
Glede na to lahko sklepamo, da bi COVID-19 lahko ponovno prečkal ovire med vrstami. Ne moremo izključiti, da bi zaradi imunsko posredovane imunosti COVID-19 lahko skočil na druge živalske vrste, zlasti na industrijsko gojene črede (npr. na intenzivnih farmah svinj in perutnine z visoko gostoto živali), saj je znano:
1. da te vrste že gostijo več različnih koronavirusov
2. da so variabilnosti/mutacije v beljakovinski bodici in zlasti v domeni receptorske vezave (RBD) odgovorne za spremembe v tropizmu/ dovzetnosti gostiteljev.
Podobno kot pri virusu gripe bi lahko te živalske vrste nato predstavljale rezervoar za virus SARS-COVID-2. Glede na razširjenost živalskih koronavirusov v obtoku na teh kmetijah (in raven usposobljene imunitete) bi te živali potem lahko služile kot asimptomatske prenašalke virusa, s čimer bi predstavljale resno grožnjo za ljudi.
Zaključek:
Kombinacija ukrepov za množično cepljenje in preprečevanje okužb je recept za svetovno zdravstveno katastrofo.
V skladu z znanostjo je treba zaključiti, da bodo vse starostne skupine (morda z izjemo majhnih otrok) močno prizadete in podvržene vse večjim stopnjam obolevnosti in umrljivosti, ki bodo veliko višje od tistih, ki naj bi se pojavljale med naravnim potekom pandemije COVID-19. To bo še posebej veljalo, če bo zaporedje množičnih cepljenj po prvem nalezljivem valu vzporedno z naravnimi okužbami (to so najprej imunsko kompromitirani ljudje in starejši, ki jim sledijo mlajše starostne skupine).
Nikomur glede na to, ne bi smela biti podeljena pravica do izvajanja obsežnih farmacevtskih in nefarmacevtskih imunskih posegov, zlasti ne med virusno pandemijo, vsekakor pa ne brez poglobljenega razumevanja imunske patogeneze virusne pandemije. Ko sledimo znanosti, in nič drugega kot znanosti, postane zelo težko ne označiti množičnega cepljenja kot kaznivo dejanje, ne samo za javno zdravje, ampak tudi za individualno zdravje.
Da bi se obrazložilo zgoraj navedeno, bo v rokopisu najprej pojasnjeno, kako lahko sestavine prirojenega naravnega imunskega sistema ščitijo pred COVID-19 in naredijo okužbe asimptomatične. Nato bom podrobneje razložil, zakaj in kako, v imunološko COVID-19 naivni populaciji, selektivni (adaptivni) imunološki beg obrne prvi val okužbe in smrti od starih (in imunokompromitiranih) ljudi na tiste, ki so na začetku pandemije imeli asimptomatske okužbe (npr. segment populacije mlajših in srednje starih ljudi).
Podobno bo pojasnjeno, kako pospešen virusni imunski pobeg v asimptomatsko okuženi populaciji na koncu usmeri izbruh obolevanja in umrljivosti na starejše in kako prebivalstvo sčasoma nadzoruje pandemijo z nadzorom virusnega imunskega pobega. To bo ponazorilo kritični pomen spreminjajočega se prispevka prirojene naravne in pridobljene (adaptivne) imunitete na splošno imunsko obrambo prebivalstva pred virusno pandemijo.
Razumevanje te dinamike pomaga dojemati prefinjen potek naravne pandemije koronavirusa, kako se sčasoma združi v endemično okužbo in zakaj ima človekova intervencija zelo škodljiv vpliv na rafinirano prepletanje med virusom in gostiteljem. Kar zadeva slednje, bodo bolj podrobno pojasnjeni uničujoči vplivi tekočih kampanj za množično cepljenje na svetovno zdravje ter spremljajoči strogi in razširjeni ukrepi zadrževanja bodo bolj podrobno pojasnjeni, saj bodo lahko globalne in individualne zdravstvene posledice v prihodnjih letih preprosto neznosne.
Po uvodnem delu o prirojenih naravnih mehanizmih imunske obrambe, pomembnih za COVID-19, bodo obravnavane druge ustrezne teme v obliki vprašanj in odgovorov. Nazadnje, eno poglavje bo posvečeno znanstvenemu razlogu za uporabo cepiv, ki temeljijo na celicah naravnih ubijalkah (NK), ki bi lahko zagotovila sterilizacijsko imuniteto in s tem v celoti izbrisala COVID-19 in sorodne različice.
* * *
Dr. Geert Vanden Bossche, DMV, neodvisni virolog in strokovnjak za cepiva, nekdaj zaposlen pri GAVI in fundaciji Bill & Melinda Gates.
Vsem oblastem, znanstvenikom in strokovnjakom po vsem svetu, ki jih to zadeva: celotni svetovni populaciji.
Sem vse prej kot anticepilec. Kot znanstvenik se običajno ne obračam na tovrstne platforme, da bi zagovarjal teme, povezane s cepivi. Kot zavzeti virolog in strokovnjak za cepiva naredim izjemo le, kadar zdravstveni organi dovolijo cepljenje na načine, ki ogrožajo javno zdravje in seveda če se znanstveni dokazi prezrejo. Trenutna skrajno kritična situacija me sili, da razširim klic v sili. Z nezaslišanim človeškim posredovanjem v pandemiji Covid-19 zdaj tvegamo, da bomo povzročili neprimerljivo globalno katastrofo, zato ta poziv ne more zveneti dovolj glasno in odločno.
Kot rečeno, nisem proti cepljenju. Nasprotno. Lahko vam zagotovim, da so vsa sedanja cepiva ustvarili, razvili in izdelali briljantni in kompetentni znanstveniki. Vendar so te vrste profilaktičnih cepiv popolnoma neprimerne in celo zelo nevarne, če jih uporabljamo za množično cepljenje med virusno pandemijo. Vakcinologi, znanstveniki in zdravniki so zaslepljeni zaradi pozitivnih kratkoročnih učinkov pri posameznih bolnikih, vendar se zdi, da jih ne skrbijo katastrofalne posledice za globalno zdravje. Težko je razumeti, kako bodo človeške intervencije preprečile, da se različice virusa, ki krožijo, ne bodo spremenile v divjo pošast, razen če se mi znanstveno dokaže, da se motim.
Tekmujem s časom, ko dokončujem svoj znanstveni rokopis, katerega objava bo na žalost verjetno prepozna glede na vedno večjo grožnjo zaradi hitrega širjenja zelo nalezljivih različic. Zato sem se odločil, da na Linkedinu objavim povzetek svojih ugotovitev in svojega osrednjega govora na nedavnem vrhu o cepivih v Ohiu. Prejšnji ponedeljek sem mednarodnim zdravstvenim organizacijam, vključno s SZO, priskrbel analizo trenutne pandemije, ki temelji na znanstveno utemeljenih spoznanjih o imunski biologiji Covida-19. Glede na stopnjo nujnosti sem jih pozval, naj upoštevajo moje pomisleke in sprožijo razpravo o škodljivih posledicah prihodnjega "virusnega imunološkega pobega". Za tiste, ki niso strokovnjaki na tem področju, prilagam spodaj bolj dostopno in razumljivo verzijo, v kateri opisujem ta zahrbtni pojav.
Čeprav ni več časa na razpolago, do zdaj nisem prejel povratne informacije. Strokovnjaki in politiki molčijo, medtem ko so očitno še vedno pripravljeni govoriti o pravilih sproščanja za preprečevanja okužb in "spomladanski svobodi". Moje izjave temeljijo na ničemer drugem kot na znanosti. Nasprotovala jim bo samo znanost. Medtem ko lahko človek komajda izreče kakšno nepravilno izjavo, ne da bi ga vrstniki kritizirali, se zdi, da znanstveniki iz elite, ki trenutno svetujejo našim voditeljem, raje molčijo. Predloženo je bilo dovolj znanstvenih dokazov. Na žalost po njih ne posežejo tisti, ki imajo moč ukrepati. Kako dolgo lahko ignoriramo problem, ko obstajajo množični dokazi, da virusni imunološki pobeg ogroža človeštvo? Težko rečemo, da nismo vedeli - ali pa nas niso opozorili.
* * *
https://www.youtube.com/watch?v=ZJZxiNxYLpc
Mass Vaccination in a Pandemic - Benefits versus Risks: Interview with Geert Vanden Bossche
* * *
Del Bigtree o dr. Bossche 11.3. 2021
https://www.facebook.com/VaXismVideos/videos/137654238255968
*
https://www.logicno.com/politika/114301.html?fbclid=IwAR0g8Q_NRBVsihY4hNbeO2b4MJzVNx1usdJhjwN4JZrkO8ZW4NJwgZXl6o8
*
dr. Vernon Coleman o načrtu depopulacije in pomenu razkritja dr. Bossche-ja
https://www.bitchute.com/video/ZKoBCtrNvSoB/
*
*
https://childrenshealthdefense.org/defender/rebuttal-rosemary-frei-bossche-vaccination-concern/
* * *
A NEW MUTATION THREATENS A FRAGILE RECOVERY
Posted by Adam Gaertner | Mar 7, 2021
When I first looked at the virus, I saw something horrifying[1]. Deadly, permanent, recurring, and as contagious a disease as the Earth ever had witnessed. From that point forward, I dedicated my time to finding, and sharing, treatments and cures, for the preservation and life of all humanity. Little did I know then of the enormous powers lined up against us[2].
Fortunately, as the work of some great leaders in medicine eventually discovered[3] and told the world[4], the infection was not to be permanent, Herpes-like, after all. An overlooked aspect of our immune system, namely CD8+ T-cells, provided an immunity of last resort, against a virus that was otherwise comprehensively cloaked against immune detection.
We have now lost that luxury[5].
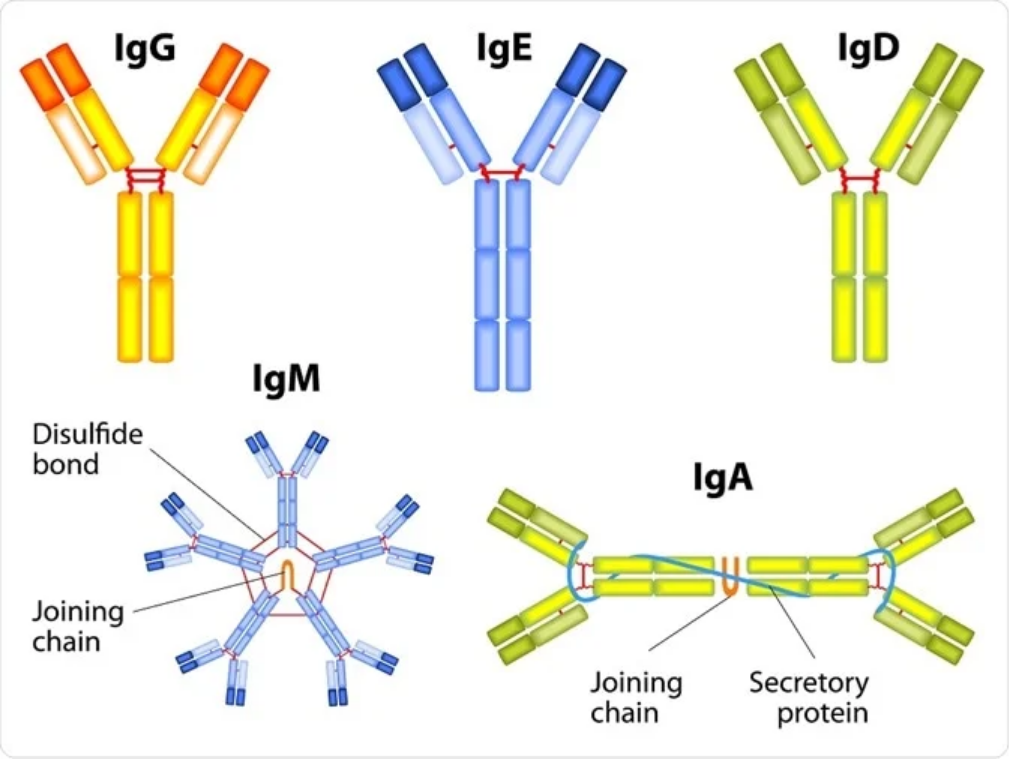
To begin this article, I should first explain to you, briefly, some various types of immunity that we are possessed of. Each of them plays an important role, and each of us have slight differences that affect our susceptibility to infection, morbidity and death.
Broadly, I will describe the first category of immunity, innate immunity[6]. This covers such immune cells as macrophages, neutrophils and others. These are blunt force instruments, responding to cytokine and complement signals of infection early in the process[7] to phagocytose foreign pathogens, signal infected cells to destroy themselves, activate stronger immune responses, and release cytotoxic chemical soup to mechanically destroy infected cells, also catching uninfected cells in the crossfire.
The second category, as you probably know, is adaptive immunity. This is, broadly, the antibody response. It is mediated by dendritic cells, CD4+ T-cells and B cells among others, which capture proteins from phagocytosed virions, study them, and by a process of trial and error, produce antibodies which bind to the recognized protein fragments. When a live pathogen that matches a previously processed protein is detected, the body releases a flood of antibodies. Those antibodies bind to the pathogen and act as hooks to enable macrophages to more easily destroy the pathogen. This form of immunity is largely irrelevant to this discussion.
The third category, very minimally described in the literature as a cohesive field, is cytosolic immunity[8]. This covers such intracellular detection and defense mechanisms as toll-like receptors, interferon-stimulated genes, endolysosomes[9] and protein kinases[10]. These form an integral link in the various mechanisms which activate the broader immune system, and it is here that our problem begins.
MHC stands for major histocompatibility complex[11], of which there are two kinds, MHC-I and MHC-II. When a cell is infected, and cytosolic sensors detect it in the endosome upon infection, the endosome fuses with a lysosome to become an endolysosome[12], MHC proteins being produced in the endoplasmic reticulum[13], and the nucleus begins producing interferon to warn neighboring cells to be on guard for infection. The viral protein is dissolved into chunks, and MHC-I is transported into the endolysosome[14]. This protein attaches to those chunks of viral protein, and carries them to the surface, where T-cells can bind to it and obtain a sample of the viral protein to begin building immunity (when this fails, it’s a problem[15].) MHC-I also acts as a binding site for effector CD8+ T-lymphocytes[16]. Upon binding to an MHC-I protein on the surface of an infected cell, the effector CD8+ cell will then destroy the cell. This action is of vital importance to the clearing of COVID-19 infection, as via the ACE2 receptor[17], the virus infects immunoprivileged cells[18] that no other component of the immune system is permitted to attack[19]. This mechanism evolved in order to protect us from our immune system damaging critically important and irreplaceable parts, such as nerves and gonads[20].
Stepping back: The SARS-CoV-2 virus uses the importin alpha-beta complex to import the ORF6 protein into the cell nucleus[21], which interferes with the action of MHC-II, among others[22]. This is one aspect of its cloaking function – the other being glycosylation of antigens[23] – which interfere with antibody recognition and binding, and prevents a cell from releasing interferon particles[75] to warn its neighbors to defend against imminent infection[24]. This delays, but does not prevent, the formation of adaptive immunity.
MHC-I has, until this time, been only mildly downregulated in this process, which has enabled clearance of infected, immunoprivileged cells via cytotoxic CD8+ T-lymphocyte interaction, and made vitamin D3 a very useful adjunct[25] in the treatment of COVID-19, due to its effect increasing the number of effector CD8+ cells[26], enabling more rapid and thorough clearance of infected cells.
New research[5], however, has identified a mutation of SARS-CoV-2 which is now able to escape the grasp of MHC-I in the endolysosome, and thus impair the cell surface presentation of MHC-I protein. The viral protein has simply mutated, by random evolutionary chance, very likely under hyper-evolutionary pressure from vaccine-induced IgG and IgM antibodies[27], such that it is possessed of a shape that the protein complex is unable to grasp and hold. The presence of such antibodies in the blood impairs the ability of the virus to spread from an infected cell, but they do not target the infected cells themselves; only the cell’s presentation of MHC-I is able to identify it as infected and cause it to be targeted for destruction. Without being able to present MHC-I, immunoprivileged cells may remain permanently infected[28], budding out endless virions[29] (rather than bursting their host cell – an important distinction), keeping the body in a hyper-immune state[31] and causing as yet unknown pathologies.
The implications of this are potentially far reaching. ACE2-mediated infection of immunoprivileged cells, very uncommon for viruses, means that cytotoxic CD8+ T-lymphocytes are the only means, aside from incredibly damaging and indiscriminate cytokine storms[30], by which infected immunoprivileged cells can be either instructed to self-destruct or be mechanically destroyed. Without this mechanism, and considering that the viral proteins ORF8, ORF6 and ORF3b already inhibit interferon and MHC-II production inside the cell[32], and that there are multiple N-linked glycosylation sites on the spike protein[33], which cloak the virion in sugar to protect it from antibody recognition and binding[23] – we may no longer have any available means to naturally clear an infection without therapeutic intervention.
This would be bad news, but not the worst news, if our medical system wasn’t so hopelessly incompetent and corrupt that extraordinarily useful therapeutics such as ivermectin are pushed by the wayside, lied about in media[34-37], and suffer in reputation from the concoction of fake science[38] and rigged trials[39] by the pharmaceutical interests that apparently wish to prolong the pandemic as long as possible[40]. Unfortunately, our medical system is hopelessly incompetent[41] and corrupt[42]. The consequences of this mutation will be dramatically amplified by our utterly insane “wait and see” policies against early treatment[43], which will likely manifest in a dramatic acceleration of COVID-related hospitalizations, closures, lockdowns, and of course a renewed emphasis on mass vaccination.
From the point of view of the COVID-19 disease itself, what we may begin seeing in patients will be much more in line with what we saw very early on in the pandemic. With the virus perpetually present inside immunoprivileged cells, and still in possession of the gp120 HIV spike protein[44], it is highly likely that CD4+ depletion[45], cytokine storms and pneumonia will occur in a much higher proportion of patients. There are also likely to be more deleterious effects in the brain[46] as CD4+ cells pyropoptose[47] in response to[48] CD4 receptor binding[49], which is a classic symptom of late-stage AIDS[50]. Recoveries will take longer, and while steroids, blood thinners and targeted immunotherapies such as tocilizumab may be able to temporarily ameliorate symptoms, the use of effective antivirals will become absolutely mandatory.
It is ironic that this mutation is highly likely, although by no means proven, to have resulted from hyper-evolutionary pressures applied by vaccines. The presently available vaccines, to their credit, appear to be mostly effective in the prevention of severe disease and mortality – for now. These vaccines work by providing IgG and IgM, but not IgA antibodies[51]. This is a crucial shortcoming; IgA antibodies reside in epithelial tissues and prevent initial infection[52], whereas IgG and IgM antibodies patrol the blood[53] and attack free virions, reducing the innate inflammatory immune response and inhibiting further spread of the virus throughout nearby tissues. However, without destroying infected cells, this simply means that the virus is remaining in place, replicating and mutating. Eventually, a random mutation occurs which allows the virus to evade those IgG and IgM antibodies, and by virtue of then becoming able to spread, that virus is quickly selected by evolution and becomes the dominant strain[27]. As CD8 has been the primary mechanism by which infected cells are destroyed, the virus’ evasion of MHC-I and CD8 immunity is likely an evolutionary response to being trapped in a cell and eventually destroyed; now, the host cells will no longer be destroyed.
This is not a unique scenario. Marek’s disease, a lymphoma virus disease in chickens, is the best known example of leaky vaccines causing evolutionary escape[54]. Long story short, the original virus was relatively mild, until flocks of chickens were vaccinated with leaky vaccines that, while preventing the chickens from dying, did not prevent infection. The virus engaged in an evolutionary arms race against the vaccines, which required frequent updates, and became more infectious and lethal over time. Eventually, the virus became so lethal that any unvaccinated chicken was certain to die if infected; the vaccine became the only means by which a flock of chickens could expect to survive an outbreak.
Humanity is at a crossroads. If we continue mass vaccination with these half-measure vaccines, we will see more, more infectious and deadlier strains of SARS-CoV-2 evolve. It is not a question of if; it is a question of when. Unlike other times in history, we are fortunate enough to have discovered a plentiful, extraordinarily safe and effective therapeutic[55-68], in ivermectin (among a number of other very promising therapeutics.) Ivermectin is, for a variety of reasons,[21,69-72] highly unlikely to cease being curative, without concerted and deliberate effort to engineer gain of function into a new virus. The people that think they’re being responsible and contributing to “herd immunity” – they are not. The only benefit of the vaccines is that they will likely, temporarily, protect from severe disease and mortality[73], until the next strain emerges. Ivermectin can also accomplish this, with a far lower risk profile, and without inducing an evolutionary arms race against the virus. It has been endorsed and put into practice by many governments, to great results; others, including our own, are actively sabotaging it, publishing fake trials, fake news, and fear, just as was done to HCQ.
The people that have been buying the official story all along – the mask Karens, the Fauci fans, the hopelessly suckered TV watchers – they, generally, are the ones most eager and likely to be vaccinated. While their sanctimonious disrespect for the work of many of the most skilled scientists and doctors in the world has cost many lives, mostly it has just been their own, having failed to study what works, and finding themselves at the mercy of our corrupt medical system. By adhering to religious scientism, failing to even acknowledge what the authorities have fully admitted about the potential for harm, and by taking the vaccines, they are now becoming an active danger to our collective health and well being. The vaccinated people, slowly gaining their own special status with vaccine passports, reserved beach seats and God knows what else is coming – they are Typhoid Maries, creating and cementing the existence of an ever-increasingly deadly disease in our midst, and dooming everybody to death, vaccinated or not, when eventually the latest shot can no longer prevent the horrifying disease of this hyper-evolved bioweapon. We must educate those people, and we must do it soon, because our health authorities are not about to abort the multi-billion dollar push for widespread vaccination. Effectively, the people who have been vaccinated are those who society most needs to now adopt pre-exposure prophylactic protocols with the antiviral drug of their choice; they are the ones incubating and spreading deadly disease, not the unvaccinated.
This is still in the early stages. We are now starting to see mutations such as this emerge. More vaccines to counter them will follow, and deadlier, harder to treat strains will follow those. We must break this cycle now. Support the use of ivermectin. Tell your friends, family, colleagues, communities, doctors, local governments, and anybody else that will listen, that we have an alternative to this incipient hellscape. Buy an ivermectin shirt, hat or mask – it won’t be quickly forgotten! Take your local health authority to court and obtain a declaration that ivermectin is an effective treatment under Section 564 of the FDA Act[74]. Whatever you can do, now is the time to start doing it.
Time is rapidly running out.
A note of optimism: in the beginning of the pandemic, the scenario described above was precisely what was feared. The crucial impact of effector CD8+ T-cells was completely overlooked, which brought mortality and morbidity significantly down, and allayed fears of permanent, recurring infection. With the loss of CD8 function, the situation does look grim; however, as with any mutation, we do not yet fully understand it, and the evolutionary tradeoff necessary for this new cloaking function may have resulted in the loss of another function, enabling an as-yet unknown mechanism to still effect clearance. Millions of years of evolution have made us pretty resilient. Let’s hope this just turns out to be another blip on the radar.
https://covidcandy.net/coronavirus/a-new-mutation-threatens-a-fragile-recovery/?fbclid=IwAR1roXbOUcYyGKhrqkvTanPhu7O0I0MFyz0CpdDgQNIaZcTcVRPXqObJu7E
*
https://ambasador21.wordpress.com/2021/03/18/top-znanstvenik-za-cepiva-opozarja-svet-ustavite-vsa-covid-19-cepljenja-takoj-ali-pa-bo-spuscena-neobvladljiva-posast/
*
Prevod pogovora med Del Bigtree in dr. Bossche:
https://www.facebook.com/anastazija.zvonkicedarruski/videos/3651219818339491
*
FB 10.4. 2021
*
Vaccine manufacturer Merck has abandoned development of two coronavirus vaccines, saying that after extensive research it was concluded that the shots offered less protection than just contracting the virus itself and developing antibodies.
*
https://www.brighteon.com/536a0e60-9b86-442f-8546-d2cc0d89ad71
Intervju z dr. Bossche-jem
*
Dr. Bossche opozarja:
https://www.facebook.com/viktor.jagarinec/videos/2952488461690273
*
Nobel Prize winner: Mass COVID vaccination an ‘unacceptable mistake’ that is ‘creating the variants’
May 19, 2021 (LifeSiteNews) – French virologist and Nobel Prize winner Luc Montagnier called mass vaccination against the coronavirus during the pandemic “unthinkable” and a historical blunder that is “creating the variants” and leading to deaths from the disease.
“It’s an enormous mistake, isn’t it? A scientific error as well as a medical error. It is an unacceptable mistake,” Montagnier said in an interview translated and published by the RAIR Foundation USA yesterday. “The history books will show that, because it is the vaccination that is creating the variants.”
Many epidemiologists know it and are “silent” about the problem known as “antibody-dependent enhancement,” Montagnier said.
“It is the antibodies produced by the virus that enable an infection to become stronger,” he said in an interview with Pierre Barnérias of Hold-Up Media earlier this month.
Vaccination leading to variants
While variants of viruses can occur naturally, Montagnier said that vaccination is driving the process. “What does the virus do? Does it die or find another solution?”
“It is clear that the new variants are created by antibody-mediated selection due to the vaccination.”
Vaccinating during a pandemic is “unthinkable” and is causing deaths, the winner of the 2008 Nobel Prize in Medicine for discovery
‘Deaths follow vaccination’
“The new variants are a production and result from the vaccination. You see it in each country, it’s the same: in every country deaths follow vaccination,” he said.
A video published last week on YouTube uses data from the Institute for Health Metrics and Evaluation at the University of Washington to illustrate the spikes in deaths in numerous countries across the globe after the introduction of COVID vaccination, confirming Montagnier’s observation.
https://www.youtube.com/watch?v=KrIoPIQZmUE
The French interviewer pointed to data from the World Health Organization (WHO) showing that since the vaccines were introduced in January, new infections contamination have “exploded,” along with deaths, “notably among young people.”
“Yes,” agreed Montagnier who is a professor at Shanghai Jiao Tong University. “With thrombosis, etc.”
Thrombosis – or blood clots — have been an unexpected problem linked to the new coronavirus vaccines and the cause of AstraZeneca’s vaccine being pulled in several countries. The head of Canada’s public health agency, Theresa Tam, told a press conference Tuesday that there are now 21 confirmed cases of vaccine-induced thrombotic thrombocytopenia, or VITT, including among three women who died from the blood-clotting disorder potentially linked to AstraZeneca’s vaccine and another 13 cases are under investigation.
Breakthrough cases
Montagnier said that he is currently conducting research with those who have become infected with the coronavirus after getting the vaccine. The Centers for Disease Control and Prevention reported in April that it had received 5,800 reports of people who had “breakthrough” COVID after being vaccinated, including 396 people who required hospitalization and 74 patients who died.
“I will show you that they are creating the variants that are resistant to the vaccine,” Montagnier said.
Coronavirus made in a lab
The famous French virologist created waves in April 2020 when he told a French television station that he believed SARS-CoV2, the new pandemic coronavirus, was man-made in a laboratory. The “presence of elements of HIV and germ of malaria in the genome of coronavirus is highly suspect and the characteristics of the virus could not have arisen naturally,” he said.
Though he was ridiculed by French experts for having “a conspiracy vision that does not relate to the real science,” Montagnier published a paper in July 2020 supporting his claims that the novel coronavirus must have originated from human experimentation in a lab – a theory that has recently resurfaced and is currently considered the most likely origin of the virus.
*
Vodilna francoska strokovnjakinja za cepiva je potrdila trditve dr. Bossche-ja, da cepiva za COVID-19 povzročijo mutante SARS CoV-2 in virusni pobeg (18.00 min)
https://www.youtube.com/watch?v=UNjaRWfwz1Q
Svetovna strokovnjakinja za cepiva, dr.Alexandra Henrion-Caude
*
In conclusion, in the context of the rushed emergency-use-authorization of SARS-CoV-2 vaccines, and the current gaps in our understanding of their safety, the following questions must be raised:
- Is it known whether cross-reactive antibodies from previous coronavirus infections or vaccine206 induced antibodies may influence the risk of unintended pathogenesis following vaccination with COVID-19?
- Has the specific risk of ADE, immunopathology, autoimmunity, and serious adverse reactions been clearly disclosed to vaccine recipients to meet the medical ethics standard of patient understanding for informed consent? If not, what are the reasons, and how could it be implemented?
- What is the rationale for administering the vaccine to every individual when the risk of dying from COVID-19 is not equal across age groups and clinical conditions and when the phase 3 trials excluded the elderly, children and frequent specific conditions?
- What are the legal rights of patients if they are harmed by a SARS-CoV-2 vaccine? Who will cover the costs of medical treatment? If claims were to be settled with public money, has the public been made aware that the vaccine manufacturers have been granted immunity, and their responsibility to compensate those harmed by the vaccine has been transferred to the tax-payers?
In the context of these concerns, we propose halting mass-vaccination and opening an urgent pluralistic, critical, and scientifically-based dialogue on SARS-CoV-2 vaccination among scientists, medical doctors, international health agencies, regulatory authorities, governments, and vaccine developers. This is the only way to bridge the current gap between scientific evidence and public health policy regarding the SARS-CoV-2 vaccines. We are convinced that humanity deserves a deeper understanding of the risks than what is currently touted as the official position. An open scientific dialogue is urgent and indispensable to avoid erosion of public confidence in science and public health and to ensure that the WHO and national health authorities protect the interests of humanity during the current pandemic. Returning public health policy to evidence-based medicine, relying on a careful evaluation of the relevant scientific research, is urgent. It is imperative to follow the science.
1 https://www.gov.uk/government/publications/covid-19-reported-sars-cov-2-deaths-in-england/covid-19-confirmed-deaths-in-england-report
https://americanconservativemovement.com/2021/05/08/57-leading-scientists-doctors-and-public-policy-experts-call-for-immediate-halt-to-covid-vaccine-programs/
*
Francuski virolog i dobitnik Nobelove nagrade Luc Montagnier nazvao je masovnu vakcinaciju protiv koronavirusa tokom pandemije „nezamislivom“ i istorijskom greškom koja „stvara varijante“ i dovodi do smrti od te bolesti.
„To je ogromna greška, zar ne? Naučna greška kao i medicinska greška. To je neprihvatljiva greška”, rekao je Montagnier u intervjuu koji je juče prevela i objavila RAIR Foundation USA. „Istorijske knjige će to pokazati, jer je vakcinacija ta koja stvara varijante.“
Mnogi epidemiolozi to znaju i „šute“ o problemu poznatom kao „pojačavanje zavisno od antitijela“, rekao je Montagnier.
“Antitijela koja proizvodi virus omogućavaju da infekcija ojača”, rekao je on u intervjuu Pierre Barneriasu iz Hold-Up Media ranije ovog mjeseca.
VAKCINACIJA KOJA DOVODI DO VARIJANTI
Iako se varijante virusa mogu pojaviti prirodno, Montagnier je rekao da vakcinacija vodi proces. „Šta radi virus? Da li umire ili pronalazi drugo rješenje?“
„Jasno je da su nove varijante stvorene selekcijom posredstvom antitijela zbog vakcinacije.“
Vakcinacija tokom pandemije je „nezamisliva“ i uzrokuje smrt, rekao je dobitnik Nobelove nagrade za medicinsko otkriće za 2008. godinu
“SMRTI PRATE VAKCINACIJU”
„Nove varijante su proizvod i rezultat vakcinacije. To vidite u svakoj zemlji, to je isto: u svakoj zemlji smrtni slučajevi prate vakcinaciju“, rekao je.
https://www.youtube.com/watch?v=xSrc_s2Gqfw&t=9s
https://www.logicno.com/hrana-zdravlje/masovna-covid-vakcinacija-neprihvatljiva-greska-koja-stvara-varijante.html
*
Virusni pobeg, dr. Stephanie Seneff (str. 26)
https://ijvtpr.com/index.php/IJVTPR/article/view/23
*
Explosion of 3,500 new covid “variants” follows mass vaccination campaign in India
There are now 3,532 circulating Wuhan coronavirus (Covid-19) “variants” in India, new reports indicate, and they all came about almost immediately after people started getting mass injected with the “vaccines.”
According to a May 6 report from The Hindu, 27 states throughout India are confirmed to be afflicted with these variants, which were identified from 13,000 samples that were sequenced for variants. Among the 3,532 variants identified, 1,527 were found to be B.1.6.1.7, or “double mutant,” variants.
This news prompted the Indian government to announce a “third wave” of the Chinese Virus, which it says is “inevitable looking at the current surge in infections.”
The B.1.1.7 variant said to be circulating throughout the United Kingdom is supposedly on the decline in India, while another double mutant strain known as B.1.617 is said to be on the rise.
The Indian government says that B.1.617 could be linked to the “second wave” that reportedly caused a number of deaths in past weeks.
“The current surge in cases seen over the last and a half month in some states shows a correlation with the risk of the Indian mutant variant,” announced S.K. Singh, director of India’s National Center for Disease Control (NDCC).
“The U.K. variant is declining in proportion across the country in the last one and half months.”
The “vaccines” are spreading the variants, and communist China is laughing about it
Right around the time that the mainstream media began reporting these numbers and talking about scary new variants of the Wuhan Flu, Kamala Harris issued a travel ban against India.
Since the first, second and however many Chinese Virus “waves” there have been at this point have all fizzled out, the establishment is now working overtime to try to reignite fear about even more waves in order to keep people scared and muzzled inside their homes for the rest of their lives.
In talking about its record-breaking daily death toll, India’s health ministry blamed the “variants” rather than discussing the elephant in the room. Everything was fine in India until the mass vaccination campaigns began, and now more people are dying daily than ever before.
Could it be that the injections are responsible? The obvious answer is yes. But as long as the mainstream media refuses to connect the dots, many will believe that the variants are spreading through the air, necessitating the creation of even more deadly vaccines.
This vaccine addiction will be the downfall of the planet, which has been brainwashed into believing that every sniffle requires another injection as a “cure.” And with each new injection comes more disease, creating an endless cycle of diseases and vaccines.
Meanwhile, India is trying to save face by putting out messaging claiming that the situation is under control and that other countries should not worry. Communist China, in response, has been mocking India and the mass death that is occurring there.
The Chinese Communist Party (CCP) certainly knows that the injections are spreading the disease, seeing as how both were made in China – thanks to Anthony Fauci.
How quickly many have forgotten that we would not even be in this mess were it not for the machinations hatched in Wuhan a year-and-a-half ago. Both the East and the West were involved in the unleashing of all this, and there is no end in sight to the madness.
“Truth can never be buried forever; it will come out,” says GNews “With the help of the Whistleblower movement, people and countries around the world will find out the truth about the origin of the CCP virus soon.”
More related news about the Wuhan coronavirus (Covid-19) death jabs can be found at ChemicalViolence.com.
https://www.naturalnews.com/2021-05-20-3500-covid-variants-mass-vaccination-campaign-india.html
*
*
https://m.facebook.com/story.php?story_fbid=5772534079455521&id=100000969581998
*
*
*
*
UK SAGE REPORT:
The combination of high prevalence and high levels of vaccination creates the conditions in which an immune escape variant is most likely to emerge.
*
Synopsis
The current expansion in prevalence of infectious Sars-CoV-2 variants is highly problematic because it erodes natural Ab-based, variant-nonspecific immunity in the non-vaccinated part of the population. The high infectivity rate that results from this expansion not only further enhances the expansion of these variants but may also drive natural selection of viral variants that are featured by an even higher level of infectiousness. Erosion, therefore, of natural Ab-based, variant-nonspecific immunity promotes breeding and transmission of more infectious viral variants in the non-vaccinated part of the population. On the other hand, mass vaccination promotes natural selection of increasingly vaccine immunity (VI)-escaping variants in the vaccinated part of the population. Taken together, mass vaccination conducted on a background of high infectivity rates enables more infectious, increasingly VI-escaping variants to expand in prevalence. This evolution inevitably results in inclining morbidity rates in both, the non-vaccinated and vaccinated population and precipitates the emergence of circulating viral variants that will eventually fully resist vaccine-mediated immunity (VMI). This is why mass vaccination campaigns should not be conducted during a pandemic of a highly mutable virus, let alone during a pandemic of more infectious variants (unless transmission-blocking vaccines are used!). It is critical to understand that a rapid decline in viral infectivity rates that is not achieved by natural infection but merely results from expedited mass vaccination campaigns will only delay abrupt propagation of emerging, fully vaccine-resistant viral variants and hence, only delay the occurrence of a high wave of morbidity and mortality. In contrast, mass vaccination campaigns that are progressing more slowly, especially when conducted on a background of relatively low infectious pressure, will result in a steadily growing propagation of increasingly VI-escaping variants and hence, cause a wave of morbidity and mortality that continues to grow bigger and larger as more and more people become vaccinated. It’s only when fully vaccine-resistant viral variants will become dominant that this wave will start to peak.
To prevent more detrimental consequences of the ongoing evolution of Sars-CoV-2, we have no choice but to mitigate erosion of natural, Coronavirus (CoV)-nonspecific immunity in non-vaccinated individuals and exertion of strong immune selection pressure on immunodominant vaccinal epitopes in vaccinated individuals. This is to say that we must stop mass vaccination and lower viral infectivity rates immediately. Continued mass vaccination will only lead to a further increase in morbidity and hospitalization rates, which will subsequently culminate in a huge case fatality wave when expansion of more infectious, vaccine-resistant variants will explode.
A rapid and substantial decrease in viral infectivity rates could be achieved by a short-term course of large-scale antiviral chemoprophylaxis (suitable candidates have already been identified) and adequate infection prevention measures while early treatment of symptomatically infected subjects and implementation of a healthy eating (including certain dietary supplements) and lifestyle (including exercise!) plan would further contribute to building herd immunity. Although this strategy is unlikely to eradicate the virus, it should allow forcing the pandemic into transitioning to a kind of ‘artificial’endemicity. Of course, as asymptomatic reservoirs (asymptomatically infected vaccinated or non-vaccinated humans or even animals) would remain, mass gatherings would still need to be avoided in the future and large-scale chemoprophylaxis campaigns using antiviral drugs would likely need to be repeated at specific time intervals and for as long as no sterilizing immune intervention is available. The action plan proposed above should immediately be implemented: Once the virus will become entirely resistant to the current vaccines, the above-mentioned measures will no longer be able to prevent a dramatic rise in casualties, unless campaigns of antiviral chemoprophylaxis are conducted worldwide and on a permanent basis.
Analysis of current evolution of the pandemic and impact thereon of mass vaccination campaigns
I herewith reiterate that I will continue to distance myself from those who pretend the pandemic is over or at least toning down as a result of growing herd immunity (HI). I take issue with the way the observations of genomic/ molecular epidemiologists are downplayed and with the fact that immunological data are oftentimes ignored, taken out of context, misinterpreted or not understood. I do not concur with experts who pretend that the pandemic has now started transitioning into an endemic phase and that the virus will eventually spontaneously degrade into yet another common cold CoV that is only of minor concern to public health. It seems, indeed, like some experts now tend to attribute diminished severity of disease and declining mortality rates to growing HI and/ or waning viral virulence. As will be explained below, the predictions they make are not taking into account the complex interplay between the growing infectious pressure exerted by more infectious circulating viral variants and the rising immune selection pressure exerted on the virus by the rapidly expanding immunized population. Their predictions are also not in line with recently published data from molecular/ genomic epidemiologists showing how rising population-level immune selection pressure is now driving the genomic evolution of Sars-CoV-2 variants (see my recent contribution: 'Why the ongoing mass vaccination experiment drives a rapid evolutionary response of SARS-CoV-2').
It is simply mind-blowing that some experts still continue to ignore the negative impact of mass vaccination on the evolution of this pandemic. On the contrary, some of them even pretend that the weak link between the number of infectious cases and morbidity/ hospitalization rates, as now observed in several countries in Europe and in the US, proves that variants do not escape the immune system. They attribute this to a kind of broadly protective HI that has been acquired through previous exposure to common cold CoV and/or previous asymptomatic infection with Sars-CoV-2 and/or (according to others) Covid-19 vaccination. Some experts even continue to emphasize the role of cross-reactive T cells elicited by one or more of the above-described immunization events as a key contributor to HI. That cross-reactive memory T cells would prevent spike(S)-directed immune escape and, therefore, prevent S-directed immune escape variants from propagating and adapting to the host population is not based on any scientific evidence. There is, indeed, no scientific proof whatsoever that cross-reactive memory T cells in previously exposed or vaccinated individuals effectively contribute to eliminating/ killing CoV-infected cells. There is not even proof that any kind of T cell could possibly eliminate CoV-infected host cells in the absence of S-specific memory B cells. There is, therefore, no scientific evidence that cross-reactive, variant-nonspecific T cells contribute to curtailing or diminishing viral transmission and thus, contribute to HI. If the opposite would apply, one would not understand why, at a later stage of the pandemic, some previously asymptomatically infected subjects all of a sudden contract Covid-19 disease!
But even anti-S Abs generated upon previous exposure to common cold CoV or upon previous asymptomatic infection with Sars-CoV-2 or after immunization with Covid-19 vaccines fail to control viral transmission. This is because
-
Anti-S Abs elicited by previous exposure to common cold CoV do not neutralize Sars-CoV-19
-
Anti-S Abs elicited by asymptomatic infection are short-lived and not fully functional (there is no evidence that asymptomatic infection with Sars-CoV-2 induces memory B cells). It has been reported that these short-lived Abs are not responsible for virus elimination (the latter occurs even before anti-S-Abs start to peak)
-
Anti-S Abs elicited by vaccination lose their neutralizing capacity towards more infectious and increasingly S Ab-resistant variants (hence, explaining the steadily increasing occurrence of ‘breakthrough’ cases).
But, even more importantly: How do these experts reconcile an allegedly growing HI with rising infectivity rates that are currently observed in many countries due to increased circulation of the delta variant? Wouldn’t this argue for a growing erosion rather than for a consolidation of HI? This observation is certainly far from indicating that the pandemic is currently transitioning into endemicity.
So, if HI cannot account for reduced severity of the disease, then maybe spontaneous attenuation of the virus could? But how on earth would a treacherous virus all of a sudden breed descendant variants that are no more harmful than a common cold CoV? Viruses can only replicate, mutate or hide. Selection and adaptation of the mutations they produce is driven by selection pressure placed on specific phenotypic features of the virus. But what kind of selection pressure would force the virus into attenuation? And how could that happen, given that the current selection pressure on Sars-CoV-2 is reportedly known to be exerted by the population’s overall immune status and is directed at the S protein, which is known to enable viral infectiousness? When and how does natural immune selection pressure on the infectiousness of a pathogen cause diminished virulence? If these mass vaccination campaigns were really driving the propagation of ‘attenuated’ viral variants that are no longer of public health concern, I would rather welcome them as a blessing rather than rejecting them as a scourge (1)! However, as far as I am aware, no genomic evidence has been provided so far to show that the delta variant or any other more infectious variant is currently evolving mutations that would mediate a more benign course of the disease or enable the virus to become intrinsically more infectious for younger age groups.
The scientifically more plausible explanation for the observed decline in disease severity in the non-vaccinated is that the delta variant, or any other more infectious variant, increasingly affects younger age groups (e.g., young adults). Younger age groups have higher levels of natural, polyreactive B1b Abs and can, therefore, better cope with antigenic variants than the elderly or individuals with underlying disease (see references from the literature on my website under topic 1). This already explains why the delta variant is seemingly ‘less virulent’. But why does the delta variant (or other more infectious variants) increasingly target young to middle-aged adults? This, most likely, has to do with its higher level of infectiousness rather than with its intrinsic virulence. Higher viral infectiousness implies enhanced affinity of the variant spike protein for the Ace-2 (angiotensin-converting enzyme 2) entry receptor. Enhanced affinity results in diminished capture of the virus by natural, variant-nonspecific Abs. There is abundant and compelling scientific evidence on the protective effect of polyreactive, natural Abs, including their protective effect against a number of viral infections (see references from the literature on my website under topic 1). Elevated levels of these Abs are to be considered a hallmark of natural protection from symptomatic infection upon Sars-CoV-2 exposure. It is, therefore, reasonable to assume that individuals with low functional levels of natural Abs will be more prone to contracting severe Covid-19 disease.
But how or why do more infectious variants arise?
During the first ten months of the pandemic, high waves of infectious cases that occurred in overcrowded areas (e.g., slums, favelas, highly populated cities,..) affected by the pandemic may have caused immune pressure on viral infectiousness, especially upon re-exposure of previously asymptomatically infected individuals. It is possible that such events have been driving natural selection and enhanced circulation of more infectious, S-directed immune escape variants. The higher and more widespread the viral infectious pressure, the higher the likelihood that previously asymptomatically infected subjects become re-exposed to the virus at a point in time where their titers of low affinity, S-directed Abs are still high enough to compete with their natural, polyreactive Abs for binding to the circulating Sars-CoV-2 lineage (see Fig. 1; in previous contributions, I have explicitly explained why S-specific Abs have higher affinity for S protein than natural IgMs, which bind to virus surface-expressed motifs through multivalent interactions). Consequently, enhanced infectivity rates could lead to a transient increase of the susceptibility of younger age groups (< 60-65 years) to Covid-19 disease and may, therefore, raise morbidity and hospitalization rates in these age groups (as is currently observed in many European countries as well as in the US). So, the higher and more widespread the viral infectious pressure, the more productive the breeding ground for more infectious variants and the higher the likelihood for natural selection of certain S-directed immune escape variants (i.e., such that evolved mutations capable of resisting suboptimal immune pressure on viral infectiousness). Immune escape variants that are selected because of their capacity to overcome such immune pressure exhibit a higher level of infectiousness. This is how high infectivity rates facilitate breeding of increasingly infectious viral variants. During the first year of the pandemic, several of such ‘more infectious’ immune escape variants have emerged (e.g., alpha (2), beta, gamma, delta).
Depending on the remaining protective effect provided by natural Abs, younger and healthy age groups, and children in particular, may not even show any symptoms at all, even though dominant circulation of more infectious variants (e.g., delta variant) is now substantially increasing the risk of repeated exposure. This already explains why Covid-19 disease in the non-vaccinated is primarily observed in young, middle-aged adults. Since younger age groups are generally better protected by natural, poly-reactive Abs, cases of severe disease in these groups are rather rare. The severity of the disease in these subjects is thought to depend on the time point of re-exposure after their previous infection (i.e., the shorter thereafter, the higher the concentration of blocking S-specific Abs, the higher the likelihood for contracting more severe disease).
Because both, binding of natural CoV-nonspecific Abs to Sars-CoV-2 and binding of Sars-CoV-2 to the Ace-2 entry receptor is mediated by multivalent interactions, it is reasonable to assume that the blocking effect of natural, CoV-nonspecific Abs on the interaction between the Ace-2 receptor and a given Sars-CoV-2 lineage primarily depends on the functional concentration of these natural Abs. This would already explain why, under normal circumstances (i.e., if not suppressed by S-specific Abs), young and/ or healthy individuals can effectively deal with all Sars-CoV-2 viral variants. The higher the affinity of S for Ace-2 (i.e., the higher the level of intrinsic viral infectiousness) and the older the age group, the lower the residual (i.e., non-suppressed) functional capacity of natural Abs.
In contrast, vaccinal Abs are directed at a limited set of S-derived Sars-CoV-2 motifs (i.e., epitopes primarily comprised within the receptor-binding domain [RBD] of the S protein). Hence, very few mutations within this limited set of epitopes will already substantially diminish the affinity of vaccinal Abs for binding to Sars-CoV-2. This, however, does not apply to S-specific Abs acquired upon recovery from natural Covid-19 disease as those are directed at a much broader and diversified spectrum of B cell epitopes. This would already explain why more infectious Sars-CoV-2 variants more readily escape from vaccinal S-specific Abs than from naturally acquired S-specific Abs and also why we are now seeing more and more breakthrough disease cases with the more infectious delta variant in vaccinees whereas young and/ or healthy individuals or previously symptomatically infected people (provided seronegative for S protein (3)) remain largely protected from Covid-19 disease.
Molecular epidemiologists conclude that, because of the steadily increasing S-directed immune pressure exerted by the human population, circulating variants are now increasingly evolving mutations that drive resistance to S-specific Abs, especially to those recognizing immunodominant epitopes that are situated within the RBD and N-terminal domain (NTD) of the S protein. It is highly unlikely that naturally acquired S-specific Abs are responsible for this immune pressure as people who recover from Covid-19 disease only constitute a relatively small subset of the population and mount Abs against a much broader and more diversified panel of S-derived epitopes. Given the nature of the vaccinal Abs and the large vaccine coverage rates in most countries, there can be no doubt that the steadily increasing population-level immune pressure found to be exerted on RBD, for example, is caused by vaccination of large masses of people (in a previous contribution, I have expressed my astonishment about the fact that these brilliant scientists didn’t even mention ’mass vaccination’ at all as a potential cause of the massive increase in S-directed immune pressure; (see my recent contribution: 'Why the ongoing mass vaccination experiment drives a rapid evolutionary response of SARS-CoV-2'). This evolution is, of course, extremely worrisome. Whereas progressing convergent evolution towards increased resistance against functional, S-specific Abs elicited by the vaccine may not necessarily further increase the affinity of the virus for the Ace-2 receptor (and hence, not commonly cause more disease in young and healthy individuals), it is reasonable to assume that such evolution will rapidly raise the number and severity of disease cases in the vaccinated part of the population. This is because growing VI escape will cause vaccinees to lose their vaccine-mediated immune protection while having their natural, CoV-nonspecific natural Abs suppressed by high titers of long-lived, S-specific vaccinal Abs (4). It is reasonable to assume that, as a general rule, the level of suppression of natural, CoV-nonspecific Abs will increase with increasing strength (adjuvantation!), frequency and coverage rate of booster immunizations (including 2nd generation vaccines!).
Vaccinal S-specific Abs cannot outcompete S-specific Abs from previously symptomatically infected individuals for binding to viral variants due to multivalent B-cell epitope recognition by the naturally primed immune system. On the other hand, immunity acquired upon recovery from natural Covid-19 disease is very robust and has repeatedly been reported to be capable of dealing very effectively with a diversified range of antigenic variants upon re-exposure (including variants of concerns; VoCs). Non-antigen (Ag)-specific innate immune adjuvantation enables epitope spreading and is, therefore, likely to contribute to broad immune recognition. Naturally acquired immunity is, therefore, an almost ‘invariant’ component to herd immunity. It is, however, uncertain whether binding of S-specific Abs from previously symptomatically infected individuals to circulating VI-escaping viral variants could render these individuals more susceptible to Ab-dependent enhancement of disease (ADE).
Based on all of the above, it becomes already apparent that mass vaccination campaigns conducted in the midst of a pandemic of more infectious variants will rapidly and dramatically weaken instead of strengthen the population’s overall immune protection status and, therefore, not contribute to generating herd immunity. This is because mutual viral transmission between the non-vaccinated and vaccinated population enables a self-amplifying, synergistic effect between high viral infectivity rates (due to more infectious circulating variants) and high vaccine coverage rates (due to mass vaccination). This results in enhanced expansion of more infectious, increasingly VI-escaping variants as depicted in Fig. 2:
-
High infectivity rates turn the non-vaccinated population into a breeding ground for increasingly infectious variants and a factory for the production and transmission of such infectious variants. Due to their increasing infectiousness and expansion in prevalence, viral infection and transmission rates rapidly increase and further erode natural immunity in a number of previously asymptomatically infected individuals (i.e., starting with healthy, middle-aged adults and progressively involving younger and younger individuals). This, in turn, increases S-directed immune selection pressure and drives natural selection and possibly adaptation of even more infectious variants.
-
High vaccine coverage rates turn the exposed vaccinated population into a brewery for more VI-escaping viral variants.
-
Upon their transmission to vaccinees, more infectious variants that will evolve additional mutations conferring increasing resistance to functional S-directed vaccinal Abs will be selected as those gain a competitive advantage in vaccinees and will, therefore, reproduce more effectively. Subsequent transmission of the VI-escaping variants to non-vaccinated subjects will enable them to rapidly expand in prevalence and, therefore, replace or at least dominate previously circulating variants.
The interactions described above allow to understand how mass vaccination on a background of enhanced viral infectiousness (pandemic!) engages both, the vaccinated and unvaccinated population to expedite natural selection and adaptation of immune escape variants harboring additional, RBD-associated mutations which increasingly inhibit VMI. This is to say that mass vaccination campaigns conducted during a pandemic of more infectious variants will precipitate resistance of more infectious Sars-Cov-2 variants to S-based Covid-19 vaccines.
The more ‘more infectious’ variants expand and dominate and the more these variants are subject to vaccine-mediated immune selection pressure, the more rapidly the beneficial effect from mass vaccination (i.e., reduction of viral transmission and prevention of disease) will be replaced by a growing failure of the vaccines to protect the vaccinees and of the vaccinees to protect the unvaccinated. This evolution is currently expedited by relaxation of infection-prevention measures, including more frequent contacts among healthy individuals. More frequent contacts between asymptomatically infected vaccinated and non-vaccinated subjects (5) will only promote breeding of new variants that are both, more infectious and more readily escape from vaccine immunity (e.g., lambda variant).
Summary
In summary, it is reasonable to postulate that the expansion of a series of more infectious variants and the concomitant explosion of infection rates is due to self-amplifying natural selection and adaptation of more infectious circulating variants, some of which likely emerged and propagated as a result from overcrowding. As the more infectious alpha, beta, gamma or delta variants emerged prior to the deployment of mass vaccination campaigns, the latter can, indeed, not be at the origin of these variants. However, as the human population have recently been reported to exert more and more immune pressure on immunodominant epitopes comprised within the RBD, it is reasonable to assume that this additional immune pressure results from mass vaccination because vaccine coverage rates are steadily growing. More infectious variants that have evolved to harbor naturally selected, S-directed immune escape mutations will readily gain a competitive advantage as continued mass vaccination campaigns with current S-based Covid-19 vaccines cause vaccinees to augment and broaden immune selection pressure on critically important, immunodominant epitopes comprised within those vaccines. Due to widespread immune selection pressure combined with a high viral infection rate and more frequent contacts between healthy vaccinated and non-vaccinated people, more infectious immune escape variants will now rapidly further evolve to fully escape VMI while expanding in prevalence. This is to say that new immune escape variants that can no longer be eliminated by any kind of VMI will soon become the dominant circulating strains.
In other words, high viral infection rates drive natural selection and self-amplifying expansion of more and more infectious Sars-CoV-2 variants in the non-vaccinated part of the population while high vaccine coverage rates drives natural selection of increasingly VI-escaping Sars-CoV-2 variants. This evolution is now driving enhanced rates of disease in both populations. Consequently, mass vaccination during a pandemic of more infectious variants self-amplifies natural selection and expansion of more infectious, increasingly VI-escaping Sars-CoV-variants. Both, the vaccinated and non-vaccinated part of the population fully contribute to this evolution.
Because of all of the above, I can certainly not endorse the opinion of those who think that the decrease in disease severity and hospitalizations that is now observed in several countries where mass vaccination is well advanced would be due to some kind of ‘attenuation’ of viral variants or to some kind of growing HI. One rather concludes that this pandemic is far from over or from transitioning into endemicity. There can be no doubt that, at this stage, the pandemic is gearing up for breeding vaccine-resistant ‘supervariants’, a phenomenon that is at risk of fueling an even larger wave of morbidity, hospitalization and, unfortunately, also death, not at least in the vaccinated part of the population.
The ongoing mass vaccination campaigns must immediately be abrogated because the vaccines fail to block viral transmission and their large-scale use during a pandemic of more infectious variants will inevitably lead to vaccine resistance of circulating Sars-CoV-2 variants. Instead, mass chemoprophylaxis campaigns should be conducted at regular intervals to reduce viral infectious pressure and transmission and prevent more infectious viral variants from fueling the breeding and dominant propagation of more infectious, vaccine-resistant variants. Furthermore, people should boost their health status whereas early treatment of patients who come down with Covid-19 disease (for more information, please consult, for example, prof. Dr. P. McCullough’s presentations and publications) would not only prevent severe disease and hospitalization but also enable these patients to more rapidly acquire broadly protective Abs facilitating killing/ elimination of virus-infected host cells and, therefore, diminish viral transmission and contribute to herd immunity. The above-mentioned interventions have been summarized in Fig. 3.
As we are now dealing with a pandemic of highly infectious variants (e.g., delta variant), we cannot afford any longer to target herd immunity without relying on large scale antiviral chemoprophylaxis combined with early treatment of Covid-19 diseased patients. This, together with an immediate halt of all Covid-19 mass vaccination campaigns, should now constitute the main pillars of our battle against this otherwise totally uncontrollable pandemic.
As much as I follow reports on vaccine safety issues with a great deal of concern, worry and anxiousness, I tend to believe that the potential epidemiological impact of these vaccination campaigns on human lives could be orders of magnitude larger than that of their potential short- or long-term sequelae. I am, therefore, begging the WHO and all stakeholders of these campaigns to immediately intervene as proposed above. After the first experiment failed (instead of generating herd immunity, mass vaccination is now turning vaccinees into potential spreaders of VI-escaping variants!), our human race cannot afford a second large scale experiment that aims at continuing mass vaccination while promoting exposure of the population to an even higher infectious pressure exerted by even more infectious immune escape variants!
Overall Conclusion
Both, long-lived Sars-CoV-specific immunity acquired upon recovery from disease and innate, CoV-nonspecific Ab-mediated immunity normally contribute to establishing broadly protective herd immunity and thereby enable a natural CoV pandemic (or, for that matter, any pandemic of an acute, self-limiting viral disease) to eventually transition into an endemic phase. However, circulation of more infectious variants comes with a high price to pay for herd immunity to establish as high infectivity rates are more likely to erode natural, polyreactive (i.e., CoV-nonspecific) immunity in young and/ or healthy individuals. As a result, morbidity and hospitalization rates, and ultimately also the number of deaths, will increase. This self-amplifying cycle of enhanced viral infectiousness (resulting in enhanced viral infectivity rates) would only come to an end when the population density is diluted down to a level low enough for viral transmission (of a highly transmissible/ infectious variant!) to substantially diminish.
Whereas fast and dominant propagation of naturally selected, more infectious variants continues to erode the natural first line of variant-nonspecific immune defense in the non-vaccinated part of the population, vaccination of large parts of the population and contacts among vaccinated and non-vaccinated subjects are driving natural selection and adaptation of increasingly VI-escaping variants and are, therefore, increasingly compromising VMI. Neither previous CoV infection (including Sars-CoV-2 infection), nor higher vaccine coverage rates can compensate for the lost immunological capacity. Indeed, memory T cells elicited upon previous CoV infection or vaccination are not reportedly known to be endowed with cytotoxic activity towards CoV-infected cells, nor can S-specific Abs elicited upon previous CoV infection or vaccination prevent spreading of more infectious Sars-CoV-2 variants. Molecular epidemiologists have suggested that immune failure to block viral transmission (e.g., in immunosuppressed patients) causes variants to convergently evolve specifically selected mutations, thereby enabling escape from VMI. VI escape together with suppression of natural, CoV-nonspecific Abs by vaccinal Abs will make vaccinees highly susceptible to contracting Covid-19 disease.
Dominant propagation of more infectious viral variants could be mitigated by mass chemoprophylaxis using a potent antiviral. At the same time, immune pressure on vaccinal S-specific epitopes must be mitigated by calling an immediate halt to mass vaccination campaigns. Furthermore, early treatment of symptomatic subjects can prevent severe disease and provide them with durable protection against a diversified spectrum of more infectious variants and, thereby, also reduce viral transmission. However, this is the last opportunity to limit the disastrous consequences of mass vaccination
Indeed, it is yet uncertain and unexplored to what extent naturally selected immune escape variants can recombine upon co-infection and generate even more complex variants, the phenotypic characteristics of which are totally unpredictable. It is also unclear whether early treatment could prevent vaccinees who have become highly susceptible to Covid-19 disease (i.e., due to viral resistance to VMI) from succumbing to severe disease. In addition, it is completely unknown whether vaccinees and even individuals who previously contracted symptomatic infection are more likely to fall victim to enhanced Covid-19 disease (i.e., ADE) as their vaccinal Abs may no longer be able to neutralize the virus but could still bind to it. Treatment of patients with ADE may be much more difficult and the outcome less predictable.
The more Sars-CoV-2 evolves to acquiring VI-escaping properties, the less likely vaccinees will benefit from the above-proposed strategy. This is because even low infectivity rates of circulating variants could suffice to boost their vaccinal Abs and hence, suppress their innate immune defense. Such re-stimulation could only be prevented by eradicating all of the currently circulating Sars-CoV-2 variants. Eradication of those could be achieved by using universal vaccines (6) that induce sterilizing immunity. The development of such vaccines may require a fundamentally different approach to immune intervention in that induced immune effector cells ought to be capable of CoV-nonspecific killing of CoV-infected cells and provide durable protective immunity in all subjects of the population (regardless of their immunization history and immunogenetic background). It goes without saying that such characteristics would render a vaccine highly and durably effective, even when used in mass vaccination campaigns in the midst of a pandemic of a highly mutable virus, and even if more infectious viral variants would already be circulating. Vaccine safety remains of course paramount and cannot be subject to any compromise, especially not when a smart combination of antiviral chemoprophylaxis, infection prevention, early treatment and adherence to health-strengthening eating and life-style habits could still be safe and effective in preventing cases of severe disease and prevent VI-escaping variants from becoming dominant.
Unless continued mass vaccination with S-based vaccines in populations exposed to a CoV pandemic would be proven to not cause immune selection pressure on the functionality of the vaccinal Abs and unless S-specific Abs would be proven to not compete with natural, CoV-nonspecific Abs for binding to Sars-CoV-2, mass vaccination campaigns during a pandemic, especially during a pandemic of more infectious variants, will neither enable herd immunity nor mitigate future waves of disease (unless transmission-blocking vaccines are used!). In fact, they have exactly the opposite effect in that they promote the spread of increasingly VI-escaping variants and suppress natural immunity in vaccinees. This will only result in higher morbidity and mortality rates in the part of the population that is normally naturally protected from Covid-19 (i.e., the vast majority of the population). A decline of severe morbidity and mortality rates is only observed in the elderly and in people with some underlying diseases. The outcome, therefore, of the mass vaccination campaigns is very different from the original objective, which was to protect the vast majority of people, including those who are immunologically Sars-CoV-2 naïve (via herd immunity!). Scientifically speaking, it is hard to understand how the circulating, more infectious Sars-CoV-2 variants would not rapidly evolve to overcome the RBD-directed immune pressure that is currently exerted by large parts of the human population and merge into a supervariant that evades the immune response induced by all of the S-based Covid-19 vaccines. It is simply unthinkable that the ongoing mass vaccination campaigns could mitigate, let alone terminate, this pandemic of more infectious Sars-CoV-2 variants and force the virus into adopting milder instead of even more problematic features.
I, therefore, reiterate that the currently observed convergence of naturally selected mutations towards S-derived antigenic sites that facilitate or are directly responsible for binding to the Ace-2 entry receptor combind with the velocity at which this evolution currently takes place poses a huge and imminent threat to the human population and will heavily backfire if we continue mass vaccination on a background of high viral infection rates while largely relaxing infection prevention measures.
Last but not least, it must be emphasized that those calling themselves ‘experts’ while pretending that this pandemic is ‘a pandemic among the non-vaccinated’ are devoid of any scientific insight in the evolutionary dynamics of Sars-CoV-2 as currently shaped by a combination of high viral infectivity and vaccine coverage rates. Neither the vaccinated (who merely believed the vaccine would protect them from Covid-19 disease) nor the non-vaccinated (who simply believe there is no need for them to take the vaccine in order to stay protected) are to be blamed for the escalation of this pandemic. Mass vaccination is the one and only culprit.
Note: A copy of this letter has been sent to WHO, NIH, CDC, the Bill & Melinda Gates Foundation, GAVI, CEPI, FDA, EMEA and to R&D leaders from Pfizer, Moderna, Astra-Zeneca, J&J, Novavax and GSK
Hoće li vakcine protiv COVID-a pokrenuti mutaciju SARS-CoV-2, stvarajući sve više varijanti? Ili se mutacije uglavnom javljaju kod nevakcinisanih ljudi?
Nevakcinisani su zapravo većina, bez obzira šta se priča na glavnim vestima. Oni što kažu “NE učestvovanju u eksperimentu genske modifikacije, nisu mala grupa!”
U Americi je zaključno sa 12.julom 2021. nevakcinisanih 51% stanovništva starijih od 18 godina.
U Srbiji je nevakcinisano ukupno 38,5% stanovništva, a ukupno na svetu je nevakcinisanih 86.7%, zaključno sa 20. julom 2021. godine.
Na osnovu naučnih dokaza, narativ da su nevakcinisani ljudi fabrike virusa za opasnije i nove varijante jednostavno je lažan. Još gore, potpuno je suprotno od istine i skriva činjenicu da nas masovna vakcinacija možda sve dovodi u mnogo težu situaciju nego što je to zaista potrebno.
Vakcine teraju viruse na mutaciju
Kao što je objašnjeno u „Vakcine teraju patogene da se razvijaju“, objavljeno u časopisu Quanta. Baš kao što antibiotici rađaju otpornost na bakterije, vakcine mogu podstaći promene koje omogućavaju da bolesti izmaknu njihovoj kontroli.“
Članak detaljno opisuje istoriju vakcine protiv Marekove bolesti kod kokošaka, koja je prvi put predstavljena 1970. godine. Danas smo na trećoj verziji ove vakcine, jer u roku od jedne decenije prestaje sa svojom funkcijom. Razlog? Virus je mutirao da izbegne vakcinu. Virus takođe postaje sve smrtonosniji i sve je teži za lečenje.
Rad iz PLOS Biology iz 2015. godine testirao je teoriju da vakcine pokreću mutaciju herpes-virusa koji uzrokuje Marekovu bolest kod kokošaka. Da bi to učinili, vakcinisali su 100 pilića, a 100 držali nevakcinisanim. Sve ptice su tada zaražene različitim sojevima virusa. Neki sojevi su bili virulentniji i opasniji od drugih.
*
When two great minds come to similar conclusions about the current global push to vaccinate everyone with the COVID experimental vaccines, we should pay close attention. Both highly experienced scientists have a totally negative view of the vaccination effort. Worse than being ineffective, they point to negative health outcomes for the global population. These two truth-telling acclaimed medical researchers make Fauci look as inept, deceitful and dangerous as he is.
The point made in this article is not only has Fauci pushed the wrong potentially disastrous pandemic solution, he has blocked the right one.
Much of what the two virologists say is very technical in nature. This article simplifies their controversial messages without losing their essential meanings. The public needs to understand their warnings that refute all the propaganda pushing vaccines from government and public health agencies as well as big media.
Warning: Keep reading and you may become depressed.
*
Dr. Luc Montagnier
First considered is the thinking of Dr. Luc Montagnier, a French virologist and recipient of the 2008 Nobel Prize in Medicine for his discovery of the human immunodeficiency virus (HIV). He has a doctorate in medicine. But there is a lot more to conclude he is a great expert: He has received more than 20 major awards, including the French National Order of Merit and the Légion d’honneur. He is a recipient of the Lasker Award, the Scheele Award, the Louis-Jeantet Prize for medicine , the Gairdner Award the Golden Plate Award of the American Academy of Achievement, King Faisal International Prize (known as the Arab Nobel Prize), and the Prince of Asturias Award.
He has worked hard to expose the dangers of the COVID-19 vaccines, still experimental but sadly may soon be fully approved. The vaccines don’t stop the virus, argues the prominent virologist, they do the opposite — they “feed the virus,” and facilitate its development into stronger and more transmittable variants. These new virus variants will be more resistant to vaccination and may cause more health implications than their “original” versions.
Montagnier refers to the mass vaccine program as an “unacceptable mistake” and are a “scientific error as well as a medical error.” His assertion is that “The history books will show that…it is the vaccination that is creating the variants.” In other words: “There are antibodies, created by the vaccine,” forcing the virus to “find another solution” or die. “This is where the variants are created. It is the variants that “are a production and result from the vaccination.” Stop and think about these thoughts. Have you heard a better explanation of variant creation? I doubt it.
He is talking about the mutation and strengthening of the virus from a phenomenon known as Antibody Dependent Enhancement (ADE). ADE is a mechanism that increases the ability of a virus to enter cells and cause a worsening of the disease.
Data from around the world confirms ADE occurs in SARS-CoV-2, which causes COVID-19, says Montagnier. “You see it in each country, it’s the same: the curve of vaccination is followed by the curve of deaths.” Sounds like what we are now hearing more about, namely escalating breakthrough infections that kill some people. And this spiral into disaster may have no end.
In a November 2020 documentary he emphasized harmful and irrational mask mandates as well as lockdowns, quarantines, abuses of government overreach, and supported use of effective COVID treatments such as hydroxychloroquine. The film was banned by YouTube and most other mainstream outlets. At that time Fauci had succeeded in blocking wide use of the cheap generic based treatments for COVID and pursued the wait for the vaccine strategy.
Montagnier has been a vocal critic of the mass vaccination campaign. In a letter to the President and Judges of the Supreme Court of the State of Israel, which unrolled the world’s speediest and the most massive vaccination campaign, Montagnier argued for its suspension. He said: “I would like to summarize the potential dangers of these vaccines in a mass vaccination policy.” Here they are:
1. Short-term side effects: these are not the normal local reactions found for any vaccination, but serious reactions involve the life of the recipient such as anaphylactic shock linked to a component of the vaccine mixture, or severe allergies or an autoimmune reaction up to cell aplasia. In this group we should include a number of lethal blood problems involving clots and loss of platelets that cause strokes, brain bleeds and other impacts.
Lack of vaccine protection:
2.1 In induced antibodies do not neutralize a viral infection, but on the contrary facilitate it depending on the recipient. The latter may have already been exposed to the virus asymptomatically. Naturally induced antibodies may compete with the antibodies induced by the vaccine.
2.2 The production of antibodies induced by vaccination in a population highly exposed to the virus will lead to the selection of variants resistant to these antibodies. These variants can be more virulent or more transmissible. This is what we are seeing now. An endless virus-vaccine race that will always turn to the advantage for the virus.
Long-term effects: Contrary to the claims of the manufacturers of messenger RNA vaccines, there is a risk of integration of viral RNA into the human genome. Our cells have the ability to reverse transcriptase from RNA into DNA. Although this is a rare event, its passage through the DNA of germ cells and its transmission to future generations cannot be excluded.
His bottom line: “Faced with an unpredictable future, it is better to abstain.” But most people will find it extremely difficult to resist all the coercion and vaccine mandates.
Back in April 2020, before all the talk of variants and before the rollout of the experimental vaccines, Montagnier urged people to refuse vaccines against COVID-19 when they become available. His main point should always be remembered: “instead of preventing the infection, they [would] accelerate infection.” Today, the newly occurring variants of SARS-CoV-2 that affect vaccinated people prove his thesis. With his scientific thinking, mass vaccination may cause a new, more deadly wave of pandemic infection.
As to the much talked about and hope for herd immunity, he has said: “the vaccines Pfizer, Moderna, Astra Zeneca do not prevent the transmission of the virus person-to-person and the vaccinated are just as transmissive as the unvaccinated. Therefore the hope of a ‘collective immunity’ by an increase in the number of vaccinated is totally futile.”
On the positive side, he advocated this: “The early treatment of infection with ivermectin and bacterial antibiotic because there is a bacterial cofactor that amplifies the effects of the virus. “
Dr. Vanden Bossche
The stark views of Montagnier have been shared by the esteemed Belgium virologist Dr. Vanden Bossche. He too has considerable credentials that make his views worth consideration. He has PhD degree in Virology from the University of Hohenheim, Germany. He held faculty appointments at universities in Belgium and Germany. He was at the German Center for Infection Research in Cologne as Head of the Vaccine Development Office. He has been in the private sector at several vaccine companies (GSK Biologicals, Novartis Vaccines, Solvay Biologicals) where he worked on vaccine R&D as well as vaccine development. He also worked with the Global Alliance for Vaccines and Immunization (GAVI) in Geneva as Senior Ebola Program Manager.
His views have been analyzed in a recent article. He too has loudly called for a halt to mass-vaccination programs. He believes that if the jabs are not halted, they could lead to the evolution of stronger and stronger variants of the virus until a “supervirus” takes hold and wipes out huge numbers of people.
This is his bold view:
“Given the huge amount of immune escape that will be provoked by mass vaccination campaigns and flanking containment measures, it is difficult to imagine how human interventions would not cause the COVID-19 pandemic to turn into an incredible disaster for global and individual health.”
Here is an essential element of his thinking. Pretty much everything being done in the pandemic doesn’t guarantee elimination of the virus. What is happening is selective viral ‘immune escape’ where viruses continue to be shed from those who are infected [both vaccinated and nonvaccinated] because neutralizing antibodies fail to prevent replication and elimination of the virus.
The evolutionary selection pressure on the virus through ‘immune escape,’ creates ever more virulent strains of the virus that have a competitive advantage over other variants and will increasingly have the potential to break through the antibody defenses. Defenses provided by the vaccine induced immune system. This is ‘vaccine resistance.’ What happens is that vaccine makers keep trying to outsmart variants, but fail. So, they keep pushing boosters and yearly vaccine shots. This is the more is better approach. This is aided by suppression of many negative facts about the vaccines by big media.
A frightening forecast by Bossche is that the worst of the pandemic is still to come. Hard to believe considering all the bad news propaganda about cases, hospitalizations and deaths. But he thinks we are now experiencing the calm before the ultimate storm. Imagine a new wave of infection far worse than anything we’ve seen so far is how Bossche thinks.
How does this happen? There will be more mutants or variants to which the adaptive immune system from vaccine shots provides little resistance. At the same time there will be decreased innate or natural immune effectiveness. Unless people take a number of steps to boost their natural immunity.
Bossche consistently points to a lack of evidence that the existing global, mass vaccination program that has been mounted while there is still significant infection around, is unprecedented and there is no scientific evidence that this will work. This is why he is largely ignored.
He stresses that historic vaccination programs have always emphasized the importance of vaccinating populations prophylactically in the absence of infection pressure.
He also argues that if different types of vaccine were used that provided sterilizing immunity i.e., that prevented immune escape and killed all viruses in those vaccinated, the situation would be entirely different. Most people do not understand that the current experimental vaccines do not actually kill the virus; and that both the vaccinated and nonvaccinated shed the virus. These vaccines do not stop viral transmission. And all the contagion control measures simply to not work effectively enough to stop wide spread of the virus in its various forms.
Here is his big picture view: “There is only one single thing at stake right now and that is the survival of our human race, frankly speaking.”
But there are more strong words recently said by Bossche to pay attention to:
“every person out there who is ‘partially’ or ‘fully’ vaccinated is a walking disease incubation system that puts everyone else at risk of contracting a deadly, vaccine-caused ‘variant’ that could kill them. The ‘vaccinated’ are walking murderers spreading disease to others. Getting injected for the Fauci Flu is not only foolish; it is also a form of murder in that unvaccinated people are now at risk of contracting the deadly diseases being manufactured inside the bodies of the vaccinated. If Trump had never introduced the vaccine in the first place, the pandemic would have long ago fizzled out. Since his vaccines continue to be pushed … however, the ‘Delta’ variant is spreading like wildfire, soon to be followed by other ‘variants’ as we enter the fall season.”
This too is a very strong view. The “mass vaccination program is…unable to generate herd immunity.” If true, there is little hope of seeing the COVID pandemic ending.
What is the solution? Bossche has identified the needed alternative to the current massive vaccine effort. It is this; “This first critical step can only be achieved by calling an immediate halt to the mass vaccination program and replacing it by widespread use of antiviral chemoprophylactics while dedicating massive public health resources to scaling early multidrug treatments of Covid-19 disease.” This is referring to the early home/outpatient treatment protocols based on cheap, safe and fully approved generics like ivermectin and hydroxychloroquine; these also work as preventatives. Pandemic Blunder provides much data and advice on using this treatment approach. So, both virologists support use of what Fauci has blocked.
These action recommendations were also made by Bossche “Provide – at no cost – early multidrug treatment to all patients in need. Roll out campaigns to promote healthy diets and lifestyle.” In other words, people need to take actions to boost their natural immunity, this should include vitamins and supplements, including this cocktail: vitamin C, vitamin D, zine and quercetin.
Conclusions
Take a moment to consider that Patrick Wood on the Bannon show on August 21 concluded that all the available data from the US and Europe shows some 100,000 people have died from the COVID experimental vaccines. I agree with that assessment. And by the time you read this FDA may have given full approval to the Pfizer vaccine.
After considering what these two experts have said it is appropriate to criticize what current government officials say, namely blame the unvaccinated for the surges in COVID cases, hospitalizations and deaths. The major alternative to this thinking is that it is the vaccinated people who are creating pandemic problems, including the variants. The strong conclusion is that the current vaccines are ineffective, nonprotective and dangerous.
What is needed is an entirely new approach to COVID vaccines. Perhaps there are companies working on this. This would threaten the trillion-dollar business of the current vaccine makers.
If the people, agencies and institutions with all the power listening to these two very smart people they would devote all their energies to using alternatives to the current vaccines. We have them. Notably, the treatment protocols that so many great doctors have created and used to help their patients.
Many other physicians and medical researchers have called for a halt to the current vaccine bonanza for big drug companies. In the meantime, on a daily basis for all those willing to look at the facts, it is clearer and clearer that the experimental vaccines are not effective. It is insanity to keep doing or expanding what is not working. That is the insane world we are now experiencing even as more and people die from breakthrough infections, blood problems and other bad vaccine health impacts.
Perhaps the ugly truth about the vaccines will be widely revealed only when there are massive, widespread deaths despite all the shots and jabs. That will be too late to change pandemic management from money-driven stupidity to life-saving, medically moral actions.
*
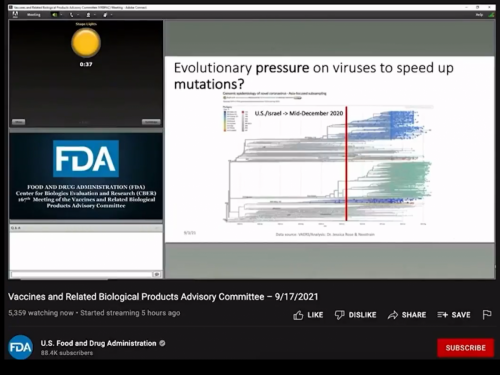
The developer of the AstraZeneca shot says the Delta variant has made herd immunity impossible because vaccinated people can still transmit the virus
The unforgivable sin
One wonders how it is possible that while it has now been reported that vaccinated shed and transmit as much virus as unvaccinated people (1), the vaccinated are still protected against severe disease whereas the unvaccinated are said to be unprotected. So, how can one explain that viral shedding and transmission and hence, viral replication no longer seem to be impacted by the vaccine whereas the opposite still applies to the occurrence of (severe) disease?
Based on their study results, the authors from the above-mentioned report (1) conclude that there is no significant difference in viral load between groups of vaccinated and unvaccinated, asymptomatic and symptomatic people who became infected with SARS-CoV-2 Delta variant. So, again: Considering that vaccinees shed and transmit as much virus as unvaccinated people, how could one even postulate that unvaccinated people are susceptible to severe disease whereas vaccinees are still largely protected from severe disease?
Frankly speaking, this doesn’t make any sense at all. So there must be a ‘small’ detail the current ‘narrative’ overlooked.
Wait a minute … Does the above-mentioned comparison of viral load between the vaccinated and the unvaccinated include people who contracted SEVERE disease? It didn’t! So, could it be that the unvaccinated are only susceptible to severe disease when their first (i.e., innate) line of immune defense is weakened because of a lowered functional capacity of their innate, poly-reactive antibodies (Abs)? Hmmm, this could definitely explain why elderly people and those who’re immune suppressed or have underlying diseases are susceptible to severe Covid-19 disease. But what about our healthy youngsters and children as these age groups are thought to have excellent innate, pre-existing immune effector cells (2) but are now also increasingly contracting severe Covid-19 disease. Could this be due to spike(S)-specific Abs that young and healthy children may harbor for up to 8 weeks after they contracted asymptomatic infection and that outcompete their innate protective Abs (3)? If this is true, this would imply that only a small part of young and unvaccinated people are susceptible to severe disease (i.e., those who get quite rapidly re-exposed to Sars-CoV-2 after previous infection) but that the vast majority of them are still protected from severe disease, regardless of which Sars-CoV-2 lineage is predominant in the circulating viral population. This seems, indeed, to be the case! Or do some of our ‘experts’ believe that the unvaccinated children and youngsters who don’t get Covid-19 disease have simply not been exposed to the virus at all? But how could that happen given the fact that in most countries the pandemic started over 1.5 years ago and that we’re now dealing with highly infectious variants and that infection prevention measures have largely been relaxed?
So, maybe we should not compare the functional immune capacity of unvaccinated youngsters who get severe disease with that of those who only get mild or moderate disease or don’t develop symptoms at all. However, it is viral transmission and shedding in the latter that has been compared to that in vaccinees (4). Does anybody realize that protection from (severe) disease in healthy children and youngsters is due to innate Abs (5), even regardless of the possible short-term presence of poorly functional S-directed Abs (which may even contribute to diminishing rather than strengthening their immune defence)? Does anybody realize that this mechanism of protection is fundamentally different from the one protecting vaccinees from severe disease? When present in sufficient concentration, high affinity, antigen-specific Abs readily outcompete low affinity, multi-specific Abs for binding to the same antigen (6). It is, therefore, reasonable to assume that vaccinees experience long-lived functional suppression of their protective, CoV-recognizing innate Abs and are thereby left to rely on their vaccinal S-specific Abs for protection against severe disease (7).
As the mechanism of immune defense in vaccinees is totally different from the one at play in unvaccinated individuals, the mantra of mass vaccination stakeholders that vaccination of youngsters and children will provide them with improved protection from contracting severe disease is a textbook example of scientific nonsense. Their irrational, erroneous extrapolations lead people to believe that they should get their children vaccinated whereas there is barely any more catastrophic immune intervention one could think of. In line with the intrinsic functional properties of innate, multi-specific Abs, healthy children and youngsters are NOT ‘naturally’ susceptible to any Sars-CoV-2 lineage but exclusively acquire such susceptibility as a direct consequence of functional suppression of their well-established innate immune capacity due to a rapid re-exposure event or, even much worse and long-lived, due to vaccination. The likelihood of rapid re-exposure to Sars-CoV-2 after previous infection dramatically increases when highly infectious variants expand in prevalence. Such an expansion in prevalence directly results from mass vaccination campaigns as mass vaccination turns vaccinees into an excellent breeding ground for naturally selected S-directed immune escape variants.
So, unless there is any contradiction in the above reasoning and unless somebody could explain how similar viral replication and transmission dynamics in vaccinated as compared to unvaccinated individuals could lead to dissimilar clinical manifestations of infection, we can only conclude that the scenario is the following: Vaccination of children and youngsters is turning off their broadly protective innate immunity in exchange for S-specific vaccinal Abs that are becoming increasingly useless since their neutralizing capacity becomes more and more eroded as a result of enhanced escape of Sars-CoV-2 from neutralizing Abs [NAbs](a trend that has been clearly confirmed by molecular epidemiologists (8)). Resistance to the neutralizing effect of vaccinal Abs that are nevertheless still able to bind Sars-CoV-2 virions and thereby outcompete protective innate Abs is likely to enhance the susceptibility of vaccinees to ADE (Ab-dependent enhancement of disease).
Unless virology and immunology are being rewritten, I cannot imagine how mass vaccination of our youngsters and children will not lead to an even more disastrous outcome of all the scientifically irrational and unjustifiable vaccination efforts. Not only will this dramatically increase the children’s risk to succumb to (accelerated) Covid-19 disease but it will also take away the highly efficient capacity of healthy, unvaccinated people to diminish the dangerous, ever rising viral infectious pressure in the population. By vaccinating our youngsters, children and, even more generally, all people in excellent health, we deprive an important part of the population from its ‘anti-viral’ capacity and instead turn them into a breeding ground for more infectious and increasingly NAb-resistant variants. In other words, mass vaccination of children will inevitably obstruct the process of building herd immunity in the population. While unvaccinated children who contract Covid-19 disease in the vast majority of cases don’t suffer severe disease and contribute to the buildup of herd immunity in the population, mass vaccination campaigns in children will prevent them from contributing to herd immunity, because more infectious viral variants are increasingly escaping from neutralization by vaccinal anti-S Abs and gaining a significant fitness advantage in such an immunological environment.
There can be no doubt that large scale immune interventions which ignore the immune pathogenesis of the disease are recipes for massive disasters.
It cannot be that highly knowledgeable vaccinologists don’t understand this clear-cut message. I can only shout at all of them, no matter their international reputation, the number of awards and recognitions they’ve gotten, the number of books they’ve written or high-ranked papers they’ve published in peer-reviewed journals: shame on you for not standing up
(1) https://www.medrxiv.org/content/10.1101/2021.09.28.21264262v2
(2) except for those born with rare genetic deficiencies of innate immune effector genes
(3) https://www.geertvandenbossche.org/post/c-19-pandemia-quo-vadis-homo-sapiens: page 1-2 and https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7772470/pdf/fimmu-11-610300.pdf
(4) https://www.medrxiv.org/content/10.1101/2021.09.28.21264262v2
(5) see references from the literature on website www.geertvandenbossche.org under topic 1
(6) https://www.geertvandenbossche.org/post/c-19-pandemia-quo-vadis-homo-sapiens: page 1-2
(7) As the protective capacity of the vaccinal Abs is now increasingly waning, claims on vaccine-induced protection have been toned down to ‘protection from severe disease’ only.
(8) https://pubmed.ncbi.nlm.nih.gov/33688681/
*
https://boriquagato.substack.com/p/the-vaccinated-superspread-hypothesis
+
*
*
https://rumble.com/vhp7y5-full-interview-world-renowned-doctor-blows-lid-off-of-covid-vaccine.html
Dr. Peter McCullough discusses the dangers of the novel COVID vaccine and it's roll out. This is a product that had minimal testing but is being pushed on the masses. Must we all get the shot for things to "go back to normal"? Are you going to get the shot?
*Fleccas is not giving any medical advice here ;-)
Dr. Peter McCullough has been the world's most prominent and vocal advocate for early outpatient treatment of SARS-CoV-2 (COVID-19) Infection in order to prevent hospitalization and death. On May 19, 2021, he was interviewed regarding his efforts as a treating physician and researcher. From his unique vantage point, he has observed and documented a PROFOUNDLY DISTURBING POLICY RESPONSE to the pandemic -- a policy response that may prove to be the greatest malpractice and malfeasance in the history of medicine and public health.
Dr. McCullough is an internist, cardiologist, epidemiologist, and Professor of Medicine at Texas A & M College of Medicine, Dallas, TX USA. Since the outset of the pandemic, Dr. McCullough has been a leader in the medical response to the COVID-19 disaster and has published “Pathophysiological Basis and Rationale for Early Outpatient Treatment of SARS-CoV-2 (COVID-19) Infection” the first synthesis of sequenced multidrug treatment of ambulatory patients infected with SARS-CoV-2 in the American Journal of Medicine and subsequently updated in Reviews in Cardiovascular Medicine. He has 40 peer-reviewed publications on the infection and has commented extensively on the medical response to the COVID-19 crisis in TheHill and on FOX NEWS Channel. On November 19, 2020, Dr. McCullough testified in the US Senate Committee on Homeland Security and Governmental Affairs and throughout 2021 in the Texas Senate Committee on Health and Human Services, Colorado General Assembly, and New Hampshire Senate concerning many aspects of the pandemic response.
Peter A. McCullough, MD, MPH, FACP, FACC, FAHA, FCRSA, FCCP, FNKF, FNLA
Professor of Medicine, Texas A & M College of Medicine
Board Certified Internist and Cardiologist
President Cardiorenal Society of America
Editor-in-Chief, Reviews in Cardiovascular Medicine
Editor-in-Chief, Cardiorenal Medicine
Senior Associate Editor, American Journal of Cardiology
For more information about Dr. McCullough, please visit: heartplace.com/dr-peter-a-mcculloughPeter A. McCullough, MD, MPH, FACP, FACC, FAHA, FCRSA, FCCP, FNKF, FNLA
*
https://www.youtube.com/watch?app=desktop&v=gnB8Tep92Us&feature=youtu.be#dialog
Dokaz trditev dr.Bosscha (od 21.00 minute)
*
*
Bocvanske oblasti poročajo, da se je nova afriška varianta OMICRON (B.1.1.529 ) razvila na cepljenih osebah.
Do cross-reactive T cells explain mild course of Omicron infection?
*
Geert Vanden Bossche je doktoriral na Univerzi v Gentu v Belgiji ter nato iz virologije na Univerzi Hohenheim v Stuttgartu, Nemčija. Bil je zaposlen kot profesor na univerzah v Belgiji in Nemčiji. Po končani akademski karieri se je pridružil več podjetjem za proizvodnjo cepiv (GSK Biologicals, Novartis Vaccines, Solvay Biologicals) in opravljal različne funkcije na področju raziskav in razvoja cepiv ter poznega razvoja cepiv. Nato se je pridružil ekipi Global Health Discovery fundacije Billa in Melinde Gates v Seattlu (ZDA) ter nato Globalnemu združenju za cepiva in cepljenje (GAVI) v Ženevi kot višji vodja programa za ebolo. Po delu za GAVI se je pridružil Nemškemu centru za raziskave okužb v Kölnu kot vodja urada za razvoj cepiv.
V nadaljevanju tega zapisa objavljam prevod njegovega javnega poziva Svetovni zdravstveni organizaciji (WHO).*
“kolegi iz SZO, mislim, da je napočil čas za priznanje, da je bil program množičnega cepljenja, ki ste ga predlagali z namenom, da bi končali pandemijo COVID-19, popolnoma neuspešen. Na začetku letošnjega leta sem vas pozval, da začnete znanstveno razpravo o morebitnih tveganjih množičnega cepljenja s temi cepivi – sredi pandemije. Na to zahtevo nisem prejel nobenega odgovora. Kmalu zatem pa mi je eden najbolj priznanih vakcinologov na tem planetu napisal elektronsko sporočilo, v katerem je zapisal; “cepljenje s temi cepivi bi samo vzgojilo nove različice, vendar ni smiselno, da bi “plaval proti toku”, ker me tako ali tako nihče ne bi poslušal. Upam, da bodo cepiva druge generacije rešila problem.”
Zato sem vam želel sporočiti, da si ne morete privoščiti ne upoštevati mnenja ljudi, ki imajo dolgoletno strokovno znanje in izkušnje z različnih relevantnih področij, povezanih s to pandemijo: virologije, imunologije, vakcinologije, evolucijske biologije, epidemiologije, zoonoz in podobno. Medtem ko smo nekateri napovedovali, da bo množično cepljenje s temi cepivi sredi pandemije neizogibno privedlo do širjenja bolj nalezljivih različic, so vaši vodilni znanstveniki pridigali poenostavljeno mantro, ki je v tem, da bolj kot bomo cepili, manj se bo virus razmnoževal in manjša bo verjetnost, da se bodo pojavile nove različice. Posledice teh poenostavljenih in napačnih stališč so, da imamo danes opravka s prevladujočim kroženjem virusa Omicron, najbolj nalezljive različice SARS-CoV-2, ki smo ji bili priča do sedaj.
Glede na to, da imamo opravka s številnimi sevi, ki krožijo ter številnimi njihovimi podrazličicami, glede na dejstvo, da so stopnje okužb zelo visoke in da imamo verjetno že več živalskih populacij, ki služijo kot rezervoar za virus, je verjetnost, da se virusne različice zdaj rekombinirajo in ustvarjajo reasortimente znotraj enega in istega gostitelja, vse bolj verjetna. To pomeni, da bo vedno težje izslediti izvor novih sevov in da bo še težje napovedati značilnosti teh novih sevov v smislu kužnosti, virulence, patogenosti in tudi v smislu odpornosti na cepilna protitelesa ali na cepiva na splošno.
*
Mar 06, 2021
