VIR: https://scivisionpub.com/pdfs/covid19-rna-based-vaccines-and-the-risk-of-prion-disease-1503.pdf
Raziskovalni članek ISSN 2639-9458
Microbiology & Infectious Diseases
Vol.5 Izvod št.1 letnik 2021
COVID-19 cepiva na osnovi mRNA in tveganje za prionsko bolezen
Classen Immunotherapies, Inc., 3637 Rockdale Road, Manchester, MD 21102,
E-mail: classen@vaccines.net.
Korespondenca: J. Bart Classen, MD* Classen Immunotherapies, Inc., 3637 Rockdale Road, Manchester, MD 21102, Tel: 410-377-8526.
Prejeto: 27. december 2020 Sprejeto: 18. januar 2021
Navedba: Classen JB. COVID-19 RNA Based Vaccines and the Risk of Prion Disease. Microbiol Infect Dis. 2021; 5(1): 1-3.
Raziskovalni članek
POVZETEK
Razvoj nove tehnologije cepiv je v preteklosti imel težave. Sedanja cepiva za SARS CoV-2 na osnovi RNK so bila odobrena v ZDA z dovoljenjem v izrednih razmerah brez obsežnega dolgoročnega preskušanja varnosti. V tem dokumentu je bilo cepivo Pfizer za COVID-19 ovrednoteno glede možnosti, da pri prejemnikih cepiva povzroči prionsko bolezen.
Analizirali so zaporedje RNK v cepivu in ciljno interakcijo proteinov beljakovinske bodice za možnost spremembe intraceličnih beljakovin TAR za vezavo RNK, beljakovin TDP-43 za vezavo DNK in beljakovin za vezavo FUS (Fused in Sarkoma) v svoje patološke prionske prilagoditve. Rezultati kažejo, da ima RNK iz cepiva specifična zaporedja, ki lahko povzročijo, da se beljakovine TDP-43 in FUS zložijo v svoje patološke prionske oblike. V sedanji analizi je bilo ugotovljenih skupno šestnajst ponovitev dvojic UG (ΨGΨG) in ugotovljenih je bilo nekaj dodatnih sekvenc z veliko UG (ΨG). Najdeni sta bili dve sekvenci GGΨA. Možno je tudi, da so navzoče potencialne G Quadruplex sekvence, a za potrditev le teh je potreben bolj dovršen računalniški program. Nadalje, beljakovinska bodica, ki je ustvarjena s prevajanjem RNK iz cepiva, veže angiotenzin pretvarjajoči encim 2 (ACE2), encim, ki vsebuje cink. Ta interakcija ima možnost povečati znotrajcelični cink. Cink ioni so pokazali, da povzročajo preoblikovanje TDP-43 v njegovo patološko prionsko konfiguracijo. Znano pa je, da cinkovi ioni povzročijo transformacijo beljakovine TDP-43 v njeno patološko prionsko konfiguracijo.
Ugotovljeno je bilo, da zlaganje beljakovin TDP-43 in FUS v njihove patološke prionske oblike povzroči ALS (amiotrofično lateralno sklerozo), degeneracijo sprednjega temporalnega režnja, Alzheimerjevo bolezen in druge nevrološke degenerativne bolezni.
Zaradi teh ugotovitev in dodatnih možnih tveganj avtor meni, da je bila regulativna odobritev cepiv za SARS COV-2 na osnovi RNK prezgodnja in da lahko to cepivo povzroči veliko več škode kot koristi.
Ključne besede: COVID-19, cepiva, diabetes, imunost
UVOD
Ugotovili so, da cepiva povzročajo veliko kroničnih, pozno razvijajočih se neželenih dogodkov. Nekateri neželeni učinki, kot je sladkorna bolezen tipa 1, se lahko pojavijo šele 3-4 leta po prejemu cepiva [1].
V primeru sladkorne bolezni tipa 1 lahko pogostnost primerov neželenih dogodkov presega pogostnost primerov hude nalezljive bolezni, katere preprečevanju je bilo namenjeno cepivo. Glede na to, da je sladkorna bolezen tipa 1 le ena od številnih imunsko posredovanih bolezni, ki jih lahko povzročijo cepiva, so kronični, pozno pojavljeni neželeni učinki resen javno zdravstveni problem.
Prihod nove tehnologije cepiva ustvarja nove potencialne mehanizme neželenih učinkov cepiva. Na primer, prvo cepivo z mrtvim virusom proti otroški paralizi je dejansko povzročilo paralizo pri prejemnikih, ker proizvodni proces ni učinkovito ubil virusa paralize, preden je bil injiciran v bolnike.
Cepiva na osnovi RNK pomenijo posebna tveganja za povzročitev posebnih neželenih učinkov. En tak potencialni neželeni dogodek so prionske bolezni, ki jih povzroča cepivo z aktivacijo intrinstičnih beljakovin, da tvorijo prione.
Veliko znanja je bilo objavljenega o vrsti beljakovin, ki vežejo RNK in ki kot kaže sodelujejo pri povzročanju številnih nevroloških bolezni, vključno z Alzheimerjevo boleznijo in ALS. TDP-43 in FUS spadata med najbolje raziskane tovrstne beljakovine [2].RNK cepivo Pfizer za COVID-19 je odobrila ameriška Uprava za hrano in zdravila (FDA) z dovoljenjem za uporabo v sili brez dolgoročnih varnostnih podatkov. Zaradi pomislekov glede varnosti tega cepiva je bila opravljena ta študija, da se ugotovi, ali lahko cepivo povzroči bolezen na osnovi prionov.
METODE
Pfizerjevo cepivo proti COVID-19 na osnovi RNK je bilo ocenjeno za možnost pretvorbe beljakovin TDP-43 in ali FUS v njune prionske oblike, ki povzročajo bolezen. RNK cepivo so analizirali za prisotnost sekvenc, ki lahko aktivirajo TDP-43 in FUS. Analizirana je bila interakcija prepisane beljakovinske bodice z njeno tarčo, da bi ugotovili, ali lahko to delovanje aktivira tudi TDP-43 in FUS.
REZULTATI
Analiza cepiva Pfizer proti COVID-19 je pokazala, da sta dva možna dejavnika tveganja za indukcijo prionske bolezni pri človeku. Zaporedje RNK v cepivu [3] vsebuje sekvence, ki naj bi povzročile, da se beljakovini TDP-43 in FUS zložita v prionsko obliko, kar vodi do razvoja znanih nevrodegerativnih bolezni.
Zlasti se je izkazalo, da RNK sekvence GGUA [4], sekvence z veliko UG [5], sekvence s ponovitvami dvojic UG [6] in z zaporedji G Quadruplex [7], imajo povečano afiniteto za vezavo TDP-43 in/ ali FUS in lahko povzročijo, da se TDP-43 ali FUS zložijo v svoje patološke konfiguracije u citoplazmi. V sedanji analizi je bilo ugotovljenih skupno šestnajst ponovitev dvojic UG (ΨGΨG) in ugotovljenih je bilo nekaj dodatnih sekvenc z veliko UG (ΨG). Najdeni sta bili dve sekvenci GGΨA. Možno je tudi, da so navzoče potencialne G Quadruplex sekvence, a za potrditev le teh je potreben bolj dovršen računalniški program.
Beljakovinska bodica (spike protein), ki je kodiran s cepivom, veže angiotenzin pretvarjajoči encim 2 (ACE2), encim, ki vsebuje cinkove molekule [8]. Vezava beljakovinske bodice na ACE2 ima možnost sproščanja molekule cinka - iona, ki sproži patološko prionsko transformacijo beljakovine TDP-43.[9].
RAZPRAVA
V medicini obstaja star pregovor, da je zdravilo lahko slabše od bolezni. Stavek se lahko uporablja za cepiva. V sedanjem dokumentu je izražena zaskrbljenost, da imajo cepiva za COVID-19 na osnovi RNK možnost, da povzročijo več bolezni kot epidemija COVID-19. Ta dokument se osredotoča na nov potencialni mehanizem škodljivih dogodkov, ki povzroča prionsko bolezen, ki bi lahko bila še pogostejša in težja od virusne okužbe, ki naj bi jo cepivo preprečevalo. Medtem ko se ta dokument osredotoča na en potencialni neželeni dogodek, obstaja več drugih potencialnih usodnih neželenih dogodkov, kot bo obravnavano v nadaljevanju.
V zadnjih dveh desetletjih je bila med nekaterimi znanstveniki zaskrbljenost, da bi se lahko prioni uporabljali kot biološko orožje. V zadnjem času obstaja zaskrbljenost, da bi lahko aktivirali vseprisotne znotraj celične molekule, da bi povzročile prionsko bolezen, vključno z Alzheimerjem, amiotrofično lateralno sklerozo (ALS) in druge nevrodegenerativne bolezni. Ta skrb izvira zaradi možnosti zlorabe raziskovalnih podatkov o mehanizmih, s katerimi je mogoče aktivirati nekatere beljakovine, ki vežejo RNK, kot so TDP-43, FUS in druge, da bi le te oblikovale prione, ki povzročajo bolezni.
Skrb vzbuja tudi dejstvo, da te raziskave, ki bi jih lahko uporabili za razvoj biološkega orožja, financirajo zasebne organizacije, vključno s Fundacijo Billa in Melinde Gates in Ellison Medical Foundation [2] brez nacionalnega/mednarodnega nadzora.
V preteklosti so na primer obstajale prepovedi objavljanja informacij v zvezi z gradnjo jedrskih bomb. Objavljeni podatki so pokazali, da obstaja več različnih dejavnikov, ki lahko prispevajo k pretvorbi nekaterih beljakovin za vezavo RNK, vključno s TDP-43, FUS in z njimi povezanimi molekulami v njihova patološka stanja. Te beljakovine, ki vežejo RNK, imajo veliko funkcij in se nahajajo tako v jedru kot v citoplazmi. Te vezavne beljakovine imajo aminokislinska področja - vezivne motive, ki vežejo specifične RNK sekvence.
Vezava na določena zaporedja RNK, kadar so beljakovine v citoplazmi, naj bi povzročila, da se molekule zložijo na določene načine, ki vodijo do patološke agregacije in nastanek prionov v citoplazmi [2]. Trenutna analiza kaže, da Pfizerjevo cepivo za COVID-19 na osnovi RNK vsebuje veliko takšnih sekvenc RNK, za katere se je izkazalo, da imajo visoko afiniteto za beljakovine TDP-43 ali FUS in lahko povzročijo kronične degenerativne nevrološke bolezni.
Vezava cinka na motiv RNK za prepoznavanje beljakovine TDP-43 je še en mehanizem, ki vodi v nastanek amiloidom podobnih agregatov [9]. Virusna beljakovinska bodica, ki jo kodira sekvenca RNK iz cepiva, veže ACE2 encim, ki vsebuje cinkove molekule [8]. Ta interakcija lahko poveča raven znotraj celičnega cinka, kar vodi do prionske bolezni.
Začetna vezava je lahko med beljakovinskimi bodicami na površini celice, ki se prenašajo s cepivom in ACE2 na površini sosednje celice. Posledični kompleks se lahko ponotranji. Druga možnost je, da bi se interakcija sprva lahko zgodila v citoplazmi celice, ki izdeluje ACE2 in je bila okužena z RNK kodiranjem beljakovinske bodice iz cepiva.
Interakcija je precej zaskrbljujoča glede na prepričanje, da je virus SARS CoV-2, ki povzroča COVID-19, biološko orožje [10,11] in možno je, da je virusna beljakovinska bodica zasnovana tako, da povzroči prionsko bolezen.
Druga, s tem povezana skrb je, da Pfizer cepivo uporablja edinstven RNK-nukleozid 1-metil-3'-pseudouridilil (Ψ) (RNA nucleoside 1-methyl-3'-pseudouridylyl). V skladu z dokumenti FDA je bil ta nukleozid izbran za zmanjšanje aktivacije naravnega (prirojenega) imunskega sistema [12]. Molekule RNK, ki vsebujejo ta nukleozid, bodo nedvomno spremenile vezavo [13].
Na žalost ni objavljen učinek na TDP-43, FUS in druge beljakovine, ki vežejo RNK.
Uporaba tega nukleozida v cepivu lahko potencialno poveča vezalno afiniteto sekvenc RNK, ki lahko povzročijo, da beljakovini TDP-43 in FUS prevzameta strupene konfiguracije.
Obstaja veliko drugih možnih neželenih dogodkov, ki jih lahko povzročijo nova cepiva proti COVID-19, ki temeljijo na RNK. Cepivo v/na površino gostiteljskih celic postavi novo molekulo - beljakovinsko bodico. Ta beljakovinska bodica je potencialni receptor za drugi,
nov infektivni agent.
Če imajo prav tisti, ki trdijo, da je COVID-19 dejansko biološko orožje, potem se lahko sprosti drugi potencialno nevarnejši virus, ki veže beljakovinske bodice, ki jih najdemo na gostiteljskih celicah prejemnikov cepiva. Podatki, ki bi dali informacije o tem, kako dolgo se RNK cepivo prevaja pri prejemniku cepiva in koliko časa po prevajanju bodo beljakovinske bodice prisotne v celicah prejemnika, niso javno dostopni.
Take študije, ki se nanašajo na izraz »in vivo«, bodo zapletene in zahtevne. Genetska raznolikost ščiti vrste pred množičnim žrtvam, ki so jih povzročili infektivni agenti. Enega posameznika lahko virus ubije, pri drugem pa isti virus nima nobenih škodljivih učinkov.
Z dajanjem identičnega receptorja, beljakovinske bodice, na celice vseh v populaciji, izgine genetska raznolikost za vsaj en potencialni receptor. Vsi v populaciji zdaj postanejo potencialno dovzetni za vezavo z istim nalezljivim agentom.
Avtoimunost in nasprotno stanje, metabolni sindrom, sta dobro poznana neželena dogodka, ki ju povzročajo cepiva [14]. Okužbe s COVID-19 so povezane z indukcijo avto- protiteles in avtoimunskih bolezni [15,16], zaradi česar bi zagotovo tudi cepivo povzročilo takšna stanja. En avtor je ugotovil, da so zaporedja aminokislin v virusnih beljakovinskih bodicah enake sekvencam v človeških beljakovinah, vključno z beljakovinami, ki jih najdemo v centralnem živčnem sistemu [17].
Avtoimunost lahko povzroči tudi epitopsko širjenje, ko je tuj antigen (kot je beljakovinska bodica) predstavljen s celico, ki predstavlja antigen, ki ima tudi svoje molekule pritrjene na njegove molekule MHC. Nazadnje, drugi, ki delajo na tem področju, so objavili dodatno podporo podatkom, da bi cepiva proti COVID-19 lahko povzročila prionsko bolezen.
Avtorji [18] so v beljakovinskih bodicah COVID-19 našli s prioni povezana zaporedja, katerih niso našli v sorodnih koronavirusih.
Drugi [19] so poročali o primeru prionske bolezni, Creutzfeldt-Jakobove bolezni (op. prev. bolezen norih krav), ki se je sprva pojavila pri človeku s COVID-19. Mnogi so opozorili, da je trenutna epidemija COVID-19 dejansko posledica napada biološkega orožja, ki so ga delno sprostili posamezniki iz vlade ZDA. [10,11].
Taka teorija ni daleč od resnice, glede na to, da je napad antraksa leta 2001 v ZDA izviral iz Fort Detricka, objekta za biološko orožje vojske ZDA. Ker je FBI preiskava napada antraksa bila zaključena v nasprotju z nasvetom vodilnega agenta FBI, je zelo verjetno, da zarotniki še vedno delujejo v vladi ZDA. V takem scenariju mora biti primarni poudarek ustavljanja napada biološkega orožja ta, da se ujamejo zarotniki, sicer se napadi nikoli ne bodo prenehali. Odobritev cepiva, z uporabo nove RNK tehnologije brez obsežnih testiranj, je izredno nevarna. Cepivo je lahko biološko orožje in še bolj nevarno od prvotne okužbe.
* * *
This is especially concerning since the Pfizer vaccine is an mRNA vaccine, an untested type of vaccine which creates new proteins and can actually integrate into the human genome, according to a report from the National Library of Medicine. In other words, degenerative brain conditions may appear at any time in your life after receiving the vaccine.
“The RNA sequence of the vaccine as well as the spike protein target interaction were analyzed for the potential to convert intracellular RNA binding proteins TAR DNA binding protein (TDP-43) and Fused in Sarcoma (FUS) into their pathologic prion conformations,” explains the report. TDP-43 is a protein known to cause dementia, ALS and even Alzheimer’s, according to Alzpedia. Similarly, the FUS protein is known to cause ALS and Hereditary Essential Tremors, according to the Human Genome Database.
The experiment done for the report was to determine whether or not these two harmful proteins embed themselves into our DNA, as an mRNA vaccine is expected to do. The report determined that “the vaccine RNA has specific sequences that may induce TDP-43 and FUS to fold into their pathologic prion confirmations,” meaning that both proteins have the potential to embed themselves into our DNA and cause harmful neurological diseases.
The report’s abstract summary concludes that “The enclosed finding as well as additional potential risks leads the author to believe that regulatory approval of the RNA based vaccines for SARS-CoV-2 was premature and that the vaccine may cause much more harm than benefit.” The report itself ends with this warning: “The vaccine could be a bioweapon and even more dangerous than the original infection.”
National File actually reached out to the CDC to inquire as to why the Pfizer vaccine is still being distributed despite these credible allegations. No response was received prior to publication.
https://nationalfile.com/report-pfizer-vaccine-confirmed-to-cause-neurodegenerative-diseases/
* * *
SARS-CoV-2 RNA reverse-transcribed and integrated into the human genome
- PMID: 33330870
- PMCID: PMC7743078
- DOI: 10.1101/2020.12.12.422516
Abstract
Prolonged SARS-CoV-2 RNA shedding and recurrence of PCR-positive tests have been widely reported in patients after recovery, yet these patients most commonly are non-infectious. Here we investigated the possibility that SARS-CoV-2 RNAs can be reverse-transcribed and integrated into the human genome and that transcription of the integrated sequences might account for PCR-positive tests. In support of this hypothesis, we found chimeric transcripts consisting of viral fused to cellular sequences in published data sets of SARS-CoV-2 infected cultured cells and primary cells of patients, consistent with the transcription of viral sequences integrated into the genome. To experimentally corroborate the possibility of viral retro-integration, we describe evidence that SARS-CoV-2 RNAs can be reverse transcribed in human cells by reverse transcriptase (RT) from LINE-1 elements or by HIV-1 RT, and that these DNA sequences can be integrated into the cell genome and subsequently be transcribed. Human endogenous LINE-1 expression was induced upon SARS-CoV-2 infection or by cytokine exposure in cultured cells, suggesting a molecular mechanism for SARS-CoV-2 retro-integration in patients. This novel feature of SARS-CoV-2 infection may explain why patients can continue to produce viral RNA after recovery and suggests a new aspect of RNA virus replication.
https://pubmed.ncbi.nlm.nih.gov/33330870/
* * *
SARS-CoV-2 Prion-Like Domains in Spike Proteins Enable Higher Affinity to ACE2

Abstract
Dr. Stephanie Seneff (MIT): Nevrodegenerativne bolezni in COVID-19 cepiva:
https://stephanieseneff.net/sars-cov-2-vaccines-and-neurodegenerative-disease/
Since December 2020, when several novel unprecedented vaccines against SARS-CoV-2 began to be approved for emergency use, there has been a worldwide effort to get these vaccines into the arms of as many people as possible as fast as possible. These vaccines have been developed “at warp speed,” given the urgency of the situation with the COVID-19 pandemic. Most governments have embraced the notion that these vaccines are the only path towards resolution of this pandemic, which is crippling the economies of many countries.
Thus far, there are four different vaccines that have been approved for emergency use for protection against COVID-19 in the US and/or Europe. Two (the Moderna vaccine and the Pfizer/BioNTech vaccine) are based on mRNA technology, whereas the other two (produced by Johnson & Johnson and AstraZeneca) are based on a double-stranded DNA recombinant viral vector. The mRNA vaccines contain only the code for the SARS-CoV-2 envelope spike protein, whereas the DNA-based vaccines both contain an adenovirus viral vector that has been augmented with DNA that codes for the SARS-CoV-2 spike protein. The DNA-based vaccines have a certain advantage over the RNA-based vaccines in that they do not have to be stored at deep-freeze temperatures, because double-stranded DNA is much more stable than single-stranded RNA. But a disadvantage is that those who have been exposed to natural forms of the adenovirus have antibodies to the virus that will likely block the synthesis of the spike protein, and therefore not afford protection against SARS-CoV-2.
In this regard, the AstraZeneca (AZ) vaccine has a slight advantage over the Johnson & Johnson (J&J) vaccine because the virus normally infects chimpanzees rather than humans, so fewer people are likely to have been exposed to it [1, 2]. On the other hand, several studies have shown that viruses that normally infect one species can cause tumors if they are injected into a different species. For example, a human adenovirus injected into baboons caused retinoblastoma (cancer of the eye) in the baboons [3]. So, it can’t be ruled out that the AZ vaccine could lead to cancer.
People don’t realize that these vaccines are vastly different from the many childhood vaccines we are now used to getting early in life. I find it shocking that the vaccine developers and the government officials across the globe are recklessly pushing these vaccines on an unsuspecting population. Together with Dr. Greg Nigh, I recently published a peer-reviewed paper on the technology behind the mRNA vaccines and the many potentially unknown consequences to health [4]. Such unprecedented vaccines normally take twelve years to develop, with only a 2% success rate, but these vaccines were developed and brought to market in less than a year. As a consequence, we have no direct knowledge of any effects that the vaccines might have on our health over the long term. However, knowledge about how these vaccines work, how the immune system works and how neurodegenerative diseases come about can be brought to bear on the problem in order to predict potential devastating future consequences of the vaccines.
The mRNA in these vaccines codes for the spike protein normally synthesized by the SARS-CoV-2 virus. However, both the mRNA and the protein it produces have been changed from the original version in the virus with the intent to increase rate of production of the protein in an infected cell and the durability of both the mRNA and the spike protein it codes for. Additional ingredients like cationic lipids and polyethylene glycol are also toxic with unknown consequences. The vaccines were approved for emergency use based on grossly inadequate studies to evaluate safety and effectiveness.
Our paper showed that there are several mechanisms by which these vaccines could lead to severe disease, including autoimmune disease, neurodegenerative diseases, vascular disorders (hemorrhaging and blood clots) and possibly reproductive issues. There is also the risk that the vaccines will accelerate the emergence of new strains of the virus that are no longer sensitive to the antibodies produced by the vaccines. When people are immune compromised (e.g., taking chemotherapy for cancer), the antibodies they produce may not be able to keep the virus in check because the immune system is too impaired. Just as in the case of antibiotic resistance, new strains evolve within an infected immune-compromised person’s body that produce a version of the spike protein that no longer binds with the acquired antibodies. These new strains quickly come to dominate over the original strain, especially when the general population is heavily vaccinated with a vaccine that is specific to the original strain. This problem is likely going to necessitate the repeated rollout of new versions of the vaccine at periodic intervals that people will have to receive to induce yet another round of antibody production in an endless game of cat and mouse.
Like the mRNA vaccines, the DNA vaccines are based on novel biotech gene editing techniques that are brand new, so they too are a massive experiment unleashed on a huge unsuspecting population, with unknown consequences. Both DNA vector vaccines have been associated with a very rare condition called thrombocytopenia, in which platelet counts drop precipitously, resulting in system-wide blood clots and a high risk of cerebral hemorrhaging [5]. This is likely due to an autoimmune reaction to the platelets, and it comes with a high risk of mortality. In the case of the AZ vaccine, this has caused over 20 European countries to temporarily pause their vaccination programs [6]. And the United States called a temporary halt on the J&J vaccine.
Even experts don’t really understand the mechanism as of now, although a fascinating theory to explain this depends on the fact that DNA vector vaccines require the DNA to be copied into RNA in the nucleus, and this presents the possibility of producing an incomplete copy, generated through “splice variants,” that is missing the code for attaching to the membrane [7]. These soluble partial sequences wander off to other parts of the body and bind to ACE2 receptors throughout the vasculature. Antibodies to these ACE2-bound partial spike fragments cause an acute inflammatory response that results in disseminated intravascular coagulation (DIC).
How to Make an Adenovirus DNA Vector Vaccine
The adenovirus vaccines are created through techniques that the average citizen can’t possibly fathom could even exist. For the AZ vaccine, the bulk of the DNA in the vaccine codes for the various proteins that are needed by a strain of adenovirus that mainly infects chimpanzees and causes cold-like symptoms [1]. However, it is not a “normal” version of this cold virus. First of all, it has been stripped of certain genes that it needs in order to replicate, and for this reason it is referred to as an “adenovirus vector.” This defect, it is argued, keeps it from actually infecting the vaccinated patient. Secondly, it is modified, through gene editing techniques, to create a recombinant version of the virus that contains the complete coding sequence for the SARS-CoV-2 spike protein, spliced into its DNA sequence – the same protein that the RNA vaccines code for. The recombinant DNA is a linear double-stranded DNA sequence where proteins from two different species are integrated through gene editing.
Since this virus can’t proliferate, it is difficult to manufacture large quantities of it. But they solved this problem by making use of a genetically modified version of a human cell line, called HEK (human embryonic kidney) 293 cells, where the human cell’s DNA was transfected long ago with fragments of the genome of an adenovirus – conveniently providing the defective recombinant virus with the missing proteins it needs to be able to proliferate [8]. Within a culture of these HEK 293 cells, the virus can replicate, assisted by the proteins that are produced by the host cells. The HEK 293 cells originally came from a kidney of an aborted fetus, and it has been maintained in culture ever since the 1970s, because it was modified to become immortal, with the help of the adenovirus. Although it was obtained from a kidney, it is not a kidney cell. In fact, it has many properties that are characteristic of a neuronal stem cell [9]. The fact is, they don’t really know what kind of cell it is. The ability of a cell line to survive indefinitely is a feature of tumor cells. Although the vaccine is “purified” during the processing, there is no guarantee that it is not contaminated with remnants from the host cells, i.e., human DNA of a neuronal tumor cell line. It does not seem like a good idea to inject the DNA of a human tumor cell into anyone.
The J&J vaccine has a very similar manufacturing process, except with a different adenovirus strain and a different human host cell. For J&J, the host cell is another fetal cell line harvested long ago and made immortal through the incorporation of adenovirus genes into the host human genome. This cell line was taken from the retina of the eye of the fetus.
The Spike Protein is Toxic
The COVID-19 vaccines are all based on supplying genetic code to produce the spike protein that is the main constituent of the SARS-CoV-2 protein cage that encloses its RNA contents. Both the DNA vector and the RNA vaccines induce the vaccine-infected cell to manufacture many copies of the spike protein according to the code. Through experimentation, researchers have determined that the spike protein is toxic even when introduced all by itself. In a revealing experiment, researchers injected spike protein into hamsters, and found that it was taken up by endothelial cells lining the blood vessels, via ACE2 receptors [10]. This caused a downregulation of ACE2, which had significant effects on the metabolic policy in the cells. In particular, it inhibited the synthesis of mitochondria, and caused the existing mitochondria to fragment. Mitochondria are the organelles in the cell that produce large quantities of ATP (the energy currency of cells) by oxidizing nutrients, while consuming oxygen and producing water and carbon dioxide. The spike protein reduced the production of ATP by mitochondria and increased glycolysis — the alternative, much less efficient, way to produce ATP without using oxygen. This metabolic change towards getting energy through glycolysis is a characteristic feature of cancer cells and of neurons in neurodegenerative diseases such as Alzheimer’s.
In another experiment, researchers showed that spike protein can cross the blood-brain barrier in mice and be taken up by neurons throughout the brain [11]. This too is likely mediated by ACE2 receptors (which neurons also produce). These same researchers also showed that spike protein administered in the nose was able to reach the brain by traveling along the olfactory nerve. When they induced inflammation in the brain through exposure to lipopolysaccharide (LPS), they saw an increased uptake of spike protein into the brain, which they hypothesized was caused by increased leakiness in the barrier. As you will see, these points become important when we later consider what happens following a SARS-CoV-2 vaccine, which is designed to induce inflammation.
Many people suffering from COVID-19 have experienced symptoms characteristic of the central nervous system such as headache, nausea, dizziness, fatal brain blood clots and encephalitis. In an advanced 3D microfluid model of the human BBB, researchers in the United States showed that the spike protein by itself disrupts the blood brain barrier by inducing an inflammatory state, and they proposed that this could be the source of such symptoms [12].
A published preprint found widespread expression of ACE2 in many parts of the brain. ACE2 was expressed in astrocytes, pericytes (cells that wrap around the endothelial cells lining capillary walls) and in endothelial cells — and all of these are key components of the blood-brain barrier [13]. Perhaps of even greater concern is that ACE2 was highly expressed in the substantia nigra, a brain-stem nucleus where damaged dopaminergic neurons lead to Parkinson’s disease.
Bell’s Palsy, Autism and Parkinson’s Disease
In a paper aptly titled, “Is COVID-19 a Perfect Storm for Parkinson’s Disease?” researchers made a strong case for the possibility that we will see an increase in Parkinson’s disease in the future, due to the COVID-19 pandemic [14]. They refer to three separate cases where acute Parkinsonism developed shortly after a COVID-19 infection. They proposed that systemic inflammation caused by severe COVID-19 could trigger neuroinflammation in the substantia nigra, killing off dopaminergic neurons. These neurons express high levels of the ACE2 receptor, making them highly vulnerable to the spike protein. A viral infection is known to upregulate α-synuclein, which, in high concentrations, forms soluble oligomers that then precipitate out as fibrils and accumulate within “Lewy bodies” that are tightly linked to Parkinson’s disease. Further corroboration of this idea comes from a paper which demonstrated that an infection with SARS-CoV-2 causes brain inflammation in macaques and induces the formation of Lewy bodies [15].
Parkinson’s disease is the second most common neurodegenerative disorder and the most common neurodegenerative motor disorder. The root cause of nearly 90% of cases remains unknown, but it has been theorized that viral infections are often involved. It can be argued that the loss of a sense of smell and/or taste in association with COVID-19 is a sign of a Parkinsonian link, since this symptom is also an early sign of Parkinson’s disease [16].
The mRNA vaccines appear to disrupt the body’s ability to keep latent viruses from “waking up” and causing disease symptoms. This observation is based on the fact that shingles and facial palsy (Bell’s palsy) are being commonly reported in side-effect reports in the FDA’s Vaccine Adverse Event Reporting System. As of May 21, 2021, over 2500 reports of Bell’s palsy following COVID-19 vaccines had appeared in VAERS. A primary cause of Bell’s palsy is the activation of latent viral infections, most notably Herpes simplex and Varicella zoster, Varicella zoster is also the virus responsible for shingles.
While Bell’s palsy usually resolves over time, there can be some serious longer-term consequences. Pregnant women who are diagnosed with active herpes infections during pregnancy have a 2-fold increased risk of having an autistic male child from that pregnancy [17]. This should make a pregnant woman hesitate to get a SARS-CoV-2 vaccine. Bell’s palsy can also be a risk factor for Parkinson’s disease much later in life. A study on nearly 200 Parkinson’s disease patients compared with age- and gender-matched controls found that six of the Parkinson’s patients had had an earlier diagnosis of Bell’s palsy, whereas none of the control patients had [18]. There’s also a link between autism and Parkinson’s disease. A study on autistic adults over 39 years old found that one third of them had symptoms that meet the criteria for a Parkinson’s diagnosis [19].
Prion Diseases
Prion diseases are a group of severe neurodegenerative diseases that are caused by misfolded prion proteins. The most common prion disease in humans is the always-fatal sporadic Creutzfeldt-Jakob disease (CJD), which accounts for more than 85% of the cases [20]. Prion diseases are more specifically called transmissible spongiform encephalopathies (TSEs), and infection can spread through exposure to misfolded proteins as “infective” agents, without requiring a live pathogen [20]. PrP is the name given to the specific prion protein associated with these TSEs. Misfolded PrP proteins act as a seed or catalyst that then recruits other molecules of PrP to misfold in the same way and glom together into pathogenic fibrils.
MADCOW, the disease that affected a large number of cows in Europe beginning in the 1990s, is probably the best-known TSE. While eating beef from an infected animal is a very rare risk factor, most cases of Creutzfeldt-Jakob disease occur for unknown reasons, and no other risk factors have been identified. A study based in Switzerland confirmed that many patients who died of Creutzfeldt-Jakob disease had detectable levels of a prion protein in their spleen and muscles, in addition to the olfactory lobe and the central nervous system [21]. More generally, diseases involving misfolded PrPs have consistently been found to involve an initial early phase of prion replication in the spleen which happens long before overt symptoms appear [22, 23]. This point becomes important when we consider whether the COVID-19 vaccines might cause prion diseases.
PrP has a unique feature that it contains multiple copies of a characteristic motif in its amino acid sequence that is called a “GxxxG” motif, also known as a “glycine zipper” [24]. These proteins normally fold into a characteristic shape called an alpha helix, which allows the protein to penetrate the plasma membrane. The glycines in the zipper motif play an essential role in cross-linking and stabilizing alpha helices [25]. This glycine zipper motif is also a common characteristic of many transmembrane proteins (proteins that cross the membrane of the cell).
Indeed, the coronavirus spike protein has a GxxxG motif in its transmembrane domain (specifically, GFIAG — glycine, phenylalanine, isoproline, alanine, glycine) [26]. There is a platform called “Uniprot” where you can look up the sequence of specific proteins. The Uniprot entry for the SARS-CoV-2 spike protein has five glycine zipper sequences altogether [27]. According to J. Bart Classen, the SARS-CoV-2 spike protein has the ability “to form amyloid and toxic aggregates that can act as seeds to aggregate many of the misfolded brain proteins and can ultimately lead to neurodegeneration.” [28]
Many neurodegenerative diseases have been linked to specific proteins that have prion-like properties, and these diseases are characterized as protein-misfolding diseases or proteopathies [29]. Like PrP, prion-like proteins become pathogenic when their alpha helices misfold as beta sheets, and the protein is then impaired in its ability to enter the membrane. These diseases include Alzheimer’s, amyotrophic lateral sclerosis (ALS), Huntington’s disease and Parkinson’s disease, and each of these is associated with a particular protein that misfolds and accumulates in inclusion bodies in association with the disease. We already saw that Parkinson’s disease is characterized by Lewy bodies in the substantia nigra that accumulate misfolded α-synuclein.
Glycines within the glycine zipper transmembrane motifs in the amyloid beta precursor protein (APP) play a central role in the misfolding of amyloid beta linked to Alzheimer’s disease (Decock et al., 2016). APP contains a total of four GxxxG motifs (one fewer than the spike protein).
A case study presented the case of a man who developed CKD simultaneously with symptomatic COVID-19. The authors proposed that infection with SARS-CoV-2 precipitates or accelerates neurodegenerative diseases [30]. A theoretical paper published by researchers in India showed that the spike protein binds to a number of aggregation-prone prion-like proteins, including amyloid beta, α-synuclein, tau, PrP and TDP-43. They argued that this could initiate aggregation of these proteins in the brain, leading to neurodegeneration [31].
Tracing the Vaccine Trail to the Spleen
It is important to understand what happens to the contents of a vaccine after it is injected into the arm. Where does it travel in the body, and what does it do in the places where it settles in?
Vaccine developers are keen to know whether the vaccine induces a strong immune response, reflected in high antibody production against the spike protein, in the case of COVID-19 vaccines. And to do this, they need to trace its movement in the body.
CD8+ T-cells are cytotoxic immune cells that can kill cells that are infected with a virus. They detect an immune complex with viral proteins that are exposed on the surface of an infected cell. A study on an adenovirus-vector based vaccination of mice used clever methods to produce a marker that could track the activity of CD8+ T-cells in the lymph system and the spleen, in the days following vaccination [32]. It can be inferred that immune cells (antigen-presenting cells, where the “antigen” is the spike protein) were initially present at the arm muscle injection site and synthesized the virus spike protein from the vaccine DNA code, exposing it on their surface. Once activated by the foreign protein, they translocated into the draining lymph nodes and finally made their way to the spleen via the lymph system. The CD8+ T-cells are idly waiting within the lymphatics until they spot an infected immune cell. Researchers could detect activation of CD8+ immune cells over time and inferred that this was caused by the arrival of the contents of the vaccine to the site where these immune cells reside. Activated CD8+ T-cells first appeared in the draining lymph nodes, but after five days began to show up in the spleen. Their numbers there peaked sharply by 12 days and then remained high with a slow decay up to 47 days, when the researchers stopped looking. What this means is that the vaccine is picked up by antigen-presenting cells at the injection site and carried to the spleen via the lymph system. The carrier cells then hang out in the spleen for a long time. And this is where the danger lies in terms of the potential to cause prion disease.
In the paper that Greg Nigh and I published recently on the mRNA vaccines, we argued that the mRNA vaccines are rather perfectly set up to produce a very dangerous situation in the spleen that is poised to launch a prion disease. Given the fact that the DNA vector vaccines also end up concentrated in the spleen, I think that the same thing holds true for them as well. The spleen is where the action is for seeding misfolded prion proteins. The vaccine-infected cells have been programmed to produce large amounts of spike proteins. Prion proteins misfold into damaging beta-sheet oligomers when there are too many of them in the cytoplasm. Might the spike protein do the same?
Three out of the four COVID-19 vaccines currently on the market in the U.S. and Europe (Pfizer, Moderna, and J&J) use a genetic code for the spike protein that has been slightly tweaked, in order to produce a more potent antibody response [33]. Normally, after binding to the ACE2 receptor, the spike protein spontaneously changes its shape in a dramatic way in order to fuse with the membrane of the cell. In a Web publication, Ryan Cross described this action very graphically based on a spring-like model, as follows: “When the spike protein binds to a human cell, that spring is released, and the two helices and the loop straighten into one long helix that harpoons the human cell and pulls the virus and human membranes close together until they fuse.” [33]. As Cross explains, through trial and error, but taking structural information into account, researchers came up with the idea of swapping out two adjacent amino acids for prolines in the membrane fusion domain in order to stabilize the shape of the spike protein in its pre-fusion form. In this form, it exposes critical antigenic areas, and this assures more rapid formation of matching antibodies, the only goal of the vaccine design. This also prevents the protein from fusing with the plasma membrane of a host cell. I’d imagine that the spike protein attaches to the ACE2 receptor and then gets stuck there, like a sitting duck. But a worrisome thought is whether this open state, not fused with the membrane, might more closely resemble the shape of a misfolded prion-like protein like amyloid beta than does the collapsed shape it needs to go into the membrane?
Tetz and Tetz have argued in a published online preprint that prion-like domains in the spike protein enable higher affinity for the ACE2 receptor, making the virus more virulent than its earlier cousins [34]. These same authors published an earlier peer-reviewed journal paper where they observed that many other viruses have proteins in their coat that have distinct features of prion proteins [35].
Germinal Centers and Parkinson’s Disease
Germinal centers in the spleen are a primary factory where antibodies against specific antigens (such as the spike protein) are manufactured and perfected. Makers of the mRNA vaccines were pleased to see that antigen-presenting cells (mainly dendritic cells), originally attracted to the site of the injection, take up the mRNA particles and then migrate via the lymph system to the spleen in high numbers and induce high levels of antibody production in these germinal centers [36].
Unfortunately, these same germinal centers are a primary site for the initiation of a process of producing and distributing misfolded prion proteins, often seeded by viral proteins, and triggered by an acute inflammatory response [37].
B cells, also known as B lymphocytes, are a type of immune cell that is the key player in the process that leads to the production of specific antibodies to a foreign antigen [38]. They originate from precursor cells in the bone marrow, and then migrate to the spleen and other lymphoid organs, where they bind to antigens presented to them by antigen-presenting cells, such as the dendritic cells. A maturation process beginning with a multipotent progenitor B cell ends with a mature “memory” B cell that has gone through a complex process to perfect its antibody production process to specifically match the antigen it has been assigned to (e.g., the spike protein). B cells also go through another process called class switching, which changes the type of antibody they produce from one class to another, without changing its specificity to the antigen.
Antibodies are also known as immunoglobulins (Igs), and the possible classes include IgM, IgG, IgA and IgE. IgM is the first immunoglobulin class that is produced (primarily in the spleen), and it is converted into IgG through class switching. IgG is the dominant class in the blood, making up 75% of the serum antibodies, and it is essential for clearing infections in the tissues. Long-lived mature memory B cells cruise the blood stream looking for any appearances of the antigen they have been assigned to, but they are useless for anything else. When the virus they’ve been trained to match mutates to the point where their antibodies no longer match well, they become useless even for the disease they’re trained to fight.
When mice are injected with PrP in the abdomen (intraperitoneal injection), the PrP shows up very quickly in the spleen. From there, the PrP travels along the spinal cord and the vagus nerve to reach the brain, causing prion disease [39]. As we will soon see, α-synuclein, the prion-like protein linked to Parkinson’s disease, also makes its way to the brain from the spleen along the vagus nerve. The mRNA vaccines set up perfect conditions in the spleen for the formation and distribution of conglomerates made up of misfolded α-synuclein, PrP and spike protein.
While α-synuclein causes neurodegenerative disease when it misfolds, in its normal shape it is an active participant in the immune response. α-Synuclein facilitates the processes that lead to antibody production in response to foreign antigens. Dendritic cells express α-synuclein, and it is upregulated (over-expressed) in response to stressors, such as the mRNA, the cationic lipids, and the PEG in the mRNA vaccines. Much can be learned by studying mice that have been genetically engineered to have a defective version of α-synuclein [40]. These mice have a decreased capacity to clear pathogens through phagocytosis, and an impairment in the ability to generate B cells from precursor stem cells. They also had a four-fold reduction in progenitor B cells in the bone marrow. The amount of immunoglobulin G was reduced compared to wildtype, suggesting impaired class switching. Altogether, they are unable to mount an effective immune response to antigens, whether they come from a natural threat or a vaccine.
Dendritic cells under stress accumulate prion proteins and release them into small lipid particles called exosomes, which are then distributed throughout the body, either along nerve fibers or in the general circulation [41]. There is reason to believe that these vaccines will accelerate the release of exosomes containing misfolded prion-like spike proteins that are being produced in large amounts under instruction from the vaccines. These spike proteins will act as seeds to cause α-synuclein and PrP to also misfold and form toxic oligomers together with the spike protein, which are released into the extracellular space as exosomes. These exosomes, released under the severe stress conditions induced by the vaccine, then carry prion proteins into the brain along the vagus nerve, to initiate prion diseases [42].
Impaired Immune Response due to Over-vaccination
A characteristic of the elderly is an impaired ability to mount antibodies against new pathogenic threats, and this is reflected in a failure to generate protective antibodies in response to vaccination. It has been demonstrated in experiments with mice that aged mice have an overabundance of long-lived memory (antigen-experienced) B cells, and this is paired with an inability to generate new B cells from progenitor cells in the bone marrow, as well as impairment in the process of refinement of the antibody response in germinal centers in the spleen and the associated class switching that produces effective IgG antibodies [43, 44]. A significant reduction in the number of naive follicular B cells, combined with an impaired ability to convert them into mature memory B cells leaves these aged mice highly vulnerable to new infections. It is likely that the same principle applies to humans. A plausible conclusion is that aggressive vaccination campaigns accelerate the pace at which an individual’s immune system reaches an ”aged” status due to exuberant generation of memory B cells in response to the artificial stimuli induced by repeated vaccination.
It has now been confirmed that the S1 component of the spike protein shows up in the blood one day after the first mRNA vaccine and remains detectable for up to a month after vaccination, becoming cleared as IgA and IgG antibodies become available [45]. For immune compromised people, it likely stays in the blood much longer, exposing all the tissues — the spleen, the heart, the brain, the gonads, etc. – to the toxic prion-like spike protein.
Today’s children are by far the most vaccinated generation in the history of humankind. If we decide in the near future to deliver a booster COVID-19 shot to them every year, as seems possible given the current climate of enthusiasm for these vaccines, are we inviting disaster for them in years to come? Will their immune system “age” much faster than that of previous generations, due to the exhaustion of the pool of progenitor B cells by all these vaccines? Will they succumb to Parkinson’s disease or other debilitating prion-based neurodegenerative diseases much sooner and in much greater numbers than previous generations? This is an experiment that I hope we finally decide not to carry out.
Summary
There are many reasons to be wary of the COVID-19 vaccines, which have been rushed to market with grossly inadequate evaluation and aggressively promoted to an uninformed public, with the potential for huge, irreversible, negative consequences. One potential consequence is to exhaust the finite supply of progenitor B cells in the bone marrow early in life, causing an inability to mount new antibodies to infectious agents. An even more worrisome possibility is that these vaccines, both the mRNA vaccines and the DNA vector vaccines, may be a pathway to crippling disease sometime in the future. Through the prion-like action of the spike protein, we will likely see an alarming increase in several major neurodegenerative diseases, including Parkinson’s disease, CKD, ALS and Alzheimer’s, and these diseases will show up with increasing prevalence among younger and younger populations, in years to come. Unfortunately, we won’t know whether the vaccines caused this increase, because there will usually be a long time separation between the vaccination event and the disease diagnosis. Very convenient for the vaccine manufacturers, who stand to make huge profits off of our misfortunes — both from the sale of the vaccines themselves and from the large medical cost of treating all these debilitating diseases.
References
[1] MDJ Dicks, AJ Spencer, NJ Edwards et al. A Novel Chimpanzee Adenovirus Vector with Low Human Seroprevalence: Improved Systems for Vector Derivation and Comparative Immunogenicity. PLoS ONE 2012; 7(7): e40385. https://doi.org/10.1371/journal.pone.0040385
[2] J Custers, D Kim, M Leyssen et al. Vaccines Based on Replication Incompetent Ad26 Viral Vectors: Standardized Template with Key Considerations for a Risk/Benefit Assessment. Vaccine 2021; 39(22): 3081-3101. https://www.sciencedirect.com/science/article/pii/S0264410X20311609
[3] N Mukai, SS Kalter, LB Cummins et al. Retinal Tumor Induced in the Baboon by Human Adenovirus 12. Science 1980; 210: 1023-1025. https://doi.org/10.1126/science.7434012.
[4] S. Seneff and G. Nigh. Worse Than the Disease? Reviewing Some Possible Unintended Consequences of the mRNA Vaccines Against COVID-19. International Journal of Vac- cine Theory, Practice, and Research 2021; 2(1): 38-79. https://ijvtpr.com/index.php/IJVTPR/article/view/23
[5] A Greinacher, T Thiele, TE Warkentin, et al. Thrombotic Thrombocytopenia after ChAdOx1 nCov-19 Vaccination. NEJM 2021; April 9, 2021 [Epub ahead of print]. https://doi.org/10.1056/NEJMoa2104840
[6]B Pancevski. Scientists Say They Found Cause of Rare Blood Clotting Linked to AstraZeneca Vaccine. Wall Street Journal. March 19, 2021. https://www.wsj.com/articles/scientists-say-they-found-cause-of-blood-clotting-linked-to-astrazeneca-vaccine-11616169108
[7] E Kowarz, L Krutzke, J Resi, et al. “Vaccine-Induced Covid-19 Mimicry” Syndrome: Splice Reactions within the SARS-CoV-2 Spike Open Reading Frame Result in Spike Protein Variants that May Cause Thromboembolic Events in Patients Immunized with Vector-Based Vaccines. Research Square Preprint. May 26, 2021. https://doi.org/10.21203/rs.3.rs-558954/v1
[8] N Lewis, C Evelegh, and FL Graham. Cloning and sequencing of the cellular-viral junctions from the human adenovirus type 5 transformed 293 cell line. Virology 1997; 233: 423-429. https://doi.org/10.1006/viro.1997.8597
[9] G Shaw, S Morse, M Ararat et al. Preferential Transformation of Human Neuronal Cells by Human Adenoviruses and the Origin of HEK 293 Cells. FASEB J 2002; 16(8): 869-71. https://doi.org/10.1096/fj.01-0995fje.
[10] Y Lei, J Zhang, CR Schiavon et al. SARS-CoV-2 Spike Protein Impairs Endothelial Function via Downregulation of ACE 2 Circulation Research 2021; 128: 1323-1326. https://doi.org/10.1161/CIRCRESAHA.121.31
[11] EM Rhea, AF Logsdon, KM Hansen et al. The S1 Protein of SARS-CoV-2 Crosses the Blood-Brain Barrier in Mice. Nature Neuroscience 2021; 24: 368-378. https://doi.org/10.1038/s41593-020-00771-8
[12] TP Buzhdygana, BJ DeOrec, A Baldwin-Leclairc et al. The SARS-CoV-2 Spike Protein Alters Barrier Function in 2D Static and 3D Microfluidic in-Vitro Models of the Human Blood-Brain Barrier. Neurobiol Dis 2020; 146: 105131. https://doi.org/10.1016/j.nbd.2020.105131.
[13] VS Hernández, MA Zetter, EC Guerra et al. ACE2 expression in rat brain: implications for COVID-19 associated neurological manifestations. bioRxiv preprint May 3, 2021. https://doi.org/10.1101/2021.05.01.442293.
[14] P Brundin, A Nath, and JD Beckham. Is COVID-19 a Perfect Storm for Parkinson’s Disease? Trends in Neurosciences 2020; 43(12): 931-933. https://doi.org/10.1016/j.tins.2020.10.009.
[15] IHCHM Philippens, KP Böszörményi, JA. Wubben et al. SARS-CoV-2 causes brain inflammation and induces Lewy body formation in macaques. bioRxiv preprint. May 5, 2021. https://doi.org/10.1101/2021.02.23.432474.
[16] E Dowd and DP McKernan. Back to the future: lessons from past viral infections and the link with Parkinsons disease. Neuronal Signaling 2021; 5: NS20200051. https://doi.org/10.1042/NS20200051
[17] M Mahic, S Mjaaland, HM Bvelstad, et al. Maternal Immunoreactivity to Herpes Simplex Virus 2 and Risk of Autism Spectrum Disorder in Male Offspring. mSphere 2017; 2(1): e00016-17. https://doi.org/10.1128/mSphere.00016-17.
[18] R Savica, JH Bower, DM Maraganore, eta l. Bell’s Palsy Preceding Parkinson’s Disease: A Case-Control Study. Movement Disorders 2009; 24(10): 1530-3. https://doi.org/10.1002/mds.22616
[19] S Starkstein, S Gellar, M Parlier et al. High Rates of Parkinsonism in Adults with Autism. Journal of Neurodevelopmental Disorders 2015; 7: 29. https://doi.org/10.1186/s11689-015-9125-6
[20] S. Nasralla, DD Rhoads, and BS Appleby. Prion Diseases. In: Hasbun, MD MPH R., Bloch, MD MPH K.C., Bhimraj, MD A. (eds) Neurological Complications of Infectious Diseases. Current Clinical Neurology. Humana, Cham. 2021. https://doi.org/10.1007/978-3-030-56084-3_18
[21] M Glatzel, E Abela, M Maissen and A Aguzzi. Extraneural Pathologic Prion Protein in Sporadic Creutzfeldt-Jakob Disease N Engl J Med 2003; 349: 1812-20. https://doi.org/10.1056/NEJMoa030351
[22] J Marchant. Prion Diseases Hide Out in the Spleen. Nature January 26, 2012: 9904. https://www.doi.org/10.1038/nature.2012.9904
[23] N Daude. Prion Diseases and the Spleen. Viral Immunol 2004; 17(3): 334-49. https://doi.org/10.1089/vim.2004.17.334.
[24] J-K Choi, S-J Park, Y-C Jun et al. Generation of Monoclonal Antibody Recognized by the GXXXG Motif (Glycine Zipper) of Prion Protein. Hybridoma (Larchmt) 2006; 25(5): 271-7. https://doi.org/10.1089/hyb.2006.25.271.
[25] BK Mueller, S Subramaniam, and A. Senes. A Frequent, GxxxG-mediated, Transmembrane Association Motif Is Optimized for the Formation of Interhelical C-H Hydrogen Bonds. Proc Natl Acad Sci USA 2014; 111(10): E888-95. https://doi.org/10.1073/pnas.1319944111
[26] R Broer, B Boson, W Spaan et al. Important Role for the Transmembrane Domain of Severe Acute Respiratory Syndrome Coronavirus Spike Protein during Entry. J Virol 2006; 80(3): 1302-1310. https://doi.org/10.1128/JVI.80.3.1302-1310.2006
[27] Uniprot. Spike Glycoprotein. https://www.uniprot.org/uniprot/P0DTC2.
[28] JB Classen. Review of COVID-19 Vaccines and the Risk of Chronic Adverse Events Including Neurological Degeneration. Journal of Medical-Clinical Research and Reviews 2021; 5(4): 1-7. https://foundationforhealthresearch.org/review-of-covid-19-vaccines-and-the-risk-of-chronic-adverse-events/.
[29] Y Chu and JH Kordower. The Prion Hypothesis of Parkinsons Disease. Current Neurology and Neuroscience Reports v2015; 15: 28. https://doi.org/10.1007/s11910-015-0549-x
[30] MJ Young, M O’Hare, M Matiello et al. Creutzfeldt-Jakob Disease in a Man with COVID-19: SARS-CoV-2-Accelerated Neuro Degeneration? Brain, Behavior, and Immunity 2020; 89: 601-603. https://doi.org/10.1016/j.bbi.2020.07.007
[31] D Idrees and V Kumar. SARS-CoV-2 Spike Protein Interactions with Amyloidogenic Proteins: Potential Clues to Neurodegeneration. Biochem Biophys Res Commun 2021; 554: 94-98. https://doi.org/10.1016/j.bbrc.2021.03.100
[32] TC Yang, K Dayball, Y H Wan, and J Bramson. Detailed Analysis of the CD8+ T-Cell Response following Adenovirus Vaccination. J Virol 2003; 77(24): 13407-13411. https://doi.org/10.1128/JVI.77.24.13407-13411.2003
[33] R Cross. The Tiny Tweak behind COVID-19 Vaccines. Chemical & Engineering News 2020; 98(38). https://cen.acs.org/pharmaceuticals/vaccines/tiny-tweak-behind-COVID-19/98/i38
[34] G Tetz and V Tetz. SARS-CoV-2 Prion-like Domains in Spike Proteins Enable Higher Affinity to ACE2. TBDL Preprint. 2020. https://doi.org/10.20944/preprints202003.0422.v1
[35] G Tetz and V Tetz. Prion-like Domains in Eukaryotic Viruses. Scientific Reports 2018; 8: 8931. https://doi.org/10.1038/s41598-018-27256-w
[36] K Lederer D Castaño, DG Atria et al. SARS-CoV-2 mRNA Vaccines Foster Potent Antigen-Specific Germinal Center Responses Associated with Neutralizing Antibody Generation. Immunity 2020; 53: 1281-1295. https://doi.org/10.1016/j.immuni.2020.11.009
[37] A Aguzzi and M Heikenwalder. Prions, Cytokines, and Chemokines: A Meeting in Lymphoid Organs. Immunity 2005; 22: 145-154. https://doi.org/10.1016/j.immuni.2004.12.007
[38] TW LeBien and TF Tedder. B Lymphocytes: How they Develop and Function. Blood 2008; 112(5): 1570-1580. https://doi.org/10.1182/blood-2008-02-078071.
[39] AJ Raeber, MA Klein, R Frigg et al. PrP-Dependent Association of Prions with Splenic but not Circulating Lymphocytes of ScrapieInfected Mice. EMBO J 1999; 18: 2702-2706. https://doi.org/10.1093/emboj/18.10.2702
[40] W Xiao, A Shameli, CV Harding et al. Late Stages of Hematopoiesis and B Cell Lymphopoiesis are Regulated by α-Synuclein, a Key Player in Parkinson’s Disease. Immunobiology 2014; 219(11): 836-44. https://doi.org/10.1016/j.imbio.2014.07.014
[41] R Castro-Seoane, H Hummerich, T Sweeting et al. Plasmacytoid Dendritic Cells Sequester High Prion Titres at Early Stages of Prion Infection. PLoS Pathogens 2012; 8(2): e1002538. https://doi.org/10.1371/journal.ppat.1002538
[42] NA Mabbott and GG MacPherson. Prions and Their Lethal Journey to the Brain. Nature Reviews Microbiology 2006; 4: 201-211. https://doi.org/10.1038/nrmicro1346
[43] D Frasca, E Van der Put, RL Riley et al. Reduced Ig Class Switch in Aged Mice Correlates with Decreased E47 and Activation-Induced Cytidine Deaminase. J Immunol 2004; 172(4): 2155-2162. https://doi.org/10.4049/jimmunol.172.4.2155
[44] Z Keren, S Naor, S Nussbaum et al. B-Cell Depletion Reactivates B Lymphopoiesis in the BM and Rejuvenates the B Lineage in Aging. Hematopoiesis and Stem Cells 2011; 117(11): 3104-12. https://doi.org/10.1182/blood-2010-09-307983
[45] AF Ogata, C-A Cheng, M Desjardins et al. Circulating SARS-CoV-2 Vaccine Antigen Detected in the Plasma of mRNA-1273 Vaccine Recipients. Clinical Infectious Diseases May 20, 2021 [Epub ahead of print] ciab465d. https://doi.org/10.1093/cid/ciab465.
*
Znanstvenica iz Massachusetts Institute of Technology (MIT), dr. Stephanie Seneff:
Some of the major points of the RAIR exclusive interview:
- Dr. Seneff “anticipates that there will be long-term damage that won’t instantly be linked to the vaccine. Developments, such as an increase in auto-immune and neurodegenerative diseases, which may take 10 to 15 years before manifesting themselves.” “We are in for a big surprise down the road,” she predicts.
- Dr. Seneff believes the vaccine would exacerbate symptoms of those with Parkinson’s.
- Those who claimed that mRNA would not impact DNA are “wrong.”
- Spike protein “really has become the most toxic part of the virus” and exists when Covid is gone.
- “Among the possibilities she foresees is an increase in Creutzfeldt-Jacob disease (CJD), a prion disease (or protein misfolding disease) comparable to mad cow disease.”
- “There is an epidemic of Alzheimer disease, which people are getting at an increasingly younger age. The recklessly and haphazardly implementation of the vaccine roll-out will contribute to this trend.”
*
Dr. Mercila in dr. Stephanie Sennef: https://www.bitchute.com/video/VA2Fv9cwSP7K/?fbclid=IwAR3PwGNra6qi4SQphybl4fV9kpQKfcVDFCk6FpGUIPObh5S9jAAGLBooo0g
*
US COVID-19 Vaccines Proven to Cause More Harm than Good Based on Pivotal Clinical Trial Data Analyzed Using the Proper Scientific Endpoint, “All Cause Severe Morbidity” Classen Immunotherapies, Inc, 3637 Rockdale Road, Manchester, MD J. Bart Classen, MD* Trends in Internal Medicine Research Article Citation: Classen B. US COVID-19 Vaccines Proven to Cause More Harm than Good Based on Pivotal Clinical Trial Data Analyzed Using the Proper Scientific Endpoint, “All Cause Severe Morbidity”. Trends Int Med. 2021; 1(1): 1-6. * Correspondence: J. Bart Classen, MD, Classen Immunotherapies, Inc, 3637 Rockdale Road, Manchester, MD 21102, Tel: 410-377-8526, E-mail: Classen@vaccines.net. Received: 24 July 2021; Accepted: 25 August 2021 ABSTRACT Three COVID-19 vaccines in the US have been released for sale by the FDA under Emergency Use Authorization (EUA) based on a clinical trial design employing a surrogate primary endpoint for health, severe infections with COVID-19. This clinical trial design has been proven dangerously misleading. Many fields of medicine, oncology for example, have abandoned the use of disease specific endpoints for the primary endpoint of pivotal clinical trials (cancer deaths for example) and have adopted “all cause mortality or morbidity” as the proper scientific endpoint of a clinical trial. Pivotal clinical trial data from the 3 marketed COVID-19 vaccines was reanalyzed using “all cause severe morbidity", a scientific measure of health, as the primary endpoint. “All cause severe morbidity” in the treatment group and control group was calculated by adding all severe events reported in the clinical trials. Severe events included both severe infections with COVID-19 and all other severe adverse events in the treatment arm and control arm respectively. This analysis gives reduction in severe COVID-19 infections the same weight as adverse events of equivalent severity. Results prove that none of the vaccines provide a health benefit and all pivotal trials show a statically significant increase in “all cause severe morbidity" in the vaccinated group compared to the placebo group. The Moderna immunized group suffered 3,042 more severe events than the control group (p=0.00001). The Pfizer data was grossly incomplete but data provided showed the vaccination group suffered 90 more severe events than the control group (p=0.000014), when only including “unsolicited” adverse events. The Janssen immunized group suffered 264 more severe events than the control group (p=0.00001). These findings contrast the manufacturers’ inappropriate surrogate endpoints: Janssen claims that their vaccine prevents 6 cases of severe COVD-19 requiring medical attention out of 19,630 immunized; Pfizer claims their vaccine prevents 8 cases of severe COVID-19 out of 21,720 immunized; Moderna claims its vaccine prevents 30 cases of severe COVID-19 out of 15,210 immunized. Based on this data it is all but a certainty that mass COVID-19 immunization is hurting the health of the population in general. Scientific principles dictate that the mass immunization with COVID-19 vaccines must be halted immediately because we face a looming vaccine induced public health catastrophe. Keywords Clinical trial, Vaccines, COVID-19. Introduction For decades, true scientists have warned that pivotal clinical trial designs for vaccines are dangerously flawed and outdated [1]. Vaccines have been promoted and widely utilized under the false claim they have been shown to improve health. However, this claim is only a philosophical argument and not science based. In a true scientific fashion to show a health benefit one would need to show fewer overall deaths during an extended period in the vaccinated group compared to a control group. Less stringent Trends Int Med, 2021 Volume 1 | Issue 1 | 2 of 6 indicators of a health benefit would include fewer severe events of all kinds, fewer days hospitalized for any reason, lower heath care expenses of all types, fewer missed days from work for any health reason. No pivotal clinical trial for a vaccine preventing an infectious disease has ever demonstrated an improvement in health using these scientific measurements of health as a primary endpoint. Instead, vaccine clinical trials have relied on misleading surrogate endpoints of health such as infection rates with a specific infectious agent. Manufactures and government agents have made the scientifically disproved and dangerous philosophical argument that these surrogate endpoints equate to a health benefit. True medical scientists, outside the vaccine fields, have embraced the use of true health measurements as the proven proper scientific endpoint of clinical trials. Decades ago, a pharmaceutical manufacturer would only need to show that a chemotherapeutic agent shrank a tumor or reduce cancer deaths to obtain FDA approval. Manufacturers would market their products under the fraudulent philosophical argument that shrinking tumors or reducing cancer deaths equates to improved survival. However, many of the toxic chemotherapeutic agents would destroy vital organs and actually reduce survival while decreasing cancer deaths at the same time. The FDA and comparable agencies around the world switched to “all cause mortality” as the primary endpoint for pivotal cancer drug trails. The gold standard for marketing approval is to show that those receiving a cancer drug actually live longer than those who do not. Typically, new “miracle” anticancer drugs only prolong survival about 2 months but this added time may be spent severely ill suffering from adverse events caused by the chemotherapy. Application of true scientific principles often severely deflates the hype promoting pharmaceutical products. All previous vaccine trials have suffered not only from lacking a proper primary clinical endpoint put also from insufficient perspective follow up of adverse events. The trials have failed to account for the well-established toxicity data and epidemiology data that vaccines are associated with chronic immune mediated disorders that may not develop for years after immunization. These adverse events, for example type 1 diabetes, are quite common, develop 3 or more years after immunization, and can exceed the reduction in infectious complications induced by the vaccine as was shown with a hemophilus vaccine [1]. Pivotal trials for the recombinant hepatitis B vaccine prospectively recorded adverse events for about 7 days after immunization and newer vaccines typically prospectively follow patients 6 months for adverse events. Use of “all cause morbidity or mortality” as the primary endpoint is warranted in vaccine trials for several reasons. First, the recipients are generally healthy (relative to patients with terminal cancer for example) and the risk of severe morbidity from the target infection is low so even rare adverse events can result in an unfavorable risk benefit. Second, stimulating the immune system with a vaccine can lead to almost any type of adverse event including increasing the incidence or severity of diseases already present in the population. One needs a trial design with a primary endpoint that captures both a decline in infectious complications as well as small rises in hundreds of different immune modified disorders of similar or worse severity as the infectious complications. Three COVID-19 vaccines are approved by the US FDA under Emergency Use Authorization (EUA). These vaccines have been developed by Pfizer-BioNTech, Moderna, and Janssen. Since marketing has begun multiple reports of potential, adverse events have been recorded. These reports include prion disease [2,3] , clotting disorders [4], myocarditis, reproductive issues, death and many more. A clear difference in frequency of adverse events between different COVID-19 vaccines has been published [3]. The clinical trial designs of the pivotal trials and the resulting data was evaluated to determine if scientifically the results support mass immunization with the vaccines for COVID-19. The published data from the manufacturers’ own clinical trials was re analyzed using the proper scientific endpoint “all cause severe morbidity”. Method Data from all three US COVID-19 vaccines was published in the New England Journal of Medicine [4-6]. Data from these three publications and the accompanying published appendixes provided the bulk of the information analyzed. On rare occasions supplemental data was found on the FDA’s website (https://www. fda.gov/advisory-committees/advisory-committee-calendar) in briefing documents pertaining to FDA advisory panel committees for COVID-19 vaccines from Pfizer-BioNTech, Moderna, and Janssen. The scientific primary endpoint, “all severe events", in the treatment group and controls was calculated by adding all severe or life threatening events reported in the clinical trials by the manufacturers. Severe events included both severe cases of COVID-19 and all other severe events in the treatment arm and control arm respectively. A Chi square analysis using a 2x2 table was used to calculate statistical p values. An online statistical chi square calculator (https://www.socscistatistics.com/tests/chisquare) was used. Statistical calculations ignored small differences in total subject number between efficacy and adverse event populations. The randomized number, shown in Table 1, was used as the study population for statistical calculations. In general, the population for adverse events was slightly higher than that for efficacy. Given the statistical significant p, values generated (see Table 1), these small differences do not appear to be material. The FDA document entitled Guidance for Industry Toxicity Grading Scale for Healthy Adult and Adolescent Volunteers Enrolled in Preventive Vaccine Clinical Trials, 2007, provided the following definitions for adverse events. Grades 3, Severe: Prevents daily activity and requires medical intervention. Grades 4, Potentially life threatening: ER visit or hospitalization. Results Moderna The Moderna pivotal Phase III trial results and protocol are published in the New England Journal of Medicine (NEJM) [5].The primary endpoint was COVID-19 illness starting 14 days after the second dose of vaccine however the trial had a secondary endpoint Trends Int Med, 2021 Volume 1 | Issue 1 | 3 of 6 which was patients developing severe COVID-19 symptoms. This later endpoint allowed for a direct comparison to severe adverse events. The study randomized 30,420 individuals, 15,210 were randomized to receive injections with Moderna’s mRNA-1273 vaccine and 15,210 were randomized to receive injections with placebo. Two shots were administered 28 days apart. “Solicited” adverse events were collected 7 days after immunization and “unsolicited” adverse events were reported up to 28 days after administration of each vaccine or approximately 56 days after the first dose according to protocol. Because of dropouts, adverse events were recorded on 15,185 vaccinated patients and 15,166 placebo patients (reference 5, appendix table S8). The treatment group had 11 cases of symptomatic COVID-19 infections and 0 cases severe COVID-19 infections (reference 5, appendix table S13). There were 234 cases of severe “unsolicited” adverse events in the treatment group (reference 5, appendix table S8), and an additional 3,751 “solicited” severe or life threatening (Grade 3 or Grade 4) adverse events (reference 5, appendix table S3 and S4). By contrast, the control group had 185 cases of symptomatic COVID-19 infections and 30 cases of severe COVID-19 infections. However, only one of these case of COVID-19 out of 15,166 controls required admission to an intensive care unit (see reference 5, appendix table S13). There were 202 cases of severe “unsolicited” adverse events in the placebo group and an additional 711 “solicited” severe or life threatening (Grade 3 or Grade 4) adverse events. There were 3 deaths in the placebo group and 2 in the vaccinated group (reference 5, appendix table S8). Pfizer-BioNTech The Pfizer-BioNTech (Pfizer) pivotal Phase III trial results are published in the New England Journal of Medicine [6]. The Pfizer trial was classified as a Phase 1/2/3 trial. Two shots were administered 21 days apart. The primary endpoint was confirmed COVID-19 infections 7 days after the second dose. A post hoc analysis of severe COVID-19 infections was included in the appendix published by the NEJM. The study randomized 43,548 individuals of which 100 did not receive injections, 21,720 received injections with the vaccine and 21,728 received injections with placebo. “Solicited” adverse events were collected 7 days after immunization and “unsolicited” severe adverse events were reported up to 14 weeks after administration of the second dose. However, median safety follow up for “unsolicited” events was only approximately 2 months after the second dose at the time of publication in the NEJM. In the treatment arm there was 1 case of severe Covid-19 (reference 6, appendix table S5), 240 “unsolicited” severe adverse events and 21 “unsolicited” life threatening adverse events (reference 6, appendix table S3). In the placebo arm, there were 9 cases of severe COVID-19, 139 “unsolicited” severe adverse events and 24 “unsolicited” life threatening adverse events. Pfizer used a safety subset of approximately 8,183 (both vaccinated and unvaccinated) to record “solicited” adverse events at 7 days. These data that are not shown in Table 1 in part because the data was depicted graphically in the NEJM manuscript. However, graphical data in the NEJM strongly
indicates the vaccinated group has more “solicited” adverse events of all grade levels than the control group. Janssen The Janssen pivotal Phase III trial design and trial results are published in the New England Journal of Medicine [4]. The primary endpoint was prevention of molecularly confirmed, moderate to severe–critical COVID-19 14 days post vaccination however a secondary endpoint was prevention of molecularly confirmed, severe–critical COVID-19 14 days post vaccination. This later endpoint allowed for a direct comparison to severe adverse events. The study randomized 19,630 to receive a single injection with Janssen’s adenovirus COVID-19 vaccine and randomized 19,691 to receive a single injection with placebo. “Solicited” adverse events were collected 7 days after immunization and “unsolicited” adverse events were reported up to 28 days after administration of the single dose of vaccine. The treatment group had 21 cases of severe or critical COVID-19 infections while the placebo control group had 78 (reference 4, appendix table S9). Further analysis shows that only 2 of 19,514 immunized patients needed medical intervention for COVID-19 infections starting 14 days after immunization, while only 8 of 19,544 controls needed medical intervention for COVID-19 infections starting 14 days after placebo injection where the COVID-19 infection was confirmed by a central lab (reference 4, appendix table S10). There were 83 “unsolicited” and approximately 492 “solicited” serious adverse events in the vaccinated group compared to 96 “unsolicited” and approximately 157 “solicited” serious adverse events in the control group (reference 4, appendix table S7). There were 3 deaths in the treatment group and 16 in the control group (reference 4, appendix table S7). Janssen did not collect “solicited” adverse events from the whole group at day 7 but instead collected these adverse events from a safety group comprising 3,356 vaccinated and 3,380 control patients. FDA briefing document Table 23, page 39 [7] provided the number of “solicited” Grade 3 adverse events in each group. These figures as well as the number of patients randomized were used to extrapolate the number of solicited severe adverse events in the full vaccinated and placebo group as recorded in Table 1. Discussion Scientific analysis of the data from pivotal clinical trials for US COVID-19 vaccines indicates the vaccines fail to show any health benefit and in fact, all the vaccines cause a decline in health in the immunized groups. Health is the sum of all medical events or lack there of. COVID-19 vaccines are promoted as improving health while in fact there is no evidence that these vaccines actual improve health in the individual or population as a whole. The current analysis used the proper scientific endpoint of “all cause severe morbidity”, a true measure of health. By contrast, manufactures and government officials promote the vaccines using a surrogate measure of health, severe infections with COVID-19, and the disproved philosophical argument that this surrogate endpoint equates to health. This substitution of philosophy for science is extremely dangerous and is certainly leading to a catastrophic public health event. Review of data from the three COVID-19 vaccines marketed in the US shows complete lack of a health benefit and even an increase in severe events among vaccine recipients. The proper scientific clinical trial endpoint, “all cause severe morbidity” was created by combing all severe and or life threatening events, both infectious and non-infectious, occurring in the vaccinated and placebo control groups respectively. The data (Table 1) shows there are clearly more severe events in the vaccinated groups. The results are highly statistically significant. The use of a true scientific measure of health as an endpoint for a vaccine trial gives a contrasting result compared to the use of a non-scientific surrogate endpoint of heath, severe infections with COVID-19. Clinical trial data show there were actually few very “severe” cases of COVID-19 in either the vaccinated or the placebo group. Moderna data shows that only one of 15,166 unvaccinated patients required admission to an intensive care unit for COVID-19. Data provided by Janssen shows that only a few of the “severe” COVID-19 infections required medical intervention. Table S10 in the appendix published in the New England Journal of Medicine [4] , shows only 2 of 19,514 patients immunized with the Janssen vaccine needed medical intervention for severe COVID-19 infections starting 14 days after immunization, while only 8 of 19,544 controls needed medical intervention for severe COVID-19 infections starting 14 days after placebo, where the infection was confirmed by a central lab. This benefit, reduction in 6 case of COVID-19 requiring medical intervention, in 19,630 vaccinated patients is simply statistically insignificant in a population that has a hundred fold more severe events of any cause. The Janssen vaccinated group had 595 severe Grade 3 or 4 events in the first 28 days post immunization. Science thus does not support a health benefit with COVID-19 vaccines. All arguments for immunization are purely philosophical and based on false, discredited, assumptions. Reductions in infection rates, hospitalization rates and even death with COVID-19 are poor surrogate markers for health and are not proper primary endpoints for a vaccine clinical trial. As discussed earlier with cancer treatments, a trial endpoint showing reduced cancer deaths is not equivalent to enhanced survival. One could apply enough radiation (or cytotoxic chemotherapy) to cancer patients to kill all their cancer cells and prevent cancer deaths but these cancer patients would die of radiation sickness (or chemotherapy induced organ failure) faster than if they died naturally of cancer. In the same manner, reducing severe COVID-19 infections does not equate to enhanced survival especially when the vaccine can cause clotting, heart disease and many other severe adverse events. Potential vaccine recipients need to know if the vaccine improves their survival in order for them to make an informed consent to be immunized. Unfortunately, the current studies with COVID-19 vaccines in fact show they cause a decline in health. The actual health decline caused by the vaccines is probably much worse than what is depicted in Table 1 for many reasons. First manufactures took a haphazardly approach to recording adverse events in contrast to recording a reduction in COVID-19 events. At Trends Int Med, 2021 Volume 1 | Issue 1 | 5 of 6 the time of publication, patients were only followed prospectively for approximately 7 days after immunization for “solicited” adverse events, and then relied on “unsolicited” reports of adverse events for approximately 30-60 days after immunization. Serious noninfectious events occurring after this 30-60 day period were not part of the published data. By contrast, infections with COVID-19 were followed indefinitely since the time of immunization. Both Janssen and Pfizer were specifically lax recording adverse events and only recorded “solicited” adverse events at day 7 in a safety cohort representing less than 20% of the study population. Given that some of the vaccine clinical trials recruited patients in the third world, patients with low education, and potentially even elderly with dementia the patients can not be expected to understand when they may be having an serious event that needs reporting or how to report it. For these and others reason only 5% of adverse events are generally ever reported [8]. COVID-19 vaccines were released for marketing under a EUA. Use of such a protocol should be reserved for outbreaks of life threatening epidemics. If this were, actually the case with COVID-19 then reduction in “all cause mortality” should be the primary outcome for the vaccine trials and “all cause severe morbidity” should be the secondary endpoint. However, the manufacturers show no evidence of a survival benefit. Deaths in the trials were extremely rare and of 30 deaths, out of roughly 110,000 trial participants, only about 6 deaths were confirmed to have COVID-19 at the time of death. Regrettably, the vaccines did not reduce morbidity but caused an increase in severe events. Worse, the pivotal clinical trials were never designed to show a benefit in “all-cause mortality” or reduction “in all cause severe morbidity”. The fact that the trials were never designed to show these health benefits is an admission that those developing the vaccines never expected the vaccines to result in measurable health benefits. Regrettably some manufacturers have published the false claim [6] that the vaccine have been proven to be “effective” and that its now “unethical” to withhold immunization from the control group. They advocate abolishing the control group by immunizing them. This unscientific act only further proves the pharmaceutical industry is unaccountable to any one and does not feel the need to adhere to principles of science, ethics, or public health. The COVID-19 vaccine pivotal clinical trials were of very short duration and the question exists whether longer-term follow up will reverse the vaccine induced health decline and show a health benefit. The question is purely philosophical. Some manufactures have already threatened to destroy the randomization by immunizing the control group, as stated above, making further scientific study impossible. While it is possible that the vaccines will continue to prevent severe infectious disease long after the immunization, the reality is that immunity wanes with time and vaccine resistant variants keep developing. Another issue is that severe adverse events will continue to occur over time. Given evidence of prion genic activity by both established pathophysiology [2], animal toxicity data [9] and epidemiology data [3] one can expect an increase in adverse events in the vaccinated group for decades. Yearly booster are unlikely to improve the health outcome with COVID-19 vaccines. A booster may provide a small incremental benefit in preventing severe COVID-19 infections however, the boosters are likely to cause many more severe adverse events. Looking at the data on secondary injections with the Moderna vaccine (Table 1) there are approximately 3 times as many Grade 3 or 4 adverse events after the second dose than after the first dose. However, this is not the case following the second dose of placebo in the Moderna placebo group. The net is that adding a booster shot is highly unlikely to induce a favorable health benefit that was missing with the first series of immunization. Government officials are promoting COVID-19 vaccines as a way to stop the epidemic. There is however no scientific data that the COVID-19 vaccines can improve the health of the population. In fact, the data from the clinical trials seems to point in the opposite direction. Given that the population is the sum of the individuals, and the vaccines cause a decline in health in the individuals, then mass immunization is likely to erode the health of the general population, not improve it. Immunization may even cause a selection bias for new variants. Finally, if the COVID-19 outbreak is the result of a bioweapons attack and vaccine resistant variants represent the release of different prototypes then immunization is almost certain to fail [10]. There is an old saying, fool me once shame on you, fool me twice shame on me. This saying can be applied to the COVID-19 mass immunization program. The US anthrax attack of 2001, which originated at US army is Fort Detrick, has demonstrated that there are people in the US government who desire to attack US citizens with bioweapons [10]. According to the chief FBI agent leading the investigation of the US anthrax attack, conspirators were likely not apprehended in part because the investigation was prematurely ended and prior to stopping the investigation, people at the top of the FBI deliberately tried to sabotage the investigation [11]. In the US anthrax attack of 2001, people high in the US government publicly anticipated the anthrax attack as early as 1999 [10]. Similarly with the COVID-19 attack, people high in government anticipated the COVID-19 attack [12,13] several years before the attack took place [10]. There is even data that an effort was made in 2018 to protect certain populations against COVID-19 by immunizing them with MMR vaccine [14]. In such a hostile government environment, the citizens need to individually evaluate the science of immunization with COVID-19 vaccines and not rely on philosophical arguments propagated by government officials. In this case there is no scientific evidence that the COVID-19 vaccines improve the health of the individual, much less of the population as a whole. Mass immunization with COVID-19 vaccines is certainly leading to a catastrophic public health event.
*
Kalifornijska študija (v predtisku) je pokazala, da so cepljeni posamezniki bolj dovzetni za okužbe z različico COVID kot necepljeni. Poleg tega je povečanje pogostosti sevov, odpornejših proti protitelesom, v populaciji povezano s povečanjem pogostosti cepljenja v populaciji.
https://www.medrxiv.org/content/10.1101/2021.08.19.21262139v1.full
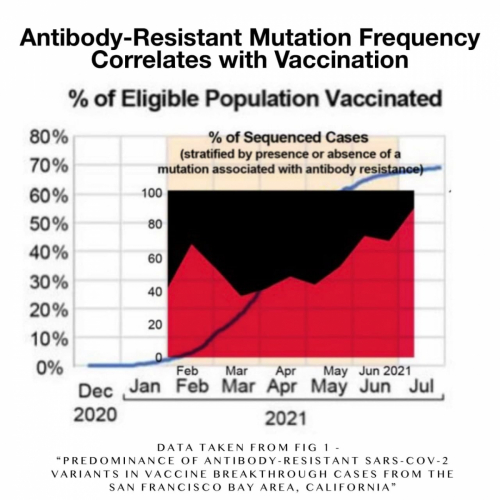
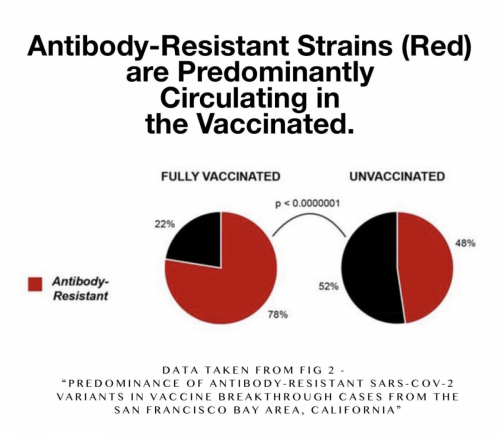
*
Dr. Richard Fleming razlaga, kako mRNA iz cepiv, oziroma beljakovinska bodica, ki ima gene retrovirusa HIV, ki so prion; povzroča bolezen norih krav: 0d 34.00 minute dalje (slovenski podnapisi): Dr Richard Fleming (31.00 minuta- slovenski podnapisi): Virusna mRNA iz cepiva za Covid-19 se vključi v vse, razen v tri človeške kromosome: https://www.facebook.com/odprite.oci.9/videos/565186491206722
*
*
Toksično delovanje beljakovinske bodice: SARS-CoV-2 beljakovinska bodica cilja na os USP33-IRF9 prek eksosomalnega miR-148a in aktivira človeški mikroglija sistem
SARS-CoV-2, nova koronavirusna okužba, je poleg običajnega sindroma dihalne stiske dosledno povezana z nevrološkimi anomalijami pri bolnikih. Disfunkcije več organov, vključno z nevrološkimi posledicami med COVID-19, vztrajajo tudi po zmanjšanju virusne obremenitve. Predlagamo, da je genski produkt SARS-CoV-2, Spike, sposoben spremeniti gostiteljev eksosomalni tovor, ki se prenaša v oddaljena neokužena tkiva in organe ter lahko sproži katastrofalno imunsko kaskado v osrednjem živčevju (CNS). S SARS-CoV-2 beljakovinskimi bodicami transfundirane celice sproščajo precejšnjo količino eksosomov, ki vsebujejo mikroRNA, kot sta miR-148a in miR-590. MikroRNA internalizirajo človeške mikroglije in zavirajo izražanje tarčnega gena USP33 (Ubikvitin specifična peptidaza 33) ter nižje ravni IRF9. Celične ravni USP33 uravnavajo čas obrata IRF9 z deubikvitilacijo. Naši rezultati kažejo tudi, da absorpcija modificiranih eksosomov učinkovito uravnava profil izražanja glavnih pro-vnetnih genov TNFα, NF-κB in IFN-β. Ti rezultati razkrivajo mehanizem poškodb centralnega živčnega sistema, ki jih povzroča SARS-CoV-2 s hiperaktivacijo človeške mikroglije. Naši rezultati poskušajo pojasniti tudi zunajpljučne disfunkcije, opažene v primerih COVID-19, ko aktivna replikacija virusa ni podprta. Ker so bili geni in mRNA za cepivo v veliki meri izbrani za razvoj cepiva, je poznavanje imunskega odziva gostitelja na gene in beljakovine iz cepiv velikega pomena. Naša študija zato zagotavlja nova in pomembna spoznanja o vplivu gena za kodiranje beljakovinskih bodic SARS CoV-2 na prenos gostiteljskih mikroRNA prek eksosomov, ki sprožijo vnetje nevrološkega sistema.
https://www.ncbi.nlm.nih.gov/labs/pmc/articles/PMC8079643/
***
Bodite pozorni na beljakovino spike SARS-CoV-2: Obstaja več, kot je videti na prvi pogled
T.C. Theoharides1,2,3 in P. Conti4
Pandemija COVID-19 je zahtevala hitro proizvodnjo cepiv, namenjenih proizvodnji nevtralizacijskih protiteles proti beljakovinski bodici SARS CoV-2, ki je potrebna za vezavo virusa corona na ciljne celice. Najbolj znana cepiva so uporabljala mRNA ali adenovirusni vektor za usmerjanje človeških celic, da proizvajajo beljakovinske bodice, proti katerim telo večinoma proizvaja nevtralizirajoča protitelesa. Vendar, so nedavna poročila sprožila nekaj skepse glede biološkega delovanja beljakovinskih bodic in vrst proizvedenih protiteles. V enem od člankov so poročali, da nekatera protitelesa v krvi okuženih bolnikov spremenijo obliko beljakovinske bodice, tako da se lažje veže na celice, medtem ko so drugi članki pokazali, da lahko beljakovinska bodica sama po sebi (ne da bi bila del virusa corona, na primer kodirana s cepivi) poškoduje endotelijske celice in poruši krvno-možgansko pregrado. Te ugotovitve so lahko še pomembnejše za patogenezo sindroma dolgega COVID, ki lahko prizadene kar 50 % oseb, okuženih s SARS-CoV-2. V primeru COVID-19 je potreben odziv na oksidativni stres s povečanjem antioksidativnih molekul. V zvezi s tem je znano da so polifenoli naravni antioksidanti s protivnetnimi lastnostmi. Zato obstajajo celo več razlogov za poseganje z uporabo antioksidativnih spojin, kot je luteolin, poleg razpoložljivih cepiv in protivnetnih zdravil, da bi preprečili škodljivo delovanje beljakovinskih bodic.
***
SARS-CoV-2 Spike Glycoprotein S1 povzroča nevrovnetje v mikrogliji BV-2
Poleg respiratornih zapletov, ki jih povzroča SARS-CoV-2, vse več dokazov kaže, da so z boleznijo, ki jo povzroča ta koronavirus, povezani tudi nekateri nevrološki simptomi. V tej študiji smo raziskali učinke stimulacije z beljakovinsko bodico S1 SARS-CoV-2 na nevrovnetje v mikrogliji BV-2. Analize supernatantov kulture so pokazale povečanje proizvodnje TNF-α, IL-6, IL-1β in iNOS/NO. Beljakovinska bodica S1 je povečala tudi ravni beljakovin fosfo-p65 in fosfo-IκBα ter je povečala vezavo DNK in transkripcijsko aktivnost NF-κB. Ti učinki proteina so bili blokirani v prisotnosti BAY11-7082 (1 µM). Izpostavljenost S1 beljakovinskih bodic v mikrogliji BV-2 je povečala tudi raven beljakovin inflammasoma NLRP3 in je povečala aktivnost kaspaze-1. Pri mikrogliji BV-2, stimulirani z beljakovinsko bodico S1 (100 ng/ml), so opazili povečano raven beljakovin p38 MAPK, pri čemer se je to delovanje zmanjšalo v prisotnosti zdravila SKF 86.002 (1 µM). Rezultati imunofluorescenčne mikroskopije so pokazali povečanje izražanja beljakovine TLR4 v mikrogliji BV-2, stimulirani z beljakovinsko bodico S1. Poleg tega sta farmakološka inhibicija s TAK 242 (1 µM) in transfekcija z majhno interferenčno RNK TLR4 povzročili znatno zmanjšanje proizvodnje TNF-α in IL-6 v mikrogliji BV-2, stimulirani z beljakovinsko bodico S1. Ti rezultati so prvi dokaz, ki kaže na nevrovnetje, povzročeno z beljakovinsko bodico S1 v mikrogliji BV-2. Predlagamo, da je indukcija nevrovnetja s to beljakovino v mikrogliji posredovana prek aktivacije NF-κB in p38 MAPK, morda kot posledica aktivacije TLR4. Ti rezultati prispevajo k razumevanju nekaterih mehanizmov, ki so vključeni v patologijo centralnega živčnega sistema pri SARS-CoV-2.
https://link.springer.com/article/10.1007/s12035-021-02593-6
* * *
Podenota S1 beljakovinske bodice SARS-CoV-2 povzroča nevrovnetne, mikroglijske in vedenjske bolezenske odzive: Dokazi o lastnostih, podobnih PAMP (molekularnim vzorcem povezanim s patogeni)
Poudarki
- Podenota S1 beljakovinske bodice SARS-CoV-2 povzroča bolezensko vedenje.
- S1 povzroča subakutni (24 ur) in kronični (7dnevni) nevrovnetni odziv.
- S1 neposredno povzroči proinflamatorni odziv v primarnih mikroglijah.
- S1 aktivira signalizacijo TLR2 in TLR4 in vitro.
- S1 lahko deluje kot molekularni vzorec, povezan s patogeni.
Povzetek
Okužba s SARS-CoV-2 povzroča nevrovnetje ter nevrološke, kognitivne (npr. možganska megla) in nevropsihiatrične simptome (npr. depresija, tesnoba), ki lahko trajajo dlje časa (6 mesecev) po koncu okužbe. Nevroimunski mehanizem(-i), ki povzroča nevrovnetje, povzročeno s SARS-CoV-2, še ni opredeljen(-i). Predlagani mehanizmi vključujejo periferno signalizacijo citokinov v možgane in/ali neposredno virusno okužbo centralnega živčnega sistema. V tem prispevku preučujemo novo hipotezo, da strukturni protein (S1 podenota beljakovinske bodice SARS-CoV-2), deluje kot molekularni vzorec, povezan s patogenom (PAMP), in povzroča nevrovnetne procese neodvisno od virusne okužbe. Predhodni dokazi kažejo, da je podenota S1 beljakovinske bodice SARS-CoV-2 vnetna in vitro in signalizira prek receptorja za prepoznavanje vzorcev TLR4. Zato smo preverili, ali podenota S1 zadostuje za 1) vedenjski odziv bolezni, 2) nevrovnetni odziv, 3) neposredno aktivacijo mikroglije in vitro ter 4) aktivacijo transgenih človeških celic HEK293 s TLR2 in TLR4. Odraslim samcem podgan Sprague-Dawley so vbrizgali intracisterna magna (ICM) z vehiklom ali S1. Spremljanje vedenja v kletki (8 ur po ICM) je pokazalo, da je S1 zmanjšal več vedenjskih vzorcev, vključno s skupno aktivnostjo, samopregledovanjem in vzpenjanjem po steni. S1 je povečal tudi socialno izogibanje pri testu socialnega raziskovanja mladostnikov (24 ur po ICM). S1 je povečal in/ali moduliral izražanje nevroimunskih genov (Iba1, Cd11b, MhcIIα, Cd200r1, Gfap, Tlr2, Tlr4, Nlrp3, Il1b, Hmgb1) in ravni beljakovin (IFNγ, IL-1β, TNF, CXCL1, IL-2, IL-10), ki so se razlikovale po možganskih regijah (hipotalamus, hipokampus in frontalna skorja) in času (24 ur in 7d) po zdravljenju s S1. Neposredna izpostavljenost mikroglije S1 je povzročila povečano izražanje genov (Il1b, Il6, Tnf, Nlrp3) in ravni beljakovin (IL-1β, IL-6, TNF, CXCL1, IL-10). S1 je v transgenih celicah HEK293 aktiviral tudi signalizacijo receptorjev TLR2 in TLR4. Skupaj te ugotovitve kažejo, da lahko strukturni proteini pridobljeni iz SARS-CoV-2, delujejo neodvisno kot PAMP in povzročajo nevrovnetne procese prek vključevanja receptorjev za prepoznavanje vzorcev.
https://www.sciencedirect.com/science/article/pii/S0889159121006383
***
SARS-CoV-2 lahko sproži inflamasom in piroptozo v osrednjem živčevju: mehanicistični pogled na nevrotropizem
Povzetek
Koronavirus 2 hudega akutnega respiratornega sindroma (SARS-CoV-2) lahko vstopi v osrednji živčni sistem in povzroči več nevroloških simptomov. Podatki iz analiz cerebrospinalne tekočine in posmrtnih vzorcev so pokazali, da ima SARS-CoV-2 nevroinvazivne lastnosti. Zato so se tekoče študije osredotočile na mehanizme, ki so vključeni v nevrotropizem in nevronske poškodbe SARS-CoV-2. Inflammasom je del prirojenega imunskega sistema, ki je odgovoren za izločanje in aktivacijo več pro-vnetnih citokinov, kot so interlevkin-1β, interlevkin-6 in interlevkin-18. Ker je znano, da je citokinska nevihta glavni mehanizem, ki mu sledi SARS-CoV-2, lahko inflamasom sproži vnetno obliko programirane celične smrti (piroptoza) po okužbi s SARS-CoV-2 in prispeva k povezanim nevrološkim zapletom. Pregledali in razpravljali smo o možni vlogi inflammasoma in njegovi posledici piroptozi po okužbah s koronavirusi kot možnih mehanizmih nevrotropizma SARS-CoV-2. Nadaljnje študije, zlasti posmrtna analiza vzorcev možganov, pridobljenih od bolnikov s COVID-19, lahko osvetlijo morebitno vlogo inflamasoma pri nevrotropizmu SARS-CoV-2.
https://link.springer.com/article/10.1007/s10787-021-00845-4
** *
Mitohondrijska dinamika v človeški mikrogliji, izpostavljeni beljakovinskim bodicam SARS-COV2 posledice za Neuro-COVID
Povzetek
Po novih kliničnih podatkih iz trenutne pandemije COVID-19 naj bi se pri ~ 40 % bolnikov s COVID-19 razvili nevrološki simptomi, ki jih pripisujemo virusnemu encefalitisu, medtem ko se pri dolgotrajnih bolnikih s COVID kronično nevrovnetje in nevronske poškodbe razvijejo v sindrom, opisan kot nevro-COVID. Predvidevamo, da SAR-COV2 povzroča mitohondrijsko disfunkcijo in aktivacijo mitohondrijsko odvisne intrinzične apoptotične poti, kar povzroči mikroglijsko in nevronsko apoptozo. Cilj naše študije je bil določiti učinek SARS-COV2 na biogenezo mitohondrijev in neinvazivno spremljati apoptozo celic v človeški mikrogliji v realnem času z uporabo Ramanove spektroskopije, ki zagotavlja edinstvene prostorsko-časovne informacije o delovanju mitohondrijev v živih celicah. Človeške mikroglije smo obdelali z beljakovinskimi bodicami SARS-COV2 in preučili ravni citokinov in nastajanje reaktivnih kisikovih zvrsti (ROS), določili vpliv SARS-COV2 na biogenezo mitohondrijev ter preučili spremembe v molekularni sestavi fosfolipidov. Naši rezultati kažejo, da beljakovinska bodica SARS- COV2 poveča raven pro-vnetnih citokinov in proizvodnjo ROS, poveča apoptozo in poveča stopnjo porabe kisika (OCR) v mikroglijskih celicah. Povečanje OCR kaže na povečano proizvodnjo ROS in oksidativni stres, kar kaže na to, da SARS-COV2 povzroča celično smrt. Ramanova spektroskopija je pokazala pomembne razlike v fosfolipidih, kot so fosfatidilinozitol (PI), fosfatidilserin (PS), fosfatidiletanolamin (PE) in fosfatidilholin (PC), ki predstavljajo ~ 80 % lipidov mitohondrijske membrane med mikroglijskimi celicami, zdravljenimi s SARS-COV2, in nezdravljenimi. Ti podatki zagotavljajo pomemben mehanistični vpogled v mitohondrijsko disfunkcijo, ki jo povzroča SARS-COV2 in je podlaga za nevropatologijo, povezano z Neuro-COVID.
https://link.springer.com/article/10.1007/s11481-021-10015-6
*
Mnenje J. Patrick Whelana, zaposlenega pri FDA, dec 2020:
Sem specialist pediater, ki skrbi za otroke z multisistemskim vnetnim sindromom (MIS-C). Skrbi me možnost, da lahko nova cepiva, katerih namen je ustvariti odpornost proti beljakovinski bodici SARS-CoV-2 (vključno s cepivi mRNA podjetij Moderna in Pfizer), povzročijo mikrovaskularne poškodbe možganov, srca, jeter in ledvic na način, za katere trenutno ni videti, da bi bile ocenjene v preskusih varnosti teh potencialnih zdravil.
Puntmann in drugi (JAMA Cardiol. 2020;5:1265-1273) so pokazali, da je prospektivna študija 100 nemških bolnikov, ki so nedavno ozdraveli od COVID-19, pri 78 % od njih v povprečju 2-1/2 meseca po ozdravitvi od akutne bolezni pokazala pomembno prizadetost srca na slikanju z magnetno resonanco srca. Dve tretjini teh bolnikov nista bili nikoli hospitalizirani, pri 60 % pa je bilo vnetje srčne mišice še vedno prisotno. Do nepravilnosti je prišlo neodvisno od predhodnih stanj, resnosti začetne bolezni in splošnega poteka akutne bolezni.
Magro in sod. so pokazali, da pride do poškodb, posredovanih s komplementom, celo v grobo normalni koži s koronavirusom okuženih oseb (Human Pathology 2020:106:106-116). Pokazali so tudi (Magro et al. Annals of Diagnostic Pathology 2021:50 v tisku ), da je izražanje receptorjev ACE-2 največje v mikrovaskularnem delu možganov in podkožnega maščevja, v manjši meri pa v jetrih, ledvicah in srcu. Dokazali so tudi, da se koronavirus razmnožuje skoraj izključno v kapilarnih endotelijskih celicah septalnih kapilar pljuč in nazofarinksa, in da se pri virusni lizi in imunskem uničenju teh celic sproščajo virusni kapsidni proteini (ali psevdo-virusi), ki potujejo po obtoku in se vežejo na receptorje ACE2 v teh drugih delih telesa, kar povzroči aktivacijo komplementarne poti z lektini, ki vežejo manan, kar ne le poškoduje mikrovaskularni endotelij, ampak tudi povzroči nastajanje številnih pro-vnetnih citokinov. Meinhardt in drugi (Nature Neuroscience 2020, v tisku) so pokazali, da je protein spike v možganskih endotelijskih celicah povezan z nastankom mikrotrombov (strdkov), in tako kot Magro in drugi v možganskem endoteliju niso našli virusne RNA. Z drugimi besedami, zdi se, da virusne beljakovine povzročajo poškodbe tkiva, ne da bi se virus aktivno razmnoževal.
Ali je mogoče, da beljakovina spike sama povzroča poškodbe tkiva, povezane s Covid-19? Nuovo in drugi (v tisku) so pokazali, da so v 13/13 možganih bolnikov s smrtnim COVID-19 v endotelih možganskih mikroves prisotni psevdo-virusi (beljakovine bodice, ovojnice in membrane) brez virusne RNA. Poleg tega je vbrizgavanje celotne podenote S1 beljakovinske bodice SARS CoV-2 v repno veno pri miših povzročilo nevrološke znake (povečana žeja, stresno vedenje), ki niso bili vidni pri miših, ki so jim vbrizgali podenoto S2. Podenota S1 se locira v endotelij mikrocevi v mišjih možganih in je močan nevrotoksin. Torej je samo podenota S1 SARS-CoV-2, ki je na konici, sposobna endocitizacije v ACE2 pozitivnih endotelih tako v človeških kot v mišjih možganih, s sočasnim paucikularnim mikroencefalitisom, ki je lahko podlaga za nevrološke zaplete COVID-19. Cepivo Pfizer/BioNTech (BNT162b2) je sestavljeno iz mRNA, ki proizvaja membransko zasidrano beljakovinsko bodico v celi dolžini. Študije na miših kažejo, da lahko takšna neokrnjena oblika beljakovine S1 povzroči mikrovaskularno bolezen v tkivih, ki izražajo veliko receptorja ACE2. Skrajšana oblika S1 je bila pri miših veliko manj škodljiva.
Čeprav je treba še razvozlati nekatere dele te sestavljanke, se zdi, da je beljakovinska bodica, ki je del glavnih cepiv proti SARS-CoV-2, tudi eden od ključnih dejavnikov, ki povzročajo poškodbe oddaljenih organov, ki lahko vključujejo možgane, srce, pljuča in ledvice. Preden bo katero koli od teh cepiv odobreno za široko uporabo pri ljudeh, je treba pri cepljenih osebah oceniti učinke cepljenja na srce (morda z uporabo magnetne resonance srca, kot so to storili Puntmann in drugi). Cepljene bolnike bi lahko testirali tudi na oddaljene poškodbe tkiva v biopsiji kože v deltoidnem predelu, kot so to storili Magro et al. Čeprav je pomembno, da se širjenje virusa hitro zaustavi s cepljenjem prebivalstva, bi bilo veliko slabše, če bi na stotine milijonov ljudi utrpelo dolgotrajne ali celo trajne poškodbe možganskega ali srčnega mikrovaskularja, ker se kratkoročno ni upošteval nenameren učinek cepiv na osnovi beljakovinske bodice polne dolžine na te druge organe.
Posebna previdnost bo potrebna pri morebitnem obsežnem cepljenju otrok, preden bodo na voljo resnični podatki o varnosti ali učinkovitosti teh cepiv v pediatričnih preskušanjih, ki se šele začenjajo.
https://www.regulations.gov/document/FDA-2020-N-1898-0246
***
Interakcije beljakovinske bodice SARS-CoV-2 z amiloidogenimi beljakovinami: Potencialni vzrok za nevrodegeneracijo
Povzetek
Po okužbi s COVID-19 se pojavijo številni nevrološki simptomi, vključno z nevrodegeneracijo. Agregacija proteinov v možganih je lahko eden od pomembnih razlogov za nevrodegeneracijo. Beljakovinska bodica SARS-CoV-2 podenota S1 - receptor binding domain (SARS-CoV-2 S1 RBD) se veže na heparin in beljakovine, ki vežejo heparin. Poleg tega vezava heparina pospešuje agregacijo patoloških amiloidnih beljakovin, ki so prisotne v možganih. V tem članku smo pokazali, da se RBD SARS-CoV-2 S1 veže na številne beljakovine, ki so nagnjene k agregaciji in vežejo heparin, vključno z Aβ, α-sinukleinom, tauonom, prionom in TDP-43 RRM. Te interakcije kažejo, da bi lahko mesto za vezavo heparina na beljakovini S1 pomagalo pri vezavi amiloidnih beljakovin na virusno površino in tako sprožilo agregacijo teh beljakovin, kar nazadnje vodi do nevrodegeneracije v možganih. Rezultati nam bodo pomagali preprečiti prihodnje posledice nevrodegeneracije z usmerjanjem tega procesa vezave in agregacije.
https://pubmed.ncbi.nlm.nih.gov/33789211/
*
Beljakovinska bodica SARS-CoV-2 poslabša popravljanje poškodb DNK in zavira rekombinacijo V(D)J in vitro
Povzetek
Koronavirus 2 hudega akutnega respiratornega sindroma (SARS-CoV-2) je povzročil pandemijo koronavirusne bolezni 2019 (COVID-19), ki je resno prizadela javno zdravje in svetovno gospodarstvo. Adaptivna imunost ima ključno vlogo v boju proti okužbi s SARS-CoV-2 in neposredno vpliva na klinične izide bolnikov. Klinične študije so pokazale, da imajo bolniki s hudo obliko COVID-19 zapoznele in šibke adaptivne imunske odzive; vendar mehanizem, s katerim SARS-CoV-2 ovira adaptivno imunost, ostaja nejasen. Tukaj z uporabo celične linije in vitro poročamo, da beljakovinska bodica SARS-CoV-2 znatno zavira popravljanje poškodb DNK, ki je potrebno za učinkovito rekombinacijo V(D)J pri adaptivni imunosti. Mehanistično smo ugotovili, da se beljakovinska bodica lokalizira v jedru in zavira popravljanje poškodb DNK z oviranjem ključnih beljakovin za popravljanje DNK BRCA1 in 53BP1 pri rekrutiranju na mesto poškodbe. Naše ugotovitve razkrivajo potencialni molekularni mehanizem, s katerim lahko beljakovinska bodica ovira prilagodljivo (adaptivno) imunost, in poudarjajo potencialne stranske učinke cepiv na osnovi polne dolžine beljakovinske bodice SARS CoV-2.
https://www.ncbi.nlm.nih.gov/labs/pmc/articles/PMC8538446/
***
Dr. Bart Classen: Mnogi so trdili, da sta beljakovinska bodica SARS-CoV-2 in njeno zaporedje mRNA, ki ju najdemo v vseh cepivih COVID-19, priongenična. V britanski zbirki podatkov Yellow Card o poročilih o neželenih dogodkih cepiva COVID-19 so bili ocenjeni signali, skladni s pričakovano epidemijo prionske bolezni, povzročene s cepivom COVID. Pogostost neželenih učinkov cepiva družbe AstraZeneca je bila primerjana s pogostostjo neželenih učinkov cepiva COVID družbe Pfizer. Cepiva uporabljajo različne tehnologije, kar omogoča morebitne razlike v stopnjah neželenih učinkov, vendar lahko vsako od njih služi kot kontrolna skupina za drugo cepivo. Analiza je pokazala zelo statistično pomembno in klinično relevantno (2,6-kratno) povečanje Parkinsonove bolezni, prionske bolezni, v poročilih o neželenih učinkih cepiva AstraZeneca v primerjavi s poročili o neželenih učinkih cepiva Pfizer (p = 0,000024). Ti rezultati so skladni s študijami toksičnosti pri opicah, ki kažejo, da okužba s SARS-CoV-2 povzroči nastanek Lewyjevih telesc. Ugotovitve kažejo, da je bila regulativna odobritev cepiv COVID, tudi na podlagi dovoljenja za uporabo v nujnih primerih, prezgodnja in da je treba široko uporabo ustaviti, dokler se ne zaključijo popolne dolgoročne varnostne študije, ki ocenjujejo toksičnost prionov. Za tiste, ki se želijo cepiti proti COVID-19, je treba raziskati alternativna cepiva, kot je cepivo proti ošpicam, mumpsu in rdečkam (MMR).
https://scivisionpub.com/abstract-display.php?id=1746
https://scivisionpub.com/pdfs/covid19-vaccine-associated-parkinsons-disease-a-prion-disease-signal-in-the-uk-yellow-card-adverse-event-database-1746.pdf
*
Znanstvenica iz MIT opozarja, da bi lahko injekcije COVID pri mladih ljudeh povzročile uničujočo nevrodegenerativno bolezen
Dr. Stephanie Seneff, višja znanstvenica v laboratoriju za računalništvo in umetno inteligenco pri MIT, je za Fox News povedala, da lahko cepljenje mladih proti COVID-u povzroči resne nevrodegenerativne bolezni, kot sta Parkinsonova in Alzheimerjeva bolezen.
*
They are extremely dangerous in my opinion, and the technology is novel and untested and has many unknowns. And so in that paper, we looked at theoretically, what could be some consequences that we were anticipating could be happening in the future with these vaccines. And some of them are very slow acting.
[00:04:11] So we listed several things. I’m just itemizing here. We’ve talked about each one of these in different it’s a long paper over 40 pages long. Pathogenic priming multi-system inflammatory disease. Auto-immune disease, allergic reactions anaphylaxis because of the polyethylene glycol, probably. Antibody dependent enhancement, meaning that over time the vaccines could actually backfire and make your disease worse.
[00:04:33] Activation of latent viral infections in the course there’s Bell’s palsy and shingles. These are all viruses that normally stay quiescent. It become alive again after the vaccine. Neurodegeneration and prion disease. The emergence of novel variants. I think the vaccines are driving the emergence of novel variants and the potential for the integration of spike protein gene into human DNA and passing it on to future generations.
[00:04:56] Now, today I want to focus on neurodegenerative and prion diseases. And we have a long section in our paper on that. So I can refer you back to it. For you to read it, if you want to know more. So I want to just show here a picture. This is a nice picture of the messenger RNA in the vaccine.
[00:05:10] These vaccines contain messenger RNA that has the genetic code for the spike protein right here in the middle. And then it’s pegylated with all this polyethylene glycol to keep it away from enzyme, it would break it down. All of the uridines in the entire sequence. There’s four things in the code and one of them is uridine. All of them are replaced with something called one methyl, pseudo uridine and that’s all these guys up here.
[00:05:30] Every single uridine is replaced. That’s extremely unusual, never occurs in nature. It’s incorporated into a lipid particle that looks like a human LDL particle, which means that cells can take it up under natural methods that they already have in place to take up LDL. There’s a synthetic cat ionic liquid, a very unusual untested catatonic lipid.
[00:05:49] That’s added as to act as an adjutant to draw in the immune cells. And that’s been shown to be very toxic to cells. So the RNA is then humanized. It’s got this five prime cap. It’s got this three prime UTR, five-prime UTR, poly ATL. All of these things are human. Making this, mRNA look like human RNA, which gives it a stealth entry.
[00:06:07] The cells are fooled and not aware that this is a viral protein that’s being made. And this gives it a stealth entry system for massive production, spike protein. So I want to give the big picture first and then I’ll have a bunch of slides to support it. And natural infection starts in the nose and the lungs.
[00:06:23] And usually won’t even get into general circulation if you have a healthy, innate immune system, and that’s the most important thing you need to fight this virus, is a healthy innate immune system. The spike protein nanoparticles are ininjected, messenger RNA nano-particless are injected into the deltoid muscle in the arm, bypassing not only the mucosal barriers, but also the vascular barriers.
[00:06:41] So the immune cells come into the arm, take up this message. Also take up these particles and they start making spike protein because they can’t stop themselves from doing it’s all designed to so that it cannot even be controlled to be shut down. And then they carry these spike proteins into the lymph system and they ultimately gathering in the spleen where they continue to make spike protein.
[00:07:00] So these immune cells in the spleen release large quantities of spike protein, and they release them inside exosomes. And these are liquid bodies that cells release when they’re under stress. And so those exosomes contain the spike protein displayed on their surface. And that’s probably what causes tremendous
[00:07:16] reaction antibody response. The vaccines are very successful in their goal of producing a huge antibody response. The kind of response, you would only get in severe disease. People who recover from the disease without many symptoms only produce very small numbers of antibodies. So these exosomes are dispersed throughout the body, but they travel, especially along neuro fibers to the brain and they deliver the prion like spike protein to the neurons, and then an inflammatory response in the brain induces neurological damage.
[00:07:46] So here’s a paper, “Is COVID-19 a perfect storm for Parkinson’s disease”. So this is looking at the disease and this, these authors noted this loss of smell, which is a very common symptom, very interesting and unusual common symptom of this disease, which means that the the virus is capable of going into the nose, going along the olfactory nerve and along the olfactory nerve, it can gain access to the brain stem nuclei.
[00:08:08] It can go along the olfactory nerve. It can travel on the Vegus nerve, which is another nerve system that connects the gut and many of the organs to the brain. And then it gets to the brain and it can update. When it does that. It upregulates a protein called alpha-synuclein, which is one of the proteins.
[00:08:26] It’s a protein that misfolds in association with Parkinson’s disease. That’s well known. And so this alpha-synuclein when there’s too much of it, it folds the wrong way and becomes toxic. And now in the substantia nigra, which is the center of Parkinson’s disease symptoms, dopaminogenic neuron, sorry, that’s a hard word to say.
[00:08:46] The neurons that make dopamine in the substantia nigra, they express high levels of this HT receptor, which allows it to get in. So three independent case reports have described the development of Parkinson’s disease following COVID-19 disease. Now I think the same thing can happen in spades with respect to the vaccine because Parkinson’s disease has been well studied and has been shown that it begins in the gut.
[00:09:07] And it’s from prion proteins that prion-like proteins that are produced by pathogens in the gut. And then the spike protein itself is a prion-like protein. And I’ve studied prions for a long time. And they’re quite interesting because they have a characteristic signature motif, which is this G X, G motif glycine zipper.
[00:09:26] And that motif is present in the human prion protein. There’s 15 of them. Most proteins have zero. Just to be, have a backdrop. Most proteins have zero. The prion protein that humans produce has 15. Amyloid beta, which people probably know is linked to Alzheimer’s disease. Another protein that is false, it has only four.
[00:09:45] The spike protein has six. So it’s worse than amyloid beta in the sense of it’s prion-like character, but not as bad as the human prion protein. So stress immune cells in the digestive tract, in the spleen up regulate alpha-synuclein and they release it packaged up in exosomes, along with this foreign misfolded proteins.
[00:10:02] This is what is known to happen in the association with Parkinson’s disease. And then those exosomes travel along the vagus nerve to the brainstem nuclei and this damages. Then it reaches the substantia nigra damages that organ, and that’s the source of the Parkinson’s disease. And the process over time can take decades, a slow process over decades before symptoms appear.
[00:10:22] This is an amazing paper by some people in India. I recommend everybody read this paper because it’s quite extraordinary. It actually transfected cells with the DNA code to make their own, to make the spike protein. So it’s a similar model to what’s going on with these messenger RNA vaccines.
[00:10:38] They made these cells produce the spike protein, and they determined that these cells then released exosomes. So they verified that cells exposed to the message to make spike protein will produce exosomes loaded with micro RNA. These micro RNA is have, are very strong, controlling signaling molecules that influence policy and particular will cause immune cells to induce an inflammatory response.
[00:11:02] And so they get internalized by these microglia, which are immune cells in the brain. And this induces, this strong inflammatory response, which will lead to brain swelling, brain damage, all these bad things. And so they to quote them these results uncover a bystander pathway of SARS-CoV-2 mediate CNS and central nervous system damage through hyperactivation of human microglia.
[00:11:26] And I just want to have, I just got this picture from this article, which is a nice example of these exosomes. I’m very fascinated by exosomes and I’ve been reading a lot about them lately. The donor cell can be very far away from the recipient cell and the donor would be
[00:11:38] all these nuclei in the brain get exposed to these exosomes that are then taken up by the cells in the brain. And then those micro RNA that are released in them can cause holistic changes in the immune system, in the brain to induce this inflammatory response. So this is a fascinating paper, nucleoside modified messenger, RNA vaccines.
[00:11:59] I’m sorry, the next paper is the one I’m thinking of, but this is interesting too. Induce potent T follicular helper in general center B-cell responses. So this is the paper that’s showing that this nucleoside modification, which is this trick of changing all uridines into methyl pseudo uridines this was something they discovered would really work well to stabilize the RNA. Make it last a long time, and also make it produce a strong response in terms of making protein.
[00:12:26] And that caused a very strong antibody response, which is what they’re looking for. And it induced this formation of germinal centers in the spleen, which is where a lot of the action is taking place in the immune response. And then this other study showed that repeated exposure to foreign protein, to immunization resulted in increased susceptibility to prion protein exposure.
[00:12:45] In other words, they showed that by giving vaccines to people or to animals they became increased more sensitive to the problems with prion proteins that can misfold. And of course, what you’re giving with this vaccine is both at the same time, the expansion of the germinal centers and the delivery of a prion-like protein at the same time.
[00:13:05] So here’s a paper, an article, which is very interesting. J Patrick Wieland and he’s MD-PhD so very highly qualified person. And he asked the question, is it possible the spike protein itself, causes a tissue damage associated with COVID-19? And he talks about a furin cleavage site, which is unique to the spike protein in this, SARS-cov-2 compared to .SARS-cov-1. This a furin cleavage site, which is part of why people think it’s not a natural virus, it allows this S1, the spike protein gets chopped off into S1 and S2 and S1 gets released.
[00:13:38] And so it goes into circulation. It can go anywhere. And in fact, they found that it goes to the vessels, the blood vessels, the small blood vessels in the mouse brain. And that it is a potent neurotoxin. So this is extremely dangerous. So here’s a quote from them. The spike S one sub unit of SARS-CoV-2 alone is capable of being endocytosed by H two positive endothelia.
[00:14:00] These are the cells lining the blood vessels in both the human and the mouse brain with a concomitant Palky cellular micro encephalitis. That may be the basis for the neurological complications. And they’re talking about, of course, the long haul COVID, but I think the vaccines are also causing essentially a long haul COVID microencephalitis meaning the swelling of the brain.
[00:14:18] SARS-COV-2 spike protein interactions with amyloid or genic proteins, potential clues to neuro degeneration. This is another very interesting paper where they found that the receptor binding domain of the spike protein also binds to heparin and to heparin binding proteins. And this is important because it’s been shown in other studies that heparin binding accelerates the aggregation of these amyloid protein.
[00:14:42] So there’s these various proteins that are associated with various neurological diseases, amyloid beta, of course it’s Alzheimer’s alpha-synuclein is Parkinson’s disease. And there’s also Tao, which is linked to Parkinson’s. They have probably on protein itself, which is Crisfield Jaco disease and TDP 43 is linked to ALS.
[00:14:58] So all of these nasty neurodegenerative diseases can be induced by the spike protein going into the brain binding to happen, and then facilitating the misfolding of these other toxic proteins. So this is a paper with a nice diagram over here on the left that shows how foreign pro prion proteins, which I say could be spike coming in a prion protein.
[00:15:20] They act
[00:15:20] like crystals and they induced misfolding of all these susceptible human proteins, such as alpha-synuclein amyloid beta, et cetera. It causes it’s proteins to change their shape from an alpha helix to a beta sheet. And the beta sheet is a soluble formation that then eventually they go home together and they form oligomers and fibrils.
[00:15:38] And then finally they form these plaques that are characteristic features of these diseases. This is a very interesting paper. I would advise you to read this paper because it’s quite shocking and it showed, first of all, that the spike protein actually goes into the nucleus. And this is actually very scary.
[00:15:52] It goes into the nucleus and when it gets into the nucleus, it inhibits specific proteins BRCA1 and 53BP1. These proteins are known to be able to repair DNA damage. So when you prevent the repair of DNA damage and you induce inflammatory response, you’re asking for trouble in terms of getting DNA mutations, which of course are linked to all kinds of diseases.
[00:16:17] When the cells have become disabled because of mutations in their genes. COVID-19 vaccine associated Parkinson’s disease, prion disease, signaling UK CA Yellowcard adverse event database. This is an article by Jay bar class. And I just want to give you a couple of quotes from this article. He has been talking a lot about the concept of prion as a spike as a prion-like protein. All the COVID-19 vaccines on the market, contain spike protein or it’s nucleic acid sequence creating a possible catastrophic epidemic of prion disease in the future.
[00:16:48] And then this analysis should serve as an urgent warning to those mindlessly. Following advice of politicians and public health officials regarding COVID. Now I want to take some time to look through this chart here, I’ve been rummaging through the various database. It’s actually a really great resource.
[00:17:05] And I think we should be using it more people always say it’s not reliable. Anybody can report there’s problems with it. But it’s the best we have. And it’s actually very good, I think, compared to what else we might have available. So you can go to the VARs database online at this website and you can actually just go look and see how many counts there are for various conditions across various co subclasses of the data.
[00:17:30] And so what I did was I looked at a number of different conditions that are associated with neurological disease, memory impairment, amnesia. This is the prion disease, CJD mobility, decreased resistant indicator. Parkinson’s Alzheimer’s Parkinson’s itself, dysphagia, which is difficulty swallowing and Anosomia loss of smell.
[00:17:47] So I just looked at these and I counted how many counts were there in this database? I did this on December 4th of this year. So recently last year, sorry. And and I looked at all the counts for the COVID vaccines for less than a year versus all the counts for all the other vaccines over the history of the database.
[00:18:04] So this is all 31 years, all the vaccines. How many camps? And so you can see just memory impairment significantly more one and a half times more than one and a half times as many reports for memory impairment for these vaccines, compared to all the other vaccines over the history of the database. And then you look at all of these things that I have here have more than one fall, more than more cases of these COVID vaccines and the cases associated with all the other vaccines over the history of the database.
[00:18:32] And in fact, there’s Anosomia is amazing because there’s over 4,000 cases of loss of smell, only 122 for all the other vaccines. It’s a 35 fold ratio between those two. And I want to just note these three. Prion disease. The numbers are small because this disease is very rare and people don’t ever think the prion disease could be caused by the vaccine, but it’s almost seven times as many cases of the prion disease with the COVID vaccines compared to all the other vaccines.
[00:19:02] And then there’s a four and a half times as many Alzheimer’s cases. And then 35 times as many cases of this, which is a very strong indicator of future Parkinson’s disease. And Parkinson’s is over two times as many. So this is anecdotal evidence. It’s actually got an email from someone who pointed this out to me, Mark who’s in France.
[00:19:21] He testified that his wife developed CGG about two weeks after her second dose of the Pfizer vaccine. And he said, we must no longer speak of chance because when you develop a disease where it is said that there is one case in a million, which is true at one person in a million develops this disease in their lifetime and less than 60 cases per year.
[00:19:40] And that you develop the first symptoms 15 days after the second injection of a vaccine that we do not know. We can no longer afford to speak of chance. And I want to just end on a positive note because this is a pretty depressing talk. There’s a paper here shown here published in 2018 and it shows that these really special molecules that are produced by plants and especially by herbs and spices, so things like curcumin, quercetin resveratrol, these are almost like magic molecules.
[00:20:10] And we know that they have a lot of health benefits. Ancient Chinese and ancient Indian herbs have been used, medicinal herbs, have been used for many years. And there’s formulations that have been coming out of mainland China, Taiwan, and India that show tremendous promise in treating a COVID 19 disease or even preventing it.
[00:20:29] And so all of these molecules shown here have been shown to basically drive this process of protein misfolding, which is going usually going this way towards finally these amyloid plaques drive it. Block it from happening and even drive it to reverse. These down here have been shown to convert these beta amyloid fibrils into oligomers.
[00:20:48] So it looks like these would be very therapeutic to help prevent the possibility of ending up with a nasty neurodegenerative disease after you’ve gotten these vaccines, or of course from COVID itself. And I certainly think and Bobby Kennedy said this too. The government needs to be emphasizing our need to maintain a healthy lifestyle, to eat certified organic whole foods and to spice up our food, put lots of herbs and spices into our food, even the vegetables and fruits themselves also have these magic molecules that can really help to keep your immune system strong and also get out in the sunshine and get out in the sunlight without sunscreen, without sunglasses, get your vitamin D up.
[00:21:27] These are such important messages to try to keep us from getting sick from the disease. And even I think from the vaccine as well. I think it’s the same approach to try to protect yourself if you’re forced to get the vaccine, keep yourself extremely healthy through these methods. So in summary, the message RNA vaccines are carefully crafted to induce immune cells to produce large quantities of the SARS-CoV-2 spike protein.
[00:21:49] This protein is neurotoxic and it has prion-like characteristics. Whereas our SARS cov two infection is localized in the lungs. The vaccine induces immune response, primarily in the spleen. Exosomes traveling from the spleen to the brain may play a decisive role. The vaccines produce a very strong antibody response in spleen by activated germinal centers.
[00:22:09] And this increases susceptibility to prion disease. Spike causes an inflammatory response in the brain by activating microglia. And there’s much evidence from VARS of messenger RNA vaccines causing neurodegenerative diseases, including Alzheimer’s Parkinson’s and CJD. Anecdotally CJD can be induced within 15 days of mRNA vaccination. Herbs and spices
[00:22:29] rich in polyphenols may have therapeutic value and thank you for your time.
[00:22:33] Shabnam Palesa Mohamed: Thank you very much, Dr. Stephanie Seneff for that a science-based doctor driven, informative, and of course empowering presentation. I think what you shared with us at the end is equally as important as everything you shared before us.
[00:22:47] And of course we all about knowledge and taking action, with compassion and wisdom. Let’s have a look at some of the questions, Jennifer.
[00:22:54] Dr. Jennifer Hibberd: Yes, we have a number of interesting questions here. Okay. The first question is from Anne McCloskey. “Dr. Seneff in your opinion, are there things those already injected can do and attempt to mitigate these neurological problems?”
[00:23:08] Dr.Stephanie Seneff: Yeah, that’s a big question. Isn’t it? I do have friends who are working on protocols to help people to recover. And I think it actually overlaps tremendously with, in my opinion, just the basic search for good health. Live a lifestyle that’s based on optimizing your health. And to me, that includes really being careful to avoid toxic chemicals eating certified organic food, eating whole foods, staying away from processed foods, getting out in the sunlight.
[00:23:31] These are all the things that I recommend as a general policy. As far as specific things you might take, I would imagine you could take some of these. Like in my last slide I talked about all of these special nutraceuticals that come from plants and from herbs and spices, I think even possibly just taking these Chinese herbs, that there’s a formulation coming out of Taiwan that my husband found, and he’s been taking it as preventative for anticipation of a COVID infection.
[00:23:56] And so I think those kinds of things could be very therapeutic and just the usual thing of zinc and vitamin C and vitamin D and B vitamins are also very important. Just keeping all your vitamins and minerals up and and getting that sunlight exposure for the vitamin D that’s what I would recommend.
[00:24:12] And you could hope that your body, you need to improve your, I should say, also sulfur. I’m always, I’m a big fan of sulfur, as you saw from your introduction, eating a sulfur containing foods and even possibly taking some sulfur containing a nutrients such as methylsulfonylmethane or conjoint with sulfate or N-acetylcysteine.
[00:24:30] These are all sources of sulfur that can help you to boost your self or supply, because I think sulfur is very important for the immune system. You want to have a strong immune system, and I think that’s critical for good health in general, when your immune system becomes weak your general health, but you become very susceptible to these influences from toxic exposures.
[00:24:49] And the really important thing is to make your innate immune system strong.
[00:24:52] Dr. Jennifer Hibberd: Thank you very much. Now, the next question is from Meg. “What is the spike protein burden of the SARS cov two virus versus the vaccine?” In other words, what is the comparison of the risk between the virus and the vaccine for misfitting and inflammation.
[00:25:10] Dr.Stephanie Seneff: So what I believe in of course, we don’t have enough science, we don’t have enough science. Yeah. But what I believe is that if you have a healthy immune system, the virus won’t affect you at all, because you will clear it before it gets past the barrier. So it’s staying in the lungs and not even getting into the circulation.
[00:25:27] The vaccine starts already passed the lungs past the circulation in the muscle. It’s already a huge step towards a place where it can cause trouble. And then the immune cells come in and carry it into the spleen. And from the spleen, that’s when you start to get into really big problems with it traveling,
[00:25:42] so conveniently, along that vagus nerve up to the brainstem. And in fact I’ve been looking at that VARs database reports, and there’s a huge number of reports of headache and migraine headache. Huge numbers. And, I think that’s because of the spike protein has traveled up the vagus nerve to the trigeminal nerve and it’s caused inflammation, trigeminal nerve, which is linked to migraine headaches.
[00:26:04] So I think it’s actually inflaming all the nerves coming out of that pathway. That’s charged with the vagus nerve, goes to the brainstem and then goes to the olfactory nerve. And then the eyes, the optic nerve is getting inflamed. And we were getting all of these evidence. And of course the facial Bell’s palsy, that’s also neurological inflammation in the face.
[00:26:21] I think all of those things are connected to a spike protein infiltrated in the brain. And it will happen with the disease. If you have a really weak immune system, it breaks past the lung barrier breaks past the vascular barrier. And finally it gets to the brain, but that’s a much later step for the disease
[00:26:36] so it’s
[00:26:36] many fewer cases associated with the disease I suspect. And of course you also have all this problems with the heart. I didn’t talk about myocarditis and that’s probably also a Vegas nerve, just traveling to the heart, to the brain from the spleen. And the spike protein response and inflammation in the heart, just like inflammation in the brain.
[00:26:55] It’s the same thing. Really. It’s just different order in the skin, attacked by the spike protein arriving, packaged up inside those exosomes. That’s just something that happens much later in the disease process. And if you’ve got a healthy immune system, you’d never get to that stage.
[00:27:09] That’s encouraging to hear that’s good. Now from Shabnam.
[00:27:13] Dr. Jennifer Hibberd: Our Shabnam here. “Given the reality of self spreading vaccines and shedding, how likely it is that prion disease is transmissible and how can its impact be mitigated?”
[00:27:24] Dr.Stephanie Seneff: Transmissible from a vaccinated person to an unvaccinated person? Is that what she’s saying?
[00:27:29] Dr. Jennifer Hibberd: Yeah, I think it basically the incidence of getting prion disease. I think Shabnam, you’re asking more about the prion disease itself or the spike proteins.
[00:27:41] Shabnam Palesa Mohamed: The prion specific case, because self spreading vaccines are the reality and shedding. There’s emerging evidence on shedding or transmission as well.
[00:27:49] So based on that, how transmissible is prions and how can we mitigate that?
[00:27:53] Dr.Stephanie Seneff: I do think I started hearing about shedding and at first I was very skeptical, but then when I started seeing these exosomes situation, it becomes very easy for shedding to happen because it’s been shown.
[00:28:04] And we talked about that in our paper. Actually, we had quite a large section on the prion diseases in our paper, and we talked about the possibility of the exosomes getting released into the lungs and then out into the air, or even shedding through the skin. So I think it is someone who’s not vaccinated could pick up spike protein and possibly even the code to make spike protein because the messenger RNA itself has been found that the spike protein messager RNA has been found to be able to be completely kept intact and shipped out inside an exome, which is really quite frightening because that means that someone could convey the machinery to make the spike protein, not just the protein itself, but the machinery to make
[00:28:41] it could be conveyed via exosomes that are shed and picked up by somebody else. But I think that the numbers would have to be much smaller. That secondary effect would have to be much smaller. And I doubt that it would get, you would get prion disease from picking up the vaccine secondhand. And I don’t think it would be likely that would end up with a prion disease.
[00:29:00] Dr. Jennifer Hibberd: Okay. Another question from Meg. “Is white matter inflammation at target for recovery? To the drugs, such as ivermectin hydroxychloroquine work through mitigating this?”
[00:29:09] Dr.Stephanie Seneff: Yeah. Now I’m actually not an expert on that. So someone else might know the answer to that. Can ivermectin actually reduce the inflammation in the brain, I think is what you’re asking. Whether it might be a good treatment option for the vaccine. Which I suspect that the same things that treat the disease would treat the vaccine injury.
[00:29:27] I would guess that could be true, but I’m not a doctor. Anybody else want to comment on that?
[00:29:33] Dr. Jennifer Hibberd: We’ve heard cases where people with at that are having seizures that are taking it intermittently that it’s decreased the seizure activity, but I don’t think there’s been anything written up about it.
[00:29:45] Dr. Tess Lawrie: Yeah, I can.
[00:29:46] I can say that Sydney from doctors experiences and feedback, Ivermectin’s one of the, one or top of the list of a bunch of medicines that are being used to help people with post jab injuries and symptoms. And as Dr. Siena says, it actually does tend to the same group of combination therapies that are being used to treat COVID are also being used in the first instance with post jab injuries.
[00:30:12] We really need more research on this, but there’s not going to be time for randomized controlled trials. This is going to be evidence based on doctor’s experiences. Which is probably how it should be.
[00:30:22] Phil Oldfield: I think when it comes to Parkinson’s disease, it’s well known that you’ve got trauma and inflammation that can then trigger the sooner. Courses. And so anything that would mitigate that and I’ve met in does act as an anti-inflammatory. So box to me, targeted to the brain. The other thing of course is that it’s interesting when I saw the figures that there was a symptoms of Parkinsonism on December the fourth and which could be the fact that you’ve got an accelerated build up.
[00:31:04] But, we mustn’t forget that even if a headache and I’ve known people, who’ve had headaches for about three days, really severe headaches, and some that might be milder that in itself could trigger the cascade. And you might find that in about 10, 20 years, that would turn into either Parkinson’s disease or Lewy body dementia.
[00:31:30] And of course, mustn’t forget that that’s been proved for the source code V as well, where that’s been shown and.
[00:31:39] Yeah, I can guarantee that someone’s going to say, oh no, that can’t possibly be the vaccine it’s due to COVID and I want to make it very clear that I don’t know. I think Stephanie made a good point that, when the vaccine is given it’s in the blood, although do, although you do get some back, virus in the blood as well, but I know also the number of people who have been vaccinated, those people who have got COVID and I think we have to be, there’s the lots of papers in JAMA where they be linking, COVID-19 to Parkinson’s disease, very few papers linking the vaccine to Parkinson’s disease.
[00:32:28] And as that’s due to the fact that journals aren’t reluctant published this sort of work, right? Yes. We certainly had that experience. I’d like to introduce everybody to Dr. Phil field, he’s an expert in prion disease and just published a paper with him and Byron bridal and myself on prion disease and vaccines journal.
[00:32:49] And yeah, we had some interesting experiences with BMG rejecting where a paper telling us that it was getting screened by the who or who like to beforehand and then rejected. Can, I can explain it. Basically this, I was really disheartened. We submitted the paper before that buying them had submitted the paper to one of the editors at the BMJ one space sympathetic to our cause.
[00:33:17] And he said, this is just a sort of paper that BMJ needs. And of course, you’ve got a lot of articles from the British medical journal, very balanced. Anyway, we submitted the paper efficiently and we were told that the, any paper from that journal that that is submitted also gets submitted the same time to the WFA Cho to the world health organization.
[00:33:45] But a few weeks after that happened we then off to an email that said, I’m afraid when can’t go any further with this. Now we’re not talking about it being peer review. This is even before it’s been peer reviewed. So we can’t go any further with this. We’ve got so many papers for published that, this one wasn’t interested in it to be significant.
[00:34:10] And so at that point I contacted nature who also, send their articles, that BMJ to the, who I think I actually sent them the article itself. I said, would you be prepared to publish this? Got an answer back the following day saying unfortunately, because of our workload, we’re not accepting unsolicited papers at this present moment in time.
[00:34:37] I was disgusted and eventually we’d got it published in vaccines.
[00:34:43] Dr. Jennifer Hibberd: Yes. And there we gone. I have one last question. And this is actually a good closing question. Why don’t we see more adverse events in the large population, the large proportion of the population who has taken the vaccine.
[00:34:56] Dr.Stephanie Seneff: Why do most of the people…?
[00:34:59] Dr. Jennifer Hibberd: That see a lot as many adverse events…
[00:35:01] Dr.Stephanie Seneff: I think one thing is that people don’t realize the vaccines causing their problems. I actually know speaking personally, people who got the vaccine and then shortly thereafter had something really flare up something else. They were dealing with flared up, and they had to go get treated and aches and pains just much worse than they were before.
[00:35:18] These kinds of anecdotal things that people don’t think the vaccines causing it. I think many times they’re feeling bad after they got the vaccine. Maybe a couple of months later, And they just don’t realize. Cause I think the vaccine basically makes everything else you have, cancer flares up.
[00:35:31] I have friends who treat cancer and they’ve been saying they’re cancer patients that had been in remission are showing up with, new growth of the cancer, these kinds of things. It’s all anecdotal. And I think people only report to VAERS if they feel very confident that the vaccine was the thing that caused their problem for the most part, and so I think that many cases of, and, just, and even something like a headache after the vaccine, it could be very serious and it could lead to serious consequences down the road, but they like, oh yeah, the vaccine causes headaches. That’s fine. That’s part of what’s normal. We’ve been told that we should expect to have some nasty symptoms after the vaccine and that’s normal, but don’t worry.
[00:36:07] That’s shows that the vaccine vaccines working, so people don’t report those things. So I think everything goes way under reported. The numbers are, people are trying to figure out exactly how are under reported. The number that Steve Kirsch has come up with is 41 fold for every report.
[00:36:20] There’s 41 unreported, 40 others that are unreported is a, an estimate based on a number of different ways to look at the.
[00:36:26] Svetlana: Can I just comment on that? This is Svetlana from Ezra [Wellness Clinic]. I think Stephanie, you have such a great point. If people don’t have the the space to report a vaccine injury, we’re not going to be collecting that data.
[00:36:39] So currently, in the mainstream healthcare system, they’re not accepting it. They don’t want to hear Vaccine injury. So if you’re not heard, how can you heal? But for example, at Ezra, we are welcoming vaccine injury, testimonies stories, and injuries, right? So we’re starting to collect our data.
[00:36:54] And that’s right, is that line of work. We do have different facts, reporting systems, just the official ones may have limitations and make it difficult for the doctors to report. But on a number of our alliances, we actually have VAX checker and a few others. So I’m glad to hear that you guys are doing it, too.
[00:37:14] Because I think everybody needs to offer some access for people where they don’t know where to turn, because I know that it hasn’t been made that easy for them. Very much for talking with us, back to Shabnam. Thank you very much, everybody. This has been really interesting.
[00:37:31] Shabnam Palesa Mohamed: Thanks very much, much, Jen.
[00:37:32] I just want to to share that on the SAVAERS system here in South Africa which is independent and alternative. People are reporting memory issues, dementia, amnesia, Alzheimer’s and very frightening comments. Like he turned into a zombie, obviously they mean cognitively. And so I think it is really a wake up for us to understand the science of what’s going on so that together we can find a way to help people who are having these kinds of experiences.
[00:37:57] And that’s why we’re here because the World Council for Health is creating a better way together. Before we, and thank you very much, Dr. Stephanie Seneff. I want to say goodbye to you for now with a quote also from Nelson Mandela, “Everyone can rise above the circumstances and achieve success if they are dedicated to and passionate about what they do.”
[00:38:18] Thank you for your time. Thank you for your service.
[00:38:20] Dr.Stephanie Seneff: Thank you so much for having me. It’s been my pleasure.
Video: https://worldcouncilforhealth.org/multimedia/stephanie-seneff-covid-vaccines-disease/
*
https://newspunch.com/hundreds-of-children-diagnosed-with-childhood-dementia-doctors-baffled/
*
Apr 07, 2021
