
Meta študija maj 2021: Ivermectin lahko konča COVID-19 pandemijo
https://covid19criticalcare.com/wp-content/uploads/2020/11/FLCCC-Ivermectin-in-the-prophylaxis-and-treatment-of-COVID-19.pdf
*
Meta študija o Ivermectinu
*
*
Epidemiološke študije o Ivermectinu
https://covid19criticalcare.com/ivermectin-in-covid-19/
*
Poziv slovenskim inštitucijam k uporabi Ivermectina in hidroksiklorokina
https://docs.google.com/document/d/1lzBrowniPxz6oM8IRfIogh-_FHaVayqT/edit
*
Pričevanje dr. Pierre Korya o učinkovitosti Ivermectina in korupciji v Svetovni zdravstveni organizaciji: https://www.bitchute.com/video/j5X8oRUYbyHu/
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8088823/pdf/ajt-28-e299.pdf
*
Slovaška je dovolila uporabo Ivermectina za zdravljenje COVID-19 in kot preventivno zdravilo
https://trialsitenews.com/slovakia-becomes-the-first-eu-nation-to-formally-approve-ivermectin-for-both-prophylaxis-and-treatment-for-covid-19-patients/?fbclid=IwAR1gR_hi6QUWqugZVacJKx95Ci7SGDma4rS1qJCpcrAQUO3Xrnq-uU8bOL4
* * *
Češko Ministarstvo zdravstva službeno odobrilo privremenu uporabu ivermektina zbog COVID-19 krize
https://dokumentarac.hr/covid-19/cesko-ministarstvo-zdravstva-sluzbeno-odobrilo-privremenu-uporabu-ivermektina-zbog-covid-19-krize/
*
Južna Afrika je odobrila Ivermectin: strokovno preverjena študija pravi, da lahko konča COVID-19
https://coronanews123.wordpress.com/2021/05/10/south-africa-approves-ivermectin-peer-reviewed-study-says-can-end-covid/
*
*
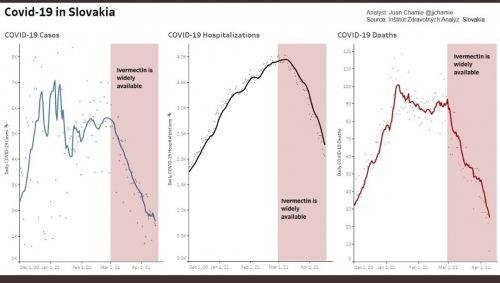
Po začetku cepljenja 16.2. 2021 se je število pozitivnih primerov PCR testa znižalo, nato pa je naraslo bolj kot pred cepljenjem. Po uvedbi Ivermectina 8.3. 2021 pa je število pozitivnih PCR testov dramatično padlo
*
https://www.delo.si/sobotna-priloga/prepovedano-zdravilo/
Cepljenje za trajno obvladovanje epidemije ne bo zadoščalo. Človeštvo potrebuje tudi zdravilo. Poročila izvedencev Svetovne zdravstvene organizacije zanikajo, da bi imela zdravila, od katerih smo največ pričakovali v lanskem letu, pozitivne učinke. Hkrati pa je v javnosti vedno več analiz, ki dokazujejo pozitivne učinke zdravila ivermektin. Dr. Matjaž Zwitter
*
https://c19ivermectin.com/ Analiza 85 študij
*
* * *
Pismo indijskih odvetnikov WHO glede Ivermectina:
*
Poleg škodljivih stranskih učinkov je učinkovitost cepiv proti COVID-19 zelo vprašljiva, saj naj bi na primer Moderna cepivo dajalo imunost le tri mesece, kar je smešno kratek čas. Cepiva niso potrebna, ker imamo na voljo učinkovita zdravila. Pisali smo že o hidroksi klorokinu s katerim z velikim uspehom zdravi vodilni svetovni virolog prof. Raoult Didier iz Francije, poročajo pa tudi o drugih uspešnih terapijah, kot je intravenozni C vitamin ali vitamin D.
*
Drugo uspešno zdravilo je Ivermectin, o katerem je pred ameriškim Senatom dne 8. 12. 2020 pričal zdravnik dr. Pierre Kory. Povedal je, da je njegova skupina odkrila, da je Ivermectin učinkovit pri zdravljenju COVID-19 in pozval je institucije, da ga začnejo uporabljati.
Dr. Pierre Kory je bil izredni profesor in predstojnik Centra za intenzivno nego in direktor Centra za travmatologijo in intenzivno nego na Univerzi Wisconsin, pred kratkim pa se je pridružil urgentni enoti pri Medicinskem centru Aurora St. Luke v Milwaukee-ju. Je specialist urgetne in interne medicine in pulmolog. Pomagal je pri zdravljenju številnih COVID-19 bolnikov v več ameriških zveznih državah. Je tudi predsednik Zveze za intenzivno zdravljenje COVID-19 bolnikov, ki je neprofitna zveza zdravnikov intenzivne nege, ki jo vodi dr. Paul Merrick. Njihova misija v zadnjih devetih mesecih je bila razvoj učinkovitih protokolov za zdravljenje COVID-19 z uporabo obstoječih zdravil. Maja 2020 je bil dr. Kory poklican na zaslišanje pred Senatom, ker je razvijal protokol s protivnetnimi steroidi za intenzivno zdravljenje COVID-19. Mnogi zdravniki so bili hvaležni za to, ker je to izboljšalo njihovn način zdravljenja. Tu je nekaj odlomkov gorova dr. Kory na zaslišanju pred Senatom dne 8.12. 2020:
Dr. Kory: Govorim v imenu skupine, v kateri so priznani znanstveniki na področju medicine Imamo okoli 2000 recenziranih znanstvenih del in zbrali smo se na začetku pandemije, da bi pregledali vso svetovno literaturo o vseh aspektih te bolezni, zato da bi razvili učinkovit protokol zdravljenja COVID-19. Maja sem povedal, da je ključno uporabiti protivnetne kortikosteroide, v času ko so mednarodne organizacije prepovedale njihovo uporabo. Pokazalo se je, da smo imeli prav in smo s tem rešili nešteta življenja. Danes imamo novo priporočilo. Naša skupina je pregledala vso dostopno literaturo v zadnjih devetih mesecih. Zaskrbljeni smo, ker Nacionalni institut za zdravje (NIH), Center za nadzor bolezni (CDC) in Uprava za hrano in zdravila (FDA) niso ustanovili operativne skupine za oceno učinkovitosti uporabe obstoječih zdravil za zdravljenje COVID-19.
Vse se vrti okoli novih in dragih zdravil, kot so Tocilizumab, Remdesivir, monoklonskih protiteles in cepiva. Naša strokovna skupina je izpolnila to praznino in našli smo rešitev za to krizo. To je čudežno učinkovito zdravilo Ivermectin, kar smo ugotovili na osnovi znanstvenih raziskav. Zakaj ga Nacionalni institut ne priporoča izven nadziranih kliničnih raziskav? To je bilo v avgustu 2020 in od takrat so se pojavile nove znanstvene raziskave in podatki iz vsega sveta, ki kažejo na čudežno delovanje Ivermectina, ki preprečuje prenos koronavirusa SARS CoV-2 in preprečuje razvoj bolezni COVID-19:
1. Imamo dokaze, da je Ivermectin učinkovit kot preventivno zdravilo – kdor ga vzame, ne bo zbolel za COVID-19. Včeraj smo dobili raziskavo iz Argentine, ki jo je opravil vodilni raziskovalec Ivermectina dr. Hector Carvallos. Dali so Ivermectin preventivno 800 zdravstvenim delavcem in nihče ni zbolel za COVID-19. Med 400 ljudmi, ki ga niso vzeli, jih je zbolelo 58%, to je 237 ljudi. Ivermectin je zelo močna protivirusna snov. Trenutno potekajo štiri raziskave o preventivnem delovanju Ivermectina na 1500 ljudeh in vse kažejo veliko učinkovitost.
2. Imamo tri raziskave o uporabi Ivermectina v zgodnji fazi zdravljenja na ambulantnem nivoju in veliko podatkov, ki kažejo, da to zdravilo zmanjšuje stopnjo hospitalizacije in smrti zaradi COVID-19.
3. Imamo tudi 4 raziskave na pacientih v bolnišnicah, ki kažejo, da Ivermectin znižuje smrtnost zaradi COVID-19.
Leta 2015 je bila podeljena Nobelova nagrada za dokaz učinkovitosti Ivermectina pri zmanjšanju parazitskih boleznih in vpliva na javno zdravje. Deluje pa tudi protivirusno in protivnetno. Uporaba Ivermectina je ključna za zajezitev pandemije COVID-19 in zmanjšanje smrti zaradi te bolezni. Vsak dan sem gledal bolnike, ki so umirali na intenzivni negi priključeni na ventilatorje. Zdravniki smo dobili travme zaradi tega. Zato kličemo k akciji in uporabi Ivermectina, kot sredstva za preprečevanje bolezni in smrti zaradi COVID-19. Pozivamo Nacionalni institut za zdravje, da ponovno oceni odločitev iz avgusta 2020 in priporoči Ivermectin, o katerem imamo že 30 študij, ki verodostojno pričajo o njegovi učinkovitosti. Mi smo zelo kredibilna skupina zdravnikov in znanstvenikov na področju medicine. Nismo naključna skupina zdravnikov, ki trdijo da imajo zdravilo. Prosimo pa za pregled in oceno naših podatkov, ki kažejo, da je Ivermectin potrebno uporabiti TAKOJ. V ZDA zaradi COVID-19 najbolj umirajo starejši, temnopolti in latino revni prebivalci. Ivermectiin pa je tako učinkovit in varen, zato prosim Nacionalni institut za zdravje, da ponovno oceni naše podatke.
Vir: https://www.youtube.com/watch?v=Tq8SXOBy-4w&feature=youtu.be&fbclid=IwAR3q-J06FRefi88DmKKB2VAiooCrZ6-WctoPdS-rxjAWs-9DWvG-8d9RC5g
*
Revija ISIS - medicina str. 39: članek o Ivermectinu:
http://online.pubhtml5.com/agha/lkug/#p=39
*
*
https://trialsitenews.com/another-new-york-state-supreme-court-justice-ivermectin-order-helping-81-year-old-farmer/?fbclid=IwAR2q48IhraqTcrqf7pdYgCwwf4fcnZFbci_Z0XHFh39Ad48_2sodmHVR7uY
*
V raziskavah narejenih v tretjem svetu so odkrili, da Ivermektin pomaga hitreje preboleti covid-19, kar je dober znak pred razširitvijo raziskav, rezultati katerih naj bi bili znani že konec januarja.
Zdravilo, ki se uporablja za zdravljenje uši in proti zajedavcem, bi lahko zmanjšalo tveganje za smrt hospitaliziranih bolnikov s Covidom do 80 odstotkov, kaže študija.
Ugotovljeno je bilo tudi, da zdravilo Ivermektin, zdravilo na recept, ki lahko stane le približno 2 dolarja, praktično prepolovi čas zdravljenja.
Andrew Hill, virolog z univerze v Liverpoolu, je s strani Svetovne zdravstvene organizacije skrbel za nadzor analize zdravila. Trdi, da je zdravilo lahko “transformacijsko” v boju proti virusu.
Študije v Egiptu in Bangladešu pokazale izjemne rezultate
V tem testu zdravila so bolniki naključno dobivali placebo ali Ivermektin. Skupina je preučila 11 testov z več kot 1.000 bolniki, preskušanja pa so bila v glavnem izvedena v državah v razvoju.
Bolniki, vključeni v teste, so se Covid-19 rešili v polovici običajnega časa, ki pri večini ljudi traja dva tedna. Od 573 bolnikov, ki so jemali zdravilo Ivermektin, jih je umrlo osem, medtem ko jih je pri 510, ki so jemali placebo umrlo 44.
Študije so bile izvedene predvsem v državah v razvoju – vključno z Bangladešem, Argentino in Egiptom – raziskavo pa je naročila Svetovna zdravstvena organizacija. Bolniki so prejemali odmerke Ivermektina med 0,2 in 0,6 mg / kg, v eni študiji pa kar 12 mg.
V poskusu v Egiptu je 100 bolnikov z blagimi simptomi v povprečju v petih dneh ni bilo več kužnih, ko so dobili zdravilo. Za primerjavo, številka tistih, ki niso prejeli zdravila je bila približno 10 dni. Pri 100 bolnikih, ki so se borili s hudimi simptomi, je zdravilo Covid odstranilo v povprečju v šestih dneh, po tem, ko so dobili zdravilo, v primerjavi z 12 dnevi pri tistih brez zdravila.
Podobni rezultati so bili vidni tudi v študiji, izvedeni v Bangladešu. Preskusi, v katerih bo sodelovalo nadaljnjih 7100 udeležencev, bodo predvidoma objavljeni v prihodnjih mesecih, konec januarja pa naj bi bili objavljeni še trije.
Smrtni primeri zmanjšani za 80 %
Zgodnje analize kažejo, da lahko zdravilo pomaga bolnikom, ki trpijo za virusom, vendar znanstveniki teh sklepov še niso opozorili.
Študije so primerjale z različnimi odmerki Ivermektina, časovnimi obdobji in različnimi načini zdravljenja s svojimi kontrolnimi skupinami.
Raziskava je tako ugotovila, da je zdravilo zmanjšala število smrtnih primerov za ljudi, ki so bili sprejeti v bolnišnico, za 80 odstotkov. Analiza iz preskusov naj bi bila objavljena konec tega meseca, dr. Hill pa je dejal, da bi lahko bil Ivermektin pomembno orodje za preprečevanje bolezni Covid-19 v državah v razvoju.
Dejal je, da bi lahko bile ugotovitve iz raziskave ključne, saj se številne države spopadajo z drugim valom, to zdravilo pa bi poleg učinkovitosti prineslo tudi cenovno dostopnost. »Združeni podatki so lahko dovolj veliki, da lahko prinesejo priporočilo Svetovne zdravstvene organizacije za zdravljenje s tem zdravilom po vsem svetu. Če bomo te iste trende dosledno opazili v naslednjih študijah, bo to resnično zdravljenje, ki bo vse spremenilo,« je dodal.
Raziskovalci menijo, da to poceni zdravilo proti ušem deluje tako, da posega v življenjski cikel koronavirusa. Delovalo naj bi tako, da ohromi virus SARS-CoV-2 in “premaga njegov živčni sistem”, da prepreči njegovo razmnoževanje.
*
https://www.youtube.com/watch?v=6Thfq47Hfvs
*
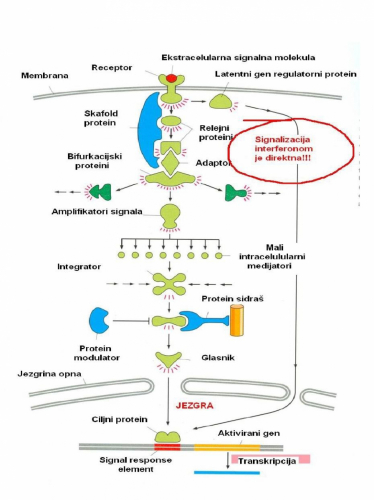
Napovedal sem, da bom povedal nekaj o Ivermektinu (Driponin), skritem zdravilu proti ′′ novi′′ Covid 19 in drugim ′′ starim-normalnim ", pravzaprav ′′ gripi podobnim ′′ boleznim, ki jih povzročajo ′′ drugi virusu influence podobni respiratorni virusi. Posamezno lahko te bolezni ostanejo brez simptomov, so kot prehlad in imajo lahko smrtno žrtev. Vse je odvisno od tega kdo je zbolel. Sem počakal z objavo, ker sem se moral prepričati.Prijatelj, star petdeset let, je preboleval hudo bolezen, pa je šlo na slabše. Vztrajne visoke temperature, vse težje in krajše dihanje. Poskusil z deksametazonom, sumamedom, aspirinom in na koncu ′′ domačim ′′ kisikom pod zdravniškim nadzorom. Prišlo je do izboljšav, a začel je razmišljati o koncu. Nismo ga mogli prepričati v protokola (za polnjenje statistike) WHO ali za sprejem v bolnišnico. Privolil je v ivermektin, saj ga je priporočil dr. Kory, predsednik Zavezništva za intenzivno obravnavo bolnikov s Covid-19, ki je preizkušal na bolnikih delovanje REGISTRIRANIH, NE nujno protiglivičnih pripravkov z ekipo zdravnikov. .... (glejte : https://www.bitchute.com/video/J41li0kEbn9m/ )Že dan po tem, ko je začel jemati zdravilo, mu je temperatura padla, nekaj dni kasneje pa je bilo jasno, da je bolezen za njim. Ivermektin ni registriran na Hrvaškem, se ga pa dobi od zunaj preko zasebnega recepta. ′′ Govorice ′′ o njegovi učinkovitosti so imele nasprotno delovanje- lekarne so več kot podvojile maržo, z receptom pa so zahtevali še zgodovino parazitske bolezni. Hrvaška, tako kot južnoameriške države, je otežila pridobitev zdravila!!Ivermektin deluje tako, da prepreči delovanje ionskih klorovih kanalov, ki se nahajajo na parazitnih membranah (ne gostitelja) Zaradi blokade parazitske celice ne morejo ustvariti in vzdrževati t.i. membranski potencial potreben za njihovo življenje! Ko umirajo celice, umrejo tudi paraziti. Z aktivnim sproščanjem negativnih ionov pride do negativnega ovoja okoli celic, ki jim ne omogoča dotikanja, tudi v najdebelejših tkivih. Med njimi so medcelični prostori za lažji transport plinov, potrebnih za celično dihanje (! ), dostavo hranil in odvoz odpadkov.Kaj pa ima blokada ionskih kanalov parazitskih celic s protivirusnim in protivnetnim delovanjem pri človeku? Ob pregledu literature sem ′′ obtičal ′′ z nepomembno podrobnostjo, kako Ivermektin POVEČA SPLOŠNO PROPUSTNOST KARIOMEMBRAN, torej propustnost membran, ki delijo jedro celice od citoplazme. Kako lahko povečanje propustnosti kariomebran ustavi množenje virusov, glede na to, da se virus ne množi v jedru, ampak v citoplazmi!? Takole.Slika prikazuje, kako signali iz okolja (rdeča pika) sporočajo celici, natančneje njenemu jedru, natančneje nukleinskim kislinam v jedru, najbolj natančno: delom nukleinskih kislin oziroma genom, kaj storiti in kateri geni naj se aktivirajo? Ko prejmejo USTREZEN signal, se bodo USTREZNI geni ′′ odzvali ′′ s produkcijo in pošiljanjem USTREZNIH sporočilnih - mRNK (preko kariomebrane) v citoplazmo, kjer bodo zapisi prevedeni v beljakovinski jezik. V primeru interferonskih signalov se bodo celice odzvale s proizvodnjo protirusnih beljakovin. V prvi vrsti s proteini neimunološke protivirusne (pra) obrambe, tiste obrambe, ki pri okuženih s SARS CoV-2 (Covid-19), povzročijo asimptomatsko prebolevanje!Za razliko od običajne signalizacije , ki sje pod nadzorom in kontrolo (glejte sliko! ), interferonski signali (ali signali! za nevrnost) potujejo BREZ PREVERJANJA direktno v jedro. Ker NI časa! Interferon-receptorski kompleks je trenutno internaliziran in potuje (prek kariomembrane) v jedro, kjer se vtisne v foasphodiestersko ogrinjalo nukleinskega zaporedja, kar aktivira t. i. interferonske gene, ki jih je znanih do sedaj že več kot 300. Interferonski geni prepišejo informacije v interferonske sporočilne -mRNK, ki gredo v citoplazmo, kjer začnejo množično proizvodnjo različnih ′′ interferonskih ′′ proteinov, katerih učinke Big Farma ne bo nikoli dosegla ali celo presegla!Domnevam, da je ključni trenutek akcije Ivermektina, ki poveča propustnost kariomembrane, da olajša vstop interferona v jedro celice?! Interferoni niso ravno majhni!Skoraj trenuten in učinkovit proti virusni odziv okuženih celic, lahko interpretiramo le z aktiviranjem celičnih obramb, olajšanim prehodom interferonskih signalov v jedro.Skrbno preučevanje potenciala membrane, ko sem bil študent, zgleda ni bilo naključje. Zagotovo je vplivalo na moje življenjsko potovanje. Tisti lucidni, ki pravijo: ′′ prhotanje ptičjih kril na Aljaski, lahko povzroči nevihto na Kanarskih otokih", imajo prav. Za zainteresirane, biografski del v naslednji objavi. Naročil bi vsem. Če vam je do ′′ najdražji h", jih ne dajajte na respiratorje! Najprej poskusite Ivermektin.
Zakaj? Dve nedavni študiji, ena britanska, druga izraelska, ugotavljata, da smrtnost s COVID-om V BOLNIŠNICAH RASTE Z ZASEDENOSTJO LE-TEH, ceteris paribus
Na osnovi dosedanjih ugotovitev, Ivermectin, če je vzet pravočasno in pravilno, zmanjšuje okuženost do 90% (pri novem sevu bo tu verjetno odstotek manjši, ni pa rečeno). Ker je manj okuženih, je tudi manj hospitalizacij. Ocene so, da bi s protokolom »outpatient treatment« od FLCCC ALLIANCE, lahko zmanjšali število hospitalizacij za 8 x, TRAJANJE hospitalizacij pa prepolovili! In ker bi bilo manj hospitaliziranih, bi bilo tudi manj mrtvih. Če k temu dodamo, da na osnovi dosedanjih študij IVM zmanjšuje smrtnost za okoli 83%, bi bilo, če bi k temu dodali še nižjo hospitalizacijo, do 16 x manj mrtvih.
S tem novim sevom, ki je bolj infektiven, bi bile verjetno vse te številke nižje. Po drugi strani pa je IVM, ker ima drug princip delovanja, imun na mutacije virusa, kar pa ne moremo reči za cepiva …
Cepiva tudi niso zdravilo, Ivermectin je. Ivermectin tu vidim kot most do cepiva, kot njegov »back-up«, kot cepivo revnih in tistih, ki so skeptični do teh.
https://covid19criticalcare.com/about/the-flccc-physicians/
FLCCC Protokol zdravljenja COVID-19: https://covid19criticalcare.com/wp-content/uploads/2020/11/FLCCC_Alliance-I-MASKplus-Protocol-v8-2021-01-12-ENGLISH.pdf
PROPHYLAXIS PROTOCOL lvermectin Prophylaxis for high risk individuals 0.2 mg/kg per dose* — one dose today, 2nd dose in 48 hours, then one dose every 2 weeks** Post COVID-19 exposure prophylaxis*** 0.2 mg/kg per dose*— one dose today, 2nd dose in 48 hours** Vitamin D3 1,000–3,000 IU/day Vitamin C 1,000mg twice a day Quercetin 250mg/day Zinc 50mg/day Melatonin 6mg before bedtime (causes drowsiness)
EARLY OUTPATIENT PROTOCOL**** lvermectin 0.2 mg/kg per dose* — one dose daily, minimum of 2 days, continue daily until recovered (max 5 days)** Vitamin D3 4,000 IU/day Vitamin C 2,000 mg 2–3 times daily Quercetin 250mg twice a day Zinc 100mg/day Melatonin 10mg before bedtime (causes drowsiness) Aspirin 325mg/day (unless contraindicated) Pulse Oximeter Monitoring of oxygen saturation is recommended (for instructions please see page 2 of this file) * ≈ 0.09 mg/lb per dose — please see conversion table on page 2 to calculate the appropriate ivermectin dose (take it with or after meals). ** The dosing may be updated as further scientific studies emerge. *** To use if a household member is COVID-19 positive, or you have prolonged exposure to a COVID-19 positive patient without wearing a mask **** For late phase — hospitalized patients — see the FLCCC’s MATH+ Hospital Treatment Protocol for COVID-19 on www.flccc.net
https://swprs.org/on-the-treatment-of-covid-19/
*
Protokol zdravljenja https://www.evms.edu/media/evms_public/departments/internal_medicine/EVMS_Critical_Care_COVID-19_Protocol.pdf
https://www.evms.edu/covid-19/covid_care_for_clinicians/
*
"Vlada je v cepiva vložila 18,5 milijarde USD. A njihova naložba v zdravila je bila veliko manjša, približno 8,2 milijarde USD, večina pa je šla le nekaj kandidatom, kot so monoklonaalna protitelesa. Dr. Ian Lipkin je direktor Centra za okužbe in imuniteto na Columbia School of Public Health. Lipkin je v intervjuju priznal, da so nacionalne prednostne naloge v zvezi s pandemijo želja po ustvarjanju novih patentov in nov dobiček.
*
V Izraelu razvijajo zdravilo (faza1) - beljakovino EXO-CD24, ki uporablja eksosome za dostavo zdravila v pljuča, kjer zavira vnetne citokine in s tem prepreči smrtonosno citokinsko nevihto.
https://www.dailymail.co.uk/news/article-9228317/Experimental-cancer-drug-hailed-coronavirus-cure-Israeli-hospital.html
https://www.italy24news.com/en/2021/02/has-israel-found-the-cure-for-covid-all-about-exo-cd24-and-allocetra-drugs.html
https://www.jewishpress.com/news/israel/innovative-israeli-corona-drug-cured-96-of-patients-in-phase-one-test/2021/02/04/
*
ZDRAVILO KOLHICIN
Od marca 2020 dalje je v raziskavi sodelovalo 4488 covid bolnikov in rezultati so nadvse obetavni. Pri bolnikih, ki so jemali kolhicin, je bilo kar za 20 odstotkov manj hospitalizacij ali smrti. Pri pacientih z uradno diagnozo covid-19 je bil rezultat še boljši: 25 odstotkov manj hospitalizacij; 50 odstotkov manj potreb po ventilatorjih; ter 44 odstotkov manj smrti.
Hipoteza za študijo je bila, da pri nekaterih covid bolnikih pride do komplikacij zaradi pretiranega odziva imunskega sistema, ko se bolniku razvijajo bele krvne celice kot odziv na virus. Če se torej uporabi močno protivnetno terapijo, kakršna je npr. zdravilo kolhicin, se ta odziv, imenovan citokinska nevihta, zmanjša – s tem pa tudi možnost za komplikacije.
Kolhicin je izjemno močno protivnetno zdravilo, odkrito že pred 150 leti, in ga pridobivajo iz rastline Colchicum autumnale. Uporablja se za zdravljenje različnih bolezni, med drugim protina, vnetnega artritisa, perikarditisa in drugih.
https://m.planet-lepote.com/colchicine-kolhicin-se-eno-zdravilo-za-covid-19/
*
Komentatori na našem portalu postavljaju odlična pitanja, a ima i sjajnih, vrlo informativnih komentara. Kako danas dobih jedan mail našeg posdoktoranta Sveučilišta u Utrechtu, Stipe Pandžića, red je ovu vrlo kvalitetno obrađenu analizu te kontekst događanja oko Ivermektina objaviti kako bi naši čitatelji, ali i mnogi drugi, bili na vrijeme ali i detaljno informirani.
A Stipe Pandžić piše u mailu slijedeće:
Prije svega, molim vas za razumijevanje jer pišem poruku iz perspektive zabrinutog laika, a ne medicinskog eksperta, premda je sadržaj ove poruke informacija koja je primarno medicinski relevantna.
Od kraja prošle godine pratim proces odobravanja, administriranja Ivermektina u covid profilaksi i tretmanu COVID pacijenata. Zapravo, bolje rečeno, pratim proces suzbijanja odobravanja Ivermektina za liječenje COVIDA-a. Što je Ivermektin? Ivermektin je supstanca otkrivena 1975. godine, čija je primarna upotreba liječenje parazitskih infekcija. Uspješno je upotrebljavan u Africi protiv niza parazitskih oboljenja, zbog čega je otkriće Ivermektina 2015. nagrađen Nobelovom nagradom za medicinu.
Priča o Ivermektinu i COVID-u započela je u proljeće 2020. studijom znanstvenika s Monash Sveučilista prema kojoj Ivermectin uništava SARS-CoV-2 in vitro unutar 48 sati.
Ova studija potaknula je niz neovisnih liječničkih centara u kojima se Ivermektin eksperimentalno administrirao u “živim uvjetima” u profilaksi i liječenju COVID pacijenata. Dobar dio pobornika ovog lijeka vremenom se okupio unutar udruženja FLCCC, ciji je idejni vođa Prof. Paul Marik. Cilj osnivanja FLCCC-a bila je prenamijena postojećih lijekova u suzbijanju pandemije (medju ostalim, razmatrali su ulogu kortikosteroida, vitamina D etc.).
Primjena Ivermektina u suzbijanju COVID-a pokazala se toliko učinkovitom da je doktor Pierre Kory u svom pozvanom predavanju ispred US senata nazvao ovaj lijek “čudesnim” s garancijom da se nećete razboljeti od COVID-a ukoliko ga uzimate.
Povrh profilaktičkog djelovanja, postoje podaci od tisuće COVID pacijenata koji pokazuju da se viralno opterećenje značajno smanjuje nakon nekoliko dana primjene Ivermektina. Što se dogodilo nakon toga ohrabrujućeg svjedočanstva?
Nažalost, spregom medijske kulture, birokracije i farmaceutskih autoriteta, (gotovo) ništa dobro se nije dogodilo. Uslijedio je niz događaja koji se dobro uklapaju u rječničku definiciju “cenzure”.
Najprije je Youtube maknuo govor Dr. Pierre Korya pred Senatom nakon sto je pregledan više od milijun puta. Nota bene, ovo je učinjeno pod izlikom zaštite od misinformiranja, prema čemu se Youtube (Google) propagira kao medicinski autoritet iznad skupine visoko citiranih znanstvenika). Potom je, u neviđenoj akademskoj travestiji, časopis Frontiers in Pharmacology najprije prihvatio pa, nakon online publikacije, maknuo studiju o Ivermektinu. U studiji se preporučuje hitno usvajanje Ivermektina u liječenju COVID pacijenata na temelju više od 20 neovisnih trial studiesa. Npr. jedan od triala je obavljenj u Argentini, vođen od Dr. Hector Carvalloa, sa sljedećim ishodom: od 1200 sudionika ukupno, medicinskih radnika, od 800 onih koji su “bili na” Ivermektinu, nijedan oboljeli. Od ostalih 400 koji nisu uzeli Ivermektin, 240 (blago ili teže) oboljelih. Dakle, nakon tri runde recenzija s četiri recenzenta i prihvaćanja, Frontiers in Pharmacology miče studiju s objašnjenjem da su stanoviti “vanjski eksperti” pronašli neosnovane tvrdnje u studiji. Svatko tko se razumije u postupak vršnjacke recenzije vidi da je ovo flagrantna povreda znanstvene procedure. Srećom, nakon ponovnog slanja u American Journal of Therapeutics, članak je nedavno prihvaćen za objavu i uskoro će se vjerojatno pojaviti na njihovom websiteu (tekst u privitku).
Povrh suzbijanja, časopis JAMA objavljuje studiju iz Calia u Kolumbiji koja opovrgava djelatnost Ivermektina uz nebrojene propuste istraživača i nekonkluzivne rezultate (vidljivo u komentarima na studiju). Ova studija se brzinom svijetlosti proširila u Nizozemskoj putem Volkskrantovog teksta “Ivermektin ne radi ništa” i Twittera, gdje je taj dan Ivermektin bio 4. najtraženiji pojam. S druge strani, mediji nisu popratili niti jednu od uspješnih studija u raznim dijelovima svijeta koje pokazuju učinkovitost Ivermektina (studije lako dostupne putem Google Scholara). Borba za medijsku pozornost pozitivnih učinaka je neumoljiva, čak i kada renomirani znanstvenici pokušavaju plasirati upotrebu Ivermektina kao rješenje pandemije. Primjer je WHO-ova konzultantica Tess Lawrie iz UK-a koja je napravila meta-analizu svih dostupnih studija o Ivermektinu sa zaključkom da smanjuje smrtnost za oko 70 %. Inače, meta-analize trial-a su ključne u usvajanju lijeka od strane agencija, ali ne i u ovom slučaju dano na panel diskusiji.
Ovo je samo dio cijele priče, ali siguran sam da ste dobili dojam općeg tijeka.
Koji je razlog suzbijanja ovog lijeka? Dokaza nema, ali mnogi upućuju na to da ovaj izuzetno jeftini, sigurni (incidencija nus-pojava samo 160 puta na milijarde primjena!) i široko-dostupni lijek ne odgovara interesima farmaceutske industrije i prirodi ugovora koje oni sklapaju s vladama zapadnih zemalja. Nisam sklon teorijama zavjera i ne bavim se spekulacijama, pa o tome ne bih dalje ovdje.
Zašto šaljem ovu poruku vama. Dva su razoga. Prvi je razlog to što vidim da je ovaj lijek nezamijećen u Hrvatskoj javnosti, a u Nizozemskoj je, npr., sustavno misreprezentiran.
Iako medicina nije domena mojih kompetencija, upoznat sam s procesom peer reviewa i trial studiesa te se nadam da u uvjetima u kojima je svijet “zakočen” na godinu dana ovaj lijek s izvrsnim rezultatima, širokom dostupnošću (za razliku od cjepiva), niskom razinom rizika te preventivnim i tretmanskim potencijalom može i mora biti prepoznat od javnosti. Siguran sam da među vama ima onih koji će ovo proučiti i uzeti za ozbiljno, a nadam se i onih koji mogu nešto korisno učiniti s ovom informacijom na korist šire javnosti.
Drugi razlog je to što vam nisu dostupna. U tom slučaju (iako sam dobro uradio “domaću zadaću” i proučio različite izvore i podatke) konzultirajte medicinske stručnjake koji makar nešto znaju o Ivermektinu (komercijalna varijanta je najčesće Stromectol) i moju informaciju uzmite cum grano salis (sa zrnom soli, razumno, oštorumno i pametno).
https://www.youtube.com/watch?v=ypxrJhSg5xU
*
https://thecovidblog.com/ivermectin/?__cf_chl_jschl_tk__=4f7e4a62a8cf30e9271e56782f63915514f41301-1618321390-0-AaX1Qll91V8DQmtst7vgN-YciNQlDK2A4fIG-R1FWsPa0xhmpGKd0GiI5BM-avlwtX4kXjgc5jCE149jpcmrDgg8sm2oAf_OkPpjCx5mPuNSFNzV7ytMsSLD61PCs-vxQyHkw0KaIwOgsCp7C_px1YJM9QfLg-MmThKi5uU4SrhVeum2e7o91m_mr827f_rQ7LDBXG5r1dtDW8ziVLe1r7bzGpwTZ0WY91Bz2Iyu4Om1t7q5749psCxExQ5iKzh38Z4o0K_IG7a5a0pb7LhIraCO8ibTDmkyyLoO3p4sDJa49uMZBZuNiEAD-5EcIpvTIpcdxZRSBk-Y5e6vDBEZsegjzaElHOtDMgAzWGXD2uleLVs0V-wFxR_F3ie4i4g8KQoXm9A9PMTs8bbXOQAYCNM
*
Dr. Simone Gold, zdravnica in pravnica iz American Frontline Doctors o hidroksi klorokinu in Ivermectinu:
*
https://www.logicno.com/hrana-zdravlje/ekskluzivno-protokol-didier-raoult-za-ambulantno-zbrinjavanje-bolesti-covid-19.html
*
Ivermectin Wins in Court Again: For Human Rights
- Apr 19, 2021 Updated Apr 21, 2021
One dose of Ivermectin was all it took to get 81-year-old John Swanson off the ventilator. John’s wife Sandra could not believe it. His story is remarkably similar to other cases of patients who were on their way out with advanced COVID-19 but saved when Ivermectin was added.
Ralph Lorigo is the lawyer who now has won three court orders forcing New York hospitals to administer Ivermectin to dying patients. Incredibly, these three hospitals and their lawyers fought against the patients, arguing they did not have the right to receive the drug despite a valid prescription written by their doctors. In essence, the argument was that they did not have the right to try a potentially life-saving medication.
In each of the three cases, the New York State Supreme Court Justices sided with the patient, and in each of the three cases, the patients made near-miraculous recoveries after the Ivermectin was given. In each case, these patients were in the Intensive Care Unit on ventilators, unable to breathe on their own, and universally, after the drug was given, they rapidly improved and were able to breathe on their own.
Judith Smentkiewicz made national news in January when her family hired Lorigo after the hospital refused a fourth dose of Ivermectin. Smentkiewicz's son and daughter called Ivermectin a "miracle drug" in court papers. Attorney Lorigo and his associate Jon F. Minear reported, “This lady was on a ventilator, literally on her deathbed, before she was given this drug. As far as we’re concerned, the judge’s order saved this woman’s life.”
The family of Glenna "Sue" Dickinson happened to see a newspaper article of Judith's remarkable story, and they decided to try Ivermectin as well.
Sue Dickinson, 65, contracted COVID-19 on January 7, 2021. She suffered progressive worsening and was admitted to Rochester General Hospital on January 12. She continued to worsen and was placed on a ventilator on January 17. The hospital staff advised that her chances of survival were about 40 percent.
With nothing to lose, Natalie Kingdollar, Dickinson’s daughter, reached out to their family doctor, Tom Madejski, who wrote the prescription. The hospital refused to give Sue the Ivermectin. The legal team of Lorigo and Minear drafted an affidavit from Dr. Madejski and sought an injunction. State Supreme Court Justice Frank Caruso ordered the hospital to provide the Ivermectin.
Dickinson, like Swanson, and Smentkiewicz, came off the ventilator and improved as well. The family reported on Facebook that, "She’s making progress each day, and it’s Ivermectin and God making this happen.” She has since been released from the hospital.
Ivermectin is widely used by physicians, as there are now 51 studies from around the world, with 50 showing clear benefit and one showing neutral. However, the lone study showing a neutral effect was roundly criticized as flawed in an open letter signed by a group of 120 physicians.
Experts worldwide have called for the global and systematic use of Ivermectin to prevent and treat COVID-19. Physicians have recently written about a profit motive by regulatory agencies and Big Pharma to block cheap, safe, and effective treatments like Ivermectin and HCQ in favor of experimental and perhaps more dangerous and arguably less effective vaccines and medicines like Remdesivir. With Remdesivir costing $3,100 per dose and not reducing deaths, the choice of Ivermectin is a no-brainer say many doctors.
Ivermectin costs about $2 per dose. It is safer than Tylenol or most vitamins, says Dr. Pierre Kory of the FLCCC Alliance, a group of expert physicians promoting access and information through a nonprofit organization. Dr. Kory and Mr. Lorigo have teamed up to help other hospitalized patients gain access to the life-saving drug.
Dr. Fred Wagshul, a Yale-educated physician, is a pulmonary specialist and directs the Lung Center of America. He is also a founding member of the FLCCC Alliance. Dr. Wagshul notes that the typical dose for hospitalized patients is 0.3 mg of Ivermectin per kg of body weight for four days which works out to nine 3 mg tablets daily for four days in a typical 200-pound patient.
Dr. George Fareed, former Harvard professor, advocates combination therapy of Ivermectin with HCQ in outpatient cases. For the benefit of physician readers, the specific doses are provided in this link.
The big problem is that information promoting Ivermectin is often censored or silenced as quickly as it is provided. Facebook, Reddit, Change.org, YouTube, and others have recently taken down posts on Ivermectin citing violation of "community standards."
Physicians who employ good judgment and scientific studies are considered violators, as well as those who publish factual accounts of Ivermectin-based recovery stories. A recent article exposed the link between large pharmaceutical corporations and government regulatory agencies who have financial entanglements and massive conflicts of interest.
The disinformation campaign is evident with the publication of articles attempting to cast Ivermectin in a false light, referring to it as an “animal dewormer” that might be a “bad idea” for humans to use. In reality, many drugs are common to both humans and animals for treatment, including antibiotics, antifungals, and antiparasitic agents.
Ampicillin, a form of penicillin, has been widely used to treat infections in children like whooping cough, salmonella, and meningitis. It has been routinely used to treat adults for bronchitis, pneumonia, and rheumatic heart disease. It is also consistently employed in veterinary applications to treat calves, cattle, dogs, and cats.
You would never see an article attempting to smear Ampicillin as an animal drug and warn people against taking it. However, we see this propaganda daily trying to influence the general public against Ivermectin, a life-saving drug that has been prescribed safely and in billions of doses over the past 40 years for parasitic disease.
Dr. Satoshi Omura won the 2015 Nobel Prize in Medicine for his discoveries leading to the development of Ivermectin. In his praise for Ivermectin and its potential to help in the COVID-19 pandemic, Dr. Omura recently compared Ivermectin to Penicillin, “one of the greatest discoveries of the twentieth century.”
Currently, Ivermectin has already been adopted by 25 percent of the world’s countries to prevent and treat COVID-19. Bangladesh, where Ivermectin is broadly used in almost every home, enjoys a 99% lower per capita death rate from COVID-19 than the US. Bangladesh, with 160 million inhabitants, has half the US population. However, it has merely 10,000 COVID-19 deaths. Contrast that with nearly 580,000 US deaths in our country of 327 million.
However, censorship, corruption, hospital lawyers, and disinformation campaigns have continued to stand in the way of its widespread acceptance in the United States. Many have never even heard of it.
Ivermectin recently won in court in South Africa after a protracted legal battle. Ralph Lorigo has now won his third State Supreme Court Injunction in New York. Will legal strategies also be required in the US to gain FDA approval for Ivermectin to treat COVID-19?
Dr. Tess Lawrie has entered this David v. Goliath battle. She is an independent research consultant to the WHO, and her work has consistently been used to underpin International Clinic Practice Guidelines. In other words, she has been one of the go-to scientists on which the WHO bases their recommendations.
She has established a non-profit organization to promote the worldwide approval and adoption of Ivermectin for COVID-19. She is requesting support through this video.
We owe it to ourselves as human beings to support this work. We owe it to future generations who need medical truth, not corruption, to guide our public health policy. We owe it to the principle of basic human rights.
Signed,
Justus R. Hope, MD
https://www.thedesertreview.com/opinion/letters_to_editor/ivermectin-wins-in-court-again-for-human-rights/article_98d26958-a13a-11eb-a698-37c06f632875.html
* * *
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7129059/
https://assets.researchsquare.com/files/rs-100956/v2/39b225ad-5df4-4da7-9cbd-233bf26a0eb4.pdf
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7698683/#bib0019
*
Predstavnici Kršćansko-socijalne unije (CSU), konzervativne političke stranke u Njemačkoj, koja je usredotočena na južni dio Njemačke, nedavno su istupili u javnosti pozivajući njemačku vladu da financira istraživanje o povezanosti između ivermektina i COVID-19. Parlamentarna skupina CSU-a sada vodi kampanju za istragu vezanu za ivermektin, kao dio vladine potpore istraživanjima vezanima za COVID-19. Predali su zahtjev zdravstvenom odboru, kojim traže da njemačka vlada podrži značajne kliničke studije kako bi se omogućilo pravilno testiranje na koronavirus. Na čelu s Bernhardom Seidenathom, predsjednikom Odbora za zdravstvo i njegu bavarskog državnog parlamenta, ova skupina pokušava saznati mogu li se nabaviti lijekovi koji u sastavu imaju ivermektin i to za liječenje bolesnika te regije, koji su oboljeni od COVID-19.
https://dokumentarac.hr/covid-19/njemacka-konzervativna-stranka-iz-bavarske-podrza-odobravanje-klinicke-studije-vezane-za-lijek-invermektin/
*
Šezdesetosmogodišnja žena je nadomak smrti dok se njezina obitelj sudi s bolnicom koja joj odbija dati lijek koji ima odobrenje Savezne agencije za lijekove, a koji je pomogao drugim oboljelima od bolesti COVID-19 u kasnoj fazi bolesti.
Nekoliko obitelji sudski se uspjelo izboriti da njihovi najbliži u bolnicama dobiju lijek ivermektin. No, situacija Nurije Fype je neviđena – ovo je prvi slučaj u kojem se ustanova, bolnica Elmhurst pokraj Chicaga, suprotstavila sudskoj odluci.
Ralph Lorigo, odvjetnik pacijentice, i Desareta Fype, njezina kći, ne odustaju od borbe. U petak, 30. travnja, dobili su sudski nalog za davanje lijeka, ali ga je bolnica odbila.
U žurno dogovorenom konferencijskom razgovoru, Lorigo je predložio sucu: „Pošaljite šerifa u bolnicu i recite upravitelju da se mora pridržavati naredbe. Ako odbije, stavite ga u zatvor. “
No, unatoč nestabilnom stanju gospođe Fype – u JIL-u i na respiratoru od 28. ožujka – sudac će tek u ponedjeljak, 3. svibnja, odlučiti hoće li utvrditi da bolnica ne poštuje nalog, kako Lorigo traži, i zatražiti prisilno izvršenje odluke.
“Jednom odvjetniku s 47 godina prakse nezamislivo je da postoji bolnica koja odbija izvršiti sudski nalog”, rekao je odvjetnik Lorigo.
Desareta Fype, čija je majka doživjela srčani zastoj neposredno prije intubacije, tvrdi da je “bijesna, uništena i frustrirana” zbog otpora bolnice. “Nastavit ću se boriti za njezin život”, rekla je, savjetujući i druge ljude u sličnoj situaciji da se educiraju i informiraju kako bi mogli napraviti “pravi izbor”.
Glasnogovornik bolnice u međuvremenu je e-mailom poručio: “Ne možemo komentirati slučaj zbog zaštite privatnosti pacijenta.”
Odvjetnik Ralph Lorigo imao je već tri uspješno sudska postupka u čijem je središtu bio lijek ivermektin. U tri savezne države New Yorka, hospitalizirani pacijenti s COVIDom, stari 65, 80 i 81 godinu – dobili su lijek nakon sudskog naloga i oporavili se.
Sudar Titana
U drugom od dva slučaja koji su još u tijeku, ivermektin je zatražen za Deborah Bucko, 52 godine, u bitci koju je Lorigo opisao kao “sudar Titana”.
U tom slučaju ogroman medicinski lanac, zdravstveni sustav Mount Sinai, je u sukobu sa dr. Pierreom Koryjem, predsjednikom Saveza za kritičnu skrb Front Line COVID-19 (FLCCC), i priznatim vodećim globalnim zagovornikom ivermektina. Deborah Bucko je primila petodnevnu dozu ivermektina u skladu sa sudskom odlukom, stanje joj je poboljšano, ali još nije izvan opasnosti.
Njezin suprug Scott Mantel sada želi da bolnica Mount Sinai Nassau South nastavi liječenje prema ažuriranim smjernicama FLCCC, što znači dodatni ivermektin u većoj dozi, sve do njezina oporavka. Bolnica odbija to učiniti i rasplet se uskoro očekuje na sudu.
U svojoj izjavi, šef bolnice dr. Aaron Glatt, ustvrdio je da ivermektin uopće nije smio biti davan jer „nije u skladu sa Smjernicama zdravstvenog sustava Mount Sinai“, koje se temelje na „preporukama medicinskih udruga, međunarodnih vladinih agencija i mišljenja stručnjaka za zarazne bolesti objavljenih u medicinskim časopisima.”
Konkretno, rekao je da “nema klinički prihvatljivih podataka o istraživanjima koja podupiru uporabu ivermektina za liječenje bolesti COVID-19 kod ozbiljno bolesnog pacijenta, poput gospođe Bucko, koja je već duže vrijeme na respiratoru.”
Bucko “nije reagirala” na petodnevno liječenje ivermektinom, navodi Glatt. “Njena prognoza je, nažalost, i dalje loša.”
Dr. Kory tvrdi, međutim, da Glattova izjava sadrži “brojne pogreške, netočnosti i kriva tumačenja”. Glattova tvrdnja da mnoge agencije “jednako” odbacuju ivermektin, “netočna je i zastarjela”.
Kory je naveo neutralni stav Nacionalnog instituta za zdravstvo, koji liječnicima omogućuje upotrebu ivermektina, kao i nedavni članak Američkog društva za zarazne bolesti u kojem se navodi da se dokazi “uglavnom sastoje od pozitivnih rezultata manjih istraživanja”. Sedam je zemalja nedavno uvrstilo lijek u svoje smjernice za liječenje, dok pet osvrta iz medicinske literature podupire njegovu upotrebu.
Dr. Kory ukazuje na činjenicu da je kod bolesnika u teškoj fazi poput gđe. Bucko, zaprepašćujuće smanjenje smrtnost. Prema istraživanju iz Floride na koje se poziva, smrtnost najteže oboljelih pacijenata pala s 80 na 30%.
Znakovito je, piše Kory, da se stanje gospođe Bucko popravilo nakon tretmana, uz “značajno smanjene potrebe za kisikom i respiratorom”. Tri dana nakon završetka liječenja ivermektinom, napisao je, “radiografija prsnog koša pokazala je smanjenje abnormalnih pojava”, uz ostala naknadna poboljšanja.
“To je u suprotnosti s izjavom dr. Glatta da nisu zamijećena poboljšanja”, napisao je Kory. “Medicinska dokumentacija jasno pokazuje značajno poboljšane respiratorne i kardiovaskularne funkcije otkako je započeto liječenje ivermektinom.”
Pogledajte dokaze
U telefonskom intervjuu dr. Kory je o oba slučaja govorio kao o primjerima neuspjeha medicine tijekom pandemije.
“Ovi liječnici odbijaju pogledati nove dokaze, svjesno su neuki i bore se svim snagama protiv jednog od najsigurnijih lijekova u povijesti”, rekao je Kory. “Pogledajte nove dokaze i djelujte brzo.”
“Šokiran sam pretjeranim oslanjanjem na javne zdravstvene službe koje preporučuju liječničke postupke”, dodao je. “Ovako se liječi.”
Odvjetnici gospođe Fype likovali su – nakratko – kad je sud presudio u petak da joj se neodgodivo mora dati terapija ivermektinom, jer na ročištu u sudu nije bio nitko iz bolnice, a nakon toga ignoriraju odluku suda.
U kasnijem telefonskom pozivu odvjetnik Lorigo zatražio je od suca da djeluje, istaknuvši da se radi o pitanju života i smrti, na što je sudac uzvratio da, iako suosjeća, trenutno jedini pravni način za daljnju borbu koji može predložiti je tužiti bolnicu za neposluh.
U Lorigovim drugim uspješnim slučajevima, protiv bolnica u Buffalu, Rochesteru i Bataviji u New Yorku, tri su pacijenta bila na intenzivnim odjelima i na repsiratorima nakon čega su im dali ivermektin. Lorigo je rekao da je dvoje sada kod kuće, dok se najnoviji pacijent koji je liječen početkom travnja nalazi u rehabilitacijskoj ustanovi.
Lorigov prvi slučaj bila je Judith Smentkiewicz, aktivna 80-godišnjakinja koja je živjela samostalno, a prije nego što je dobila ivermektin, imala je navodno 20 % šanse da preživi COVID-19. Danas je ona “kod kuće i živi svoj život onako kako je uvijek živjela.”
Ova pacijentica je imala veliku sreću što je imala srčanu i hrabru obitelj, te materijalnu mogućnost da se pravno izbori kako bi dobila traženi lijek, unatoč protivljenju bolnice čak i nakon sudskog naloga. Hvala Bogu, lijek je ipak dobila te tako spasila svoj život! Pitamo se koliko li je ljudi, radi krivog liječenja umrlo, a moglo je biti spašeno pravovremenim i vrlo kvalitetnim i jeftinim tretmanom. Možda je upravo to i razlog, jer onda se ne bi moglo opravdati postojanje javnozdravstvene prijetnje, mjera i pandemije koja već drugu godinu za redom “resetira” postojeće socio-ekonomsko “biće” čovječanstva u novi oblik tehnološkog-neofeudalizma? Još kada uz to dodamo bolnu i tužnu činjenicu da u mnogim državama SAD-a, a posebno državnim bolnicama, iste u svoj budžet dobivaju dodatke za tzv. COVID-19 pacijente , što onda može više objasniti strogo držanje protokola koje očito nemaju za cilj spašavanja života ljudi, koliko održavanja statusa pandemije u jednu ruku, te sa druge strane punjenja proračuna samih bolnica. Već smo prethodno pisali da pravila FDA ne dozvoljavaju “hitno ograničeno odobrenje” za cjepiva koja nisu završila sa svim fazama kliničkih ispitivanja, a znamo da ni jedno postojeće cjepivo protiv COVID-19 to nije. Kako bi FDA moglo dati takvo ograničeno odobrenje moraju se ispuniti dva uvjeta, a to je da mora postojati stanje hitnoće (poput pandemije) i da ne postoji lijek ili tretman dovoljno kvalitetan koji može spriječiti ili izliječiti takvu bolest (što očigledno po svim znanstvenim spoznajama ivermektin, hidroksiklorokin i visoke doze D3 vitamina svakako postižu, pogotovo u ranoj uporabi). No onda cijeli COVID-19 projekt, te s njim cijepljenje, cijepne putovnie, kontrole stanovništva kroz QR kodove itd pada u vodu.
Zato je pitanje ivermektina od suštinske važnosti za spašavanje kako pojedinačnih života ljudi oko nas, ali i naše kompletne civilizacije, dok još imamo vremena.
https://dokumentarac.hr/covid-19/sudska-bitka-za-spasavanje-zivota-ivermektinom/
*
https://dokumentarac.hr/novosti/zasto-ivermektin-djeluje-i-gdje-ga-kupiti/
https://dokumentarac.hr/novosti/zapocela-je-borba-protiv-jeftinog-i-visoko-ucinkovitog-ivermektina/
Dr. Jackie Stone o uporabi Ivermectina: https://www.youtube.com/watch?v=DtoOw9VqjI0
*
STORY AT-A-GLANCE
- Multiple studies have demonstrated successful treatment of COVID-19 with ivermectin, which lowered mortality rates, shortened hospital stays and limited viral spread
- Although billions of doses have been used in the last 30 years, Merck now says there is a concerning lack of safety data and the WHO is concerned it may create "false confidence"
- The WHO ignored their own commissioned report that found using ivermectin could cut COVID-19 deaths by 75% and instead cherry-picked data to support the subsequent recommendation that the drug be used only in clinical trials
- The unsubstantiated war against ivermectin has followed in the footsteps of the hydroxychloroquine story and bears a strong resemblance to the lies perpetrated by the tobacco and sugar industries
The growing fear during this pandemic is second to nearly no other time in medical history for the depth and breadth of the strategies used to stoke those fears. Emergency use orders, mask mandates and the suppression of health information all support public fear over a viral illness with a survival rate of over 99%.1 Ivermectin has fallen victim to these strategies.
It bears repeating that a review of the literature by respected Stanford University professor of medicine and epidemiology John Ioannidis,2 published in the Bulletin of the World Health Organization,3 found the infection fatality rate for COVID-19 as of September 2020, was 0.23%. In people younger than 70 years the median was even lower.
The study4 was undertaken to look at the different death rates across a variety of locations and included 61 studies and preliminary national estimates. The infection fatality rate is the number of deaths divided by all people who were infected.
But the fear generated by this pandemic is not one-sided. The suppression of information supported by corporations, the pharmaceutical industry and government agencies is an indication of how nervous they are and how far they are willing to go to ensure that the level of public fear remains high enough to ease the burden of manipulating behavior.
Consider the statistics from the U.S. Centers for Disease Control and Prevention. In 2019, 4.6% of the U.S. population was diagnosed with heart disease.5 The population at the end of 2019 was 328,239,523.6 This means there were 15,099,018 people with heart disease in the U.S. in 2019. There were 659,041 people who died that year from heart disease,7 which is a death rate of 4.3%.
This is 18.6 times greater than the death rate from COVID-19. Yet these same agencies were not lobbying for mandates against soda or sugar-laden foods; they weren’t banning smoking and they weren’t mandating exercise — all heart disease risk factors.8
Studies Demonstrate Ivermectin Effective Against COVID
Treatment for COVID-19 is not the first time that ivermectin has been investigated for its antiviral properties. The long list of potential antiviral effects for ivermectin include Zika virus, influenza A, Venezuelan equine encephalitis and West Nile virus.9
The development of the drug originated from a microbe in the soil found in Japan. This discovery by two scientists led to the development of ivermectin and earned them the 2015 Nobel Prize in Physiology or Medicine. According to papers published before 2020, ivermectin continued:10
“… to surprise and excite scientists, offering more and more promise to help improve global public health by treating a diverse range of diseases, with its unexpected potential as an antibacterial, antiviral and anti-cancer agent being particularly extraordinary.”
However, all that changed as pharmaceutical companies fought to develop the first drug or vaccine that could cure or prevent COVID-19. Ivermectin is a relatively inexpensive drug costing from $17 to $77 per prescription11 as compared to remdesivir that costs $3,120 for a typical course of treatment.12
Unlike the clinical trials testing remdesivir, which provided disappointing results and significant side effects, ivermectin has a 30-year history of impacting lives throughout the world and “proved ideal in many ways, being highly effective and broad-spectrum, safe, well tolerated and could be easily administered (a single, annual oral dose).”13
In June 2020, researchers published14 an in vitro lab study demonstrating ivermectin effectively reduced the viral load in cell culture 5,000-fold. The information quickly triggered dissent within the scientific community. One group believed the levels of ivermectin used in the lab were too high to achieve results in humans without triggering significant side effects.
Others were willing to use ivermectin at safe dosages without clinical trials demonstrating its effectiveness. One paper15 reported the results of a discussion of senior physicians from the Academy of Advanced Medical Education.
The doctors concluded the antiviral properties of ivermectin made it a potential prophylactic and treatment approach that may effectively reduce the burden of COVID-19 based on availability, safety, good tolerability and cost effectiveness. Other groups of doctors and researchers began studying the safety and effectiveness in the treatments of COVID-19. The results proved promising.
Ivermectin Lowered Mortality and Shortened Hospitalization
In one study,16 400 symptomatic and confirmed COVID-19 patients received ivermectin and reported early and substantial recovery documented by laboratory results. Another study17 found patients treated with ivermectin had a lower mortality rate, including those with severe pulmonary involvement.
Interestingly, the mortality rate was significantly lower in the group receiving ivermectin, although most also received hydroxychloroquine and azithromycin. While researchers were testing ivermectin against severe disease, another group published results18 finding there was no difference in patients who received a placebo or ivermectin.
In this study, 12 people received ivermectin and 12 received a placebo. There were no patients with severe illness, and none had risk factors for complicated disease. In other words, in this extremely small group it appeared illness in people with mild COVID-19 did not respond to ivermectin.
A retrospective study19 of 325 consecutive people with COVID-19 infection showed ivermectin induced rapid clearance of the virus indicating the drug limited viral spreading and controlled the course of the disease, lowering the mortality rate and shortening hospital stays.
The Unsubstantiated War Against Ivermectin
Although ivermectin has demonstrated significant success against COVID-19, the war against the drug does not stem from an argument over effectiveness, but rather one of politics. One of the underlying problems with approving drugs that are highly effective and inexpensive is that an emergency use vaccine could not be approved.
In a recent press release, the FDA admits to not reviewing data that support the use of ivermectin in COVID-19. Yet they state: “Taking a drug for an unapproved use can be very dangerous. This is true of ivermectin, too.”20 It should come as no surprise that taking high doses of many drugs can be dangerous.
However, ivermectin has been distributed billions of times over 33 years and has been especially effective in rural communities destroyed by river blindness (onchocerciasis). For this disease, Merck donated ivermectin for as long as needed, which gave birth to the Mectizan Donation Program dedicated to eradicating river blindness.21
As in the fight against hydroxychloroquine, most of the disinformation spread about ivermectin is being repeated without checking the sources. One of the myths being perpetuated is based on the initial lab study demonstrating a 5,000-fold reduction in viral load.
News organizations,22 the NIH23 and the World Health Organization24 are repeating information that appears to fit their agenda — that the dose of ivermectin must be dangerously high to achieve results. Yet, the standard human dose given in the studies above were effective in lowering the viral load, shortening hospital stays and reducing mortality rates.
Although ivermectin is commonly used in animals, it's important to remember that the drug has been used in humans for over 30 years. It is important not to use ivermectin manufactured for veterinary use, since these formulations are highly concentrated for large animals and the dose is significantly higher than is safe in humans.
It appears the World Health Organization is concerned that using ivermectin may create a “false confidence” in those taking the drug.25 Yet, the same can be said for using the vaccine since after vaccination you may continue to shed the virus, may still get sick and can still experience significant side effects, including death.26
Many of the official decrees pertaining to ivermectin do not line up with the facts. For example, the WHO commissioned an analysis27 that found ivermectin would cut COVID-19 deaths by 75%. WHO ignored this analysis and chose another team to cherry-pick evidence, finding the effectiveness was far lower than the first commissioned analysis.
Flawed Information Used to Justify Recommendations
The result was a recommendation to limit the use of ivermectin except in patients who had enrolled in a clinical trial.28 On top of that, social media platform YouTube has taken up the banner to censor content related to ivermectin or hydroxychloroquine, covering this under their “medical misinformation policy.”29
Since Google owns YouTube, you can well imagine this same policy extends to the results from the search engine that commands 92.41% of the global search market share.30
TrialSite News31 followed up on the FDA’s announcement32 that they had received “multiple reports of patients who have required medical support and been hospitalized” after using a form of the drug for veterinary medicine in horses. The TrialSite reporter could not find information about the number of people and so contacted the FDA.
The answer was four. They recorded three people who were hospitalized but had no further information. The FDA spokesperson explained in an email to the reporter, “Some of these cases were lost to follow up, so we can’t be sure of the final outcome.”33 In other words, the only cases of adverse effects from using ivermectin were from people who were using doses meant for animals weighing 900 to 2,000 pounds.34
The WHO report included a flawed study published in the Journal of the American Medical Association.35 Not long after, an open letter signed by 120 doctors from the U.S. critiqued the study, calling the results into serious question.36
The group identified several issues, including the median age in the participants was 37 with a BMI of 26, placing them in a low-risk category for COVID-19. The primary endpoint was moved halfway through the study and the information from the participants was gathered through a telephone survey and not clinical evaluation.
Despite years of safety data and assertions that ivermectin is a safe and essential medication in the treatment of parasitic infections, Merck suddenly turned in February 2021 and stated there was “a concerning lack of safety data in the majority of studies.”37
Does this mean the drug has been responsible for significant adverse effects in the last 33 years without being recognized? TrialSite News38 points to the organized and aggressive campaign to remove “misinformation” from Twitter, LinkedIn, Facebook and YouTube, which the media have barely noticed.
This seems strange since the news industry is founded on free expression and free speech guaranteed by the First Amendment to the U.S. Constitution.39 While most media outlets are intentionally overlooking this blatant disregard of the First Amendment, what happens when the stories they want to tell are suddenly deemed “misinformation”? Will they stand and fight or roll over as it appears they are doing now?
Hydroxychloroquine Squelched in Similar Battle
At the start of the COVID pandemic, many doctors began using the antimalarial drug hydroxychloroquine with great success. This garnered the attention of pharmaceutical giants and those they influence, since hydroxychloroquine is relatively inexpensive and offers small financial gain.
Instead, pharmaceutical companies were aiming at expensive new antiviral drugs or vaccines that could net billions of dollars in the coming years. Not long afterward, there were fraudulent and misleading studies published about the drug to squash public interest in an effective and low-cost solution.
As I discussed in “NY Doctor Proved Everyone Wrong About Hydroxychloroquine,” both the Solidarity Trial,40 led by the WHO, and the Bill & Melinda Gates Foundation-funded Recovery Trial,41 administered high doses of the drug.
It’s also significant to note that previous to this the hydroxychloroquine safety profile was already well-established with upper limit thresholds well-understood. It has been in use since the early 1950s in the treatment of systemic lupus erythematosus.42
The drug is also used for rheumatoid arthritis and studies show those treated with hydroxychloroquine had a lower risk of developing diabetes. This means the upper limit of the drug was well-known and should never have been administered to patients in the higher, more dangerous dosage levels. In the article linked above you can watch my interview with Dr. Vladimir Zelenko.
Zelenko garnered national attention in early 2020 when he told radio host Sean Hannity that he had nearly 100% success treating COVID-19 patients with hydroxychloroquine, azithromycin and zinc sulfate for five days. However, like others who could document success using treatment methods other than vaccines and standard antivirals, his social media platforms were censored, and he was recently removed from Twitter.
As of that interview, he had treated more than 3,000 patients with COVID-19-related symptoms. One third of them received the triple drug regimen as the remaining were in a low-risk category and did not need drug treatment. Of the 3,000, 15 were hospitalized and only three high-risk patients died.
In a patient cohort of 3,000 people, 1,000 of whom received the triple treatment regimen, the mortality rate was 0.3%. The push against hydroxychloroquine is described by Zelenko as a “psychological operation” to scare people away from the drug. He is appalled, saying in this transcript of his interview:43
“This is a genocide against the elderly and infirm, it's a mass murder and a crime against humanity. There are plenty of people who have blood on their hands, including the media. It’s unbelievable the crime that's been done on the human psyche. I'm screaming to humanity: Don't be scared! Be cautious. Be smart. Use common sense. But don't be scared.”
Vir: https://articles.mercola.com/sites/articles/archive/2021/05/05/human-prescription-ivermectin.aspx
https://trialsitenews.com/when-nothing-else-works-judges-are-siding-with-ivermectin/?utm_source=Contextly&utm_medium=ChannelEmail&utm_campaign=Ivermectin&utm_content=Popular%2BTrending
*
Ivermectin is widely used by physicians, as there are now 51 studies from around the world, with 50 showing clear benefit and one showing neutral. However, the lone study showing a neutral effect was roundly criticized as flawed in an open letter signed by a group of 120 physicians.
Vir: https://trialsitenews.com/open-letter-by-u-s-doctors-jama-ivermectin-study-is-fatally-flawed/
*
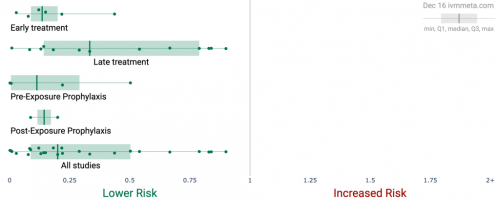
Review of the Emerging Evidence Demonstrating the Efficacy of Ivermectin in the Prophylaxis and Treatment of COVID-19
Kory, Pierre MD1,*; Meduri, Gianfranco Umberto MD2; Varon, Joseph MD3; Iglesias, Jose DO4; Marik, Paul E. MD5
Author InformationAmerican Journal of Therapeutics: May Jun 2021 - Volume 28 - Issue 3 - p e299-e318Abstract
Background:
After COVID-19 emerged on U.S shores, providers began reviewing the emerging basic science, translational, and clinical data to identify potentially effective treatment options. In addition, a multitude of both novel and repurposed therapeutic agents were used empirically and studied within clinical trials.
Areas of Uncertainty:
The majority of trialed agents have failed to provide reproducible, definitive proof of efficacy in reducing the mortality of COVID-19 with the exception of corticosteroids in moderate to severe disease. Recently, evidence has emerged that the oral antiparasitic agent ivermectin exhibits numerous antiviral and anti-inflammatory mechanisms with trial results reporting significant outcome benefits. Given some have not passed peer review, several expert groups including Unitaid/World Health Organization have undertaken a systematic global effort to contact all active trial investigators to rapidly gather the data needed to grade and perform meta-analyses.
Data Sources:
Data were sourced from published peer-reviewed studies, manuscripts posted to preprint servers, expert meta-analyses, and numerous epidemiological analyses of regions with ivermectin distribution campaigns.
Therapeutic Advances:
A large majority of randomized and observational controlled trials of ivermectin are reporting repeated, large magnitude improvements in clinical outcomes. Numerous prophylaxis trials demonstrate that regular ivermectin use leads to large reductions in transmission. Multiple, large “natural experiments” occurred in regions that initiated “ivermectin distribution” campaigns followed by tight, reproducible, temporally associated decreases in case counts and case fatality rates compared with nearby regions without such campaigns.
Conclusions:
Meta-analyses based on 18 randomized controlled treatment trials of ivermectin in COVID-19 have found large, statistically significant reductions in mortality, time to clinical recovery, and time to viral clearance. Furthermore, results from numerous controlled prophylaxis trials report significantly reduced risks of contracting COVID-19 with the regular use of ivermectin. Finally, the many examples of ivermectin distribution campaigns leading to rapid population-wide decreases in morbidity and mortality indicate that an oral agent effective in all phases of COVID-19 has been identified.
INTRODUCTION
In early 2020, on the onset of the spreading pandemic, many providers and institutions began to continuously review the rapidly emerging basic science, translational, and clinical data to identify potentially effective treatment options for COVID-19. Although there is now a small and increasing number of therapeutics showing some efficacy in important clinical outcomes, chief of which are corticosteroids in moderate to severe illness, the world continues to suffer from a worsening crisis with the potential of again overwhelming hospitals and intensive care units (ICU). As of February 21, 2020, the number of deaths attributed to COVID-19 in the United States reached 510,248 with more than 9.3 million active cases, the highest number to date. In addition, multiple European countries have imposed new rounds of restrictions and lockdowns.
Further compounding these alarming developments was a wave of recently published results from therapeutic randomized controlled trials conducted on medicines believed effective for COVID-19 that found a lack of impact on mortality in hospitalized patients with the use of remdesivir, hydroxychloroquine, lopinavir/ritonavir, interferon, convalescent plasma, and monoclonal antibody therapy.1–4 One year into the pandemic, the only therapy considered “proven” as a life-saving treatment in COVID-19 is the use of corticosteroids in patients with moderate to severe illness.5,6 Similarly, most concerning is the fact that no agent has yet proven effective in outpatients to prevent disease progression to prevent hospitalization.
More recently, trial results of ivermectin, a widely used antiparasitic medicine with known antiviral and anti-inflammatory properties, have been showing benefits in multiple important clinical and virologic outcomes, including mortality. Although growing numbers of the studies supporting this conclusion have passed through peer review, approximately half of the remaining trials data are from manuscripts uploaded to medical preprint servers, a now standard practice for both rapid dissemination and adoption of new therapeutics throughout the pandemic. Following is a comprehensive review of the available efficacy data as of December 12, 2020, taken from in vitro, animal, clinical, and real-world studies all showing the above impacts of ivermectin in COVID-19.
History of ivermectin
In 1975, Professor Satoshi Omura at the Kitsato institute in Japan isolated an unusual Streptomyces bacterium from the soil near a golf course along the southeast coast of Honshu, Japan. Omura, along with William Campbell, found that the bacterial culture could cure mice infected with the roundworm Heligmosomoides polygyrus. Campbell isolated the active compounds from the bacterial culture, naming them “avermectins” and the bacterium S. avermitilis for the compounds' ability to clear mice of worms.7 Despite decades of searching around the world, the Japanese microorganism remains the only source of avermectin ever found. Ivermectin, a derivative of avermectin, then proved revolutionary. Originally introduced as a veterinary drug, it soon made historic impacts in human health, improving the nutrition, general health, and well-being of billions of people worldwide ever since it was first used to treat onchocerciasis (river blindness) in humans in 1988. It proved ideal in many ways, given that it was highly effective, broad-spectrum, safe, well tolerated, and could be easily administered.7 Although it was used to treat a variety of internal nematode infections, it was most known as the essential mainstay of 2 global disease elimination campaigns that has nearly eliminated the world of two of its most disfiguring and devastating diseases. The unprecedented partnership between Merck & Co. Inc, and the Kitasato Institute combined with the aid of international health care organizations has been recognized by many experts as one of the greatest medical accomplishments of the 20th century. One example was the decision by Merck & Co to donate ivermectin doses to support the Mectizan Donation Program that then provided more than 570 million treatments in its first 20 years alone.8 Ivermectin's impacts in controlling onchocerciasis and lymphatic filariasis, diseases which blighted the lives of billions of the poor and disadvantaged throughout the tropics, is why its discoverers were awarded the Nobel Prize in Medicine in 2015 and the reason for its inclusion on the World Health Organization's (WHO) “List of Essential Medicines.” Furthermore, it has also been used to successfully overcome several other human diseases and new uses for it are continually being found.7
Preclinical studies of Ivermectin's activity against SARS-CoV-2
Since 2012, a growing number of cellular studies have demonstrated that ivermectin has antiviral properties against an increasing number of RNA viruses, including influenza, Zika, HIV, Dengue, and most importantly, SARS-CoV-2.9–17 Insights into the mechanisms of action by which ivermectin both interferes with the entrance and replication of SARS-CoV-2 within human cells are mounting. Caly et al18 first reported that ivermectin significantly inhibits SARS-CoV-2 replication in a cell culture model, observing the near absence of all viral material 48 hours after exposure to ivermectin. However, some questioned whether this observation is generalizable clinically given the inability to achieve similar tissue concentrations used in their experimental model using standard or even massive doses of ivermectin.19,20 It should be noted that the concentrations required for an effect in cell culture models bear little resemblance to human physiology given the absence of an active immune system working synergistically with a therapeutic agent, such as ivermectin. Furthermore, prolonged durations of exposure to a drug likely would require a fraction of the dosing in short-term cell model exposure. Furthermore, multiple coexisting or alternate mechanisms of action likely explain the clinical effects observed, such as the competitive binding of ivermectin with the host receptor-binding region of SARS-CoV-2 spike protein, as proposed in 6 molecular modeling studies.21–26 In 4 of the studies, ivermectin was identified as having the highest or among the highest of binding affinities to spike protein S1 binding domains of SARS-CoV-2 among hundreds of molecules collectively examined, with ivermectin not being the particular focus of study in 4 of these studies.27 This is the same mechanism by which viral antibodies, in particular, those generated by the Pfizer and Moderna vaccines contain the SARS-CoV-2 virus. The high binding activity of ivermectin to the SARS-CoV-2 spike protein could limit binding to either the ACE-2 receptor or sialic acid receptors, respectively, either preventing cellular entry of the virus or preventing hemagglutination, a recently proposed pathologic mechanism in COVID-19.21,22,26–28 Ivermectin has also been shown to bind to or interfere with multiple essential structural and nonstructural proteins required by the virus to replicate.26,29 Finally, ivermectin also binds to the SARS-CoV-2 RNA-dependent RNA polymerase (RdRp), thereby inhibiting viral replication.30
Arevalo et al investigated in a murine model infected with a type 2 family RNA coronavirus similar to SARS-CoV-2, (mouse hepatitis virus), the response to 500 μg/kg of ivermectin versus placebo.31 The study included 40 infected mice, with 20 treated with ivermectin, 20 with phosphate-buffered saline, and then 16 uninfected control mice that were also given phosphate-buffered saline. At day 5, all the mice were killed to obtain tissues for examination and viral load assessment. The 20 nonivermectin-treated infected mice all showed severe hepatocellular necrosis surrounded by a severe lymphoplasmacytic inflammatory infiltration associated with a high hepatic viral load (52,158), whereas in the ivermectin-treated mice a much lower viral load was measured (23,192; P < 0.05), with only few livers in the ivermectin-treated mice showing histopathological damage such that the differences between the livers from the uninfected control mice were not statistically significant.
Dias De Melo et al32 recently posted the results of a study they did with golden hamsters that were intranasally inoculated with SARS-CoV-2 virus, and at the time of the infection, the animals also received a single subcutaneous injection of ivermectin at a dose of 0.4 mg/kg on day 1. Control animals received only the physiologic solution. They found the following among the ivermectin-treated hamsters: a dramatic reduction in anosmia (33.3% vs. 83.3%, P = 0.03), which was also sex dependent in that the male hamsters exhibited a reduction in clinical score while the treated female hamsters failed to show any sign of anosmia. They also found significant reductions in cytokine concentrations in the nasal turbinates and lungs of the treated animals, despite the lack of apparent differences in viral titers.
Despite these mounting insights into the existing and potential mechanisms of action of ivermectin both as a prophylactic and treatment agent, it must be emphasized that significant research gaps remain and that many further in vitro and animal studies should be undertaken to better define not only these mechanisms but also to further support ivermectin's role as a prophylactic agent, especially in the optimal dose and frequency required.
Preclinical studies of ivermectin's anti-inflammatory properties
Given that little viral replication occurs in the later phases of COVID-19, nor can virus be cultured, and only in a minority of autopsies can viral cytopathic changes be found,33–35 the most likely pathophysiologic mechanism is that identified by Li et al36 where they showed that the nonviable RNA fragments of SARS-CoV-2 lead to a high mortality and morbidity in COVID-19 through the provocation of an overwhelming and injurious inflammatory response. Based on these insights and the clinical benefits of ivermectin in the late phase of disease to be reviewed below, it seems that the increasingly well-described in vitro properties of ivermectin as an inhibitor of inflammation are far more clinically potent than previously recognized. The growing list of studies demonstrating the anti-inflammatory properties of ivermectin include its ability to inhibit cytokine production after lipopolysaccharide exposure, downregulate transcription of NF-kB, and limit the production of both nitric oxide and prostaglandin E2.37–39
Exposure prophylaxis studies of ivermectin's ability to prevent transmission of COVID-19
Data are also now available showing large and statistically significant decreases in the transmission of COVID-19 among human subjects based on data from 3 randomized controlled trials (RCTs) and 5 observational controlled trials (OCTs) with 4 of the 8 (2 of them RCTs) published in peer-reviewed journals.40–46
Elgazzar and colleagues45 at Benha University in Egypt randomized 200 health care and household contacts of patients with COVID-19 where the intervention group consisted of 100 patients given a high dose of 0.4 mg/kg on day 1 and a second dose on day 7 in addition to wearing personal protective equipment, whereas the control group of 100 contacts wore personal protective equipment alone. They reported a large and statistically significant reduction in contacts testing positive by Reverse Transcriptase Polymerase Chain Reaction (PCR) when treated with ivermectin versus controls, 2% versus 10%, P < 0.05.
Shouman conducted an RCT at Zagazig University in Egypt, including 340 (228 treated and 112 control) family members of patients positive for SARS-CoV-2 through PCR.44 Ivermectin (approximately 0.25 mg/kg) was administered twice, on the day of the positive test and 72 hours later. After a two-week follow-up, a large and statistically significant decrease in COVID-19 symptoms among household members treated with ivermectin was found, 7.4% versus 58.4%, P < 0.001.
Recently, Alam et al from Bangladesh performed a prospective observational study of 118 patients who were evenly split into those who volunteered for either the treatment or control arms, described as a persuasive approach. Although this method, along with the study being unblinded, likely led to confounders, the difference between the 2 groups was so large (6.7% vs. 73.3%, P <0.001) and similar to the other prophylaxis trial results that confounders alone are unlikely to explain such a result.47 Carvallo et al also performed a prospective observational trial where they gave healthy volunteers ivermectin and carrageenan daily for 28 days and matched them to similarly healthy controls who did not take the medicines.40 Of the 229 study subjects, 131 were treated with 0.2 mg of ivermectin drops taken by mouth 5 times per day. After 28 days, none of those receiving ivermectin in the prophylaxis group had tested positive for SARS-COV-2 versus 11.2% of patients in the control arm (P < 0.001). In a much larger follow-up prospective, observational controlled trial by the same group that included 1195 health care workers, they found that over a 3-month period there were no infections recorded among the 788 workers who took weekly ivermectin prophylaxis, whereas 58% of the 407 controls had become ill with COVID-19. This study demonstrates that remarkable protection against transmission can be achieved among high-risk health care workers by taking 12 mg once weekly.40 The Carvallo IVERCAR protocol was also separately tested in a prospective RCT by the Health Ministry of Tucuman, Argentina, where they found that among 234 health care workers, the intervention group that took 12 mg once weekly, only 3.4% contracted COVID-19 versus 21.4% of controls, P < .0001.46
The need for weekly dosing in the Carvallo study over a 4-month period may not have been necessary given that, in a recent RCT from Dhaka, Bangladesh, the intervention group (n = 58) took 12 mg once monthly for a similar 4-month period and also reported a large and statistically significant decrease in infections compared with controls, 6.9% versus 73.3%, P < 0.05.47 Then, in a large retrospective observational case–control study from India, Behera et al41 reported that among 186 case–control pairs (n = 372) of health care workers, they identified 169 participants who had taken some form of prophylaxis, with 115 participants that had taken ivermectin. After matched pair analysis, they reported that in the workers who had taken 2 dose ivermectin prophylaxis, the odds ratio for contracting COVID-19 was markedly decreased (0.27, 95% confidence interval (CI) 0.15–0.51). Notably, one dose prophylaxis was not found to be protective in this study. Based on both their study finding and the Egyptian prophylaxis study, the All India Institute of Medical Sciences instituted a prophylaxis protocol for their health care workers where they now take two 0.3 mg/kg doses of ivermectin 72 hours apart and repeat the dose monthly.
Data that further illuminates the potential protective role of ivermectin against COVID-19 come from a study of nursing home residents in France which reported that in a facility that suffered a scabies outbreak where all 69 residents and 52 staff were treated with ivermectin,41 they found that during the period surrounding this event, 7 of the 69 residents fell ill with COVID-19 (10.1%). In this group with an average age of 90 years, only one resident required oxygen support and no resident died. In a matched control group of residents from surrounding facilities, they found 22.6% of residents fell ill and 4.9% died.
Further evidence supporting the efficacy of ivermectin as a prophylaxis agent was published recently in the International Journal of Antimicrobial agents where a group of researchers analyzed data using the prophylactic chemotherapy databank administered by the WHO along with case counts obtained by Worldometers, a public data aggregation site used by among others, the Johns Hopkins University.42 When they compared the data from countries with active ivermectin mass drug administration programs for the prevention of parasite infections, they discovered that the COVID-19 case counts were significantly lower in the countries with recently active programs, to a high degree of statistical significance, P < 0.001.
Figure 1 presents a meta-analysis performed by the study authors of the controlled ivermectin prophylaxis trials in COVID-19.
CELA ŠTUDIJA: https://covid19criticalcare.com/wp-content/uploads/2020/11/FLCCC-Ivermectin-in-the-prophylaxis-and-treatment-of-COVID-19.pdf
*
The evidence base for ivermectin against COVID-19
To date, the efficacy of ivermectin in COVID-19 has been supported by the following:
- Since 2012, multiple in vitro studies have demonstrated that Ivermectin inhibits the replication of many viruses, including influenza, Zika, Dengue, and others.9–17
- Ivermectin inhibits SARS-CoV-2 replication and binding to host tissue through several observed and proposed mechanisms.18
- Ivermectin has potent anti-inflammatory properties with in vitro data demonstrating profound inhibition of both cytokine production and transcription of nuclear factor-κB (NF-κB), the most potent mediator of inflammation.37–39
- Ivermectin significantly diminishes viral load and protects against organ damage in multiple animal models when infected with SARS-CoV-2 or similar coronaviruses.31,32
- Ivermectin prevents transmission and development of COVID-19 disease in those exposed to infected patients.40–45
- Ivermectin hastens recovery and prevents deterioration in patients with mild to moderate disease treated early after symptoms.45,49–52,61,62
- Ivermectin hastens recovery and avoidance of ICU admission and death in hospitalized patients.45,51,53,63–66
- Ivermectin reduces mortality in critically ill patients with COVID-19.45,53,63
- Ivermectin leads to temporally associated reductions in case fatality rates in regions after ivermectin distribution campaigns.48
- The safety, availability, and cost of ivermectin are nearly unparalleled given its low incidence of important drug interactions along with only mild and rare side effects observed in almost 40 years of use and billions of doses administered.75
- The World Health Organization has long included ivermectin on its “List of Essential Medicines.”
A summary of the statistically significant results from the above controlled trials are as follows:
Controlled trials in the prophylaxis of COVID-19 (8 studies)
- All 8 available controlled trial results show statistically significant reductions in transmission.
- Three RCTs with large statistically significant reductions in transmission rates, N = 774 patients.44–46
- Five OCTs with large statistically significant reductions in transmission rates, N = 2052 patients.40–43,47
Controlled trials in the treatment of COVID-19 (19 studies)
https://www.webmd.com/lung/news/20210506/covid-patient-in-coma-gets-ivermectin-after-court-order
May 6, 2021 -- A 68-year-old woman with COVID-19, who has been in intensive care in an Illinois hospital for a month, started receiving the controversial drug ivermectin (Stromectol) this week after her family sued the hospital to have someone administer it, according to a report in the Chicago Tribune.
Nurije Fype's daughter, Desareta, filed suit against Elmhurst Hospital, part of Edward-Elmhurst Health, asking that her mother receive the treatment, which is approved as an anti-parasite drug but not approved for the treatment of COVID-19. Desareta Fype has been granted temporary guardianship of her mother.
The FDA has warned against ivermectin's use for treating COVID-19, but a high-profile group of doctors has spoken passionately in favor of it.
The FDA has published guidance titled ,"Why You Should Not Use Ivermectin to Treat or Prevent COVID-19" on its website. The National Institutes of Health said there is not enough data to recommend either for or against its use in treating COVID-19.
On Friday, DuPage County Judge James Orel ruled Fype should be allowed to get the treatment.
Three days later, according to the Daily Herald, the lawyer for the hospital, Joseph Monahan, argued the hospital could not find a hospital-affiliated doctor to administer the ivermectin.
The Herald reported the judge told the hospital to "get out of the way" and allow any board-certified doctor to administer the drug.
When Fype's doctor was unable to administer it, the legal team found another doctor, Alan Bain, DO, to do it. Monahan said Bain was granted credentials to work at the hospital so he could administer it Monday evening.
In a follow-up hearing on Tuesday, Monahan told Orel that the hospital asked 20 doctors and 19 other health care workers, including nurses and pharmacists, to administer the medication and they all declined, the Herald reported.
Orel denied a request from Desareta Fype's lawyer to order the hospital's nurses to administer further doses. The judge also denied a request to hold the hospital in contempt of court.
According to the Herald, the judge said at the hearing Tuesday, "Now let's hope the good Lord allows the medication to work."
The hospital did not respond to Medscape's request for comment on the legal case or the patient's condition by publication time.
According to NBC5 Chicago, Desareta said Tuesday, "She looks calm, comfortable, and I'm happy with her monitor numbers so far. They are kind of stable."
Fype's daughter said her mother has been a patient at Elmhurst Hospital since April 7, was put on a ventilator on April 28, and is now in a coma.
According to the Daily Herald, Desareta Fype said in court documents that she is willing to release the hospital from liability if the drug harms her mother.
The Daily Herald also reports that Fype's attorneys cited arguments by the Front Line COVID Critical Care Alliance that ivermectin has antiviral and anti-inflammatory benefits that help people infected with COVID-19.
Ivermectin is an anthelmintic used mainly to treat roundworms, threadworms, and other parasites.
Ivermectin is one of the WHO’s “essential drugs” which all countries should have access to. It’s very cheap as its patent has long expired; it’s one of the most-used drugs in world history; it’s extraordinarily safe; it is often life-saving against parasitic infections. It is also one of the best-established pharmaceutical treatments for COVID-19, showing benefit in every stage of the disease, in multiple independent clinical trials of varying quality. On January 3, 2021, Dr. Tess Lawrie attempted to alert the Prime Minister to the potential of Ivermectin. Her video here was pulled from YouTube within hours of posting, though it survives on Vimeo. The paper by the FLCCC group of U.S. intensivists (whose survival rates for severe COVID-19 are best in class) that was the inspiration for Dr. Lawrie’s work was accepted after extensive open peer review (including two career employees of the FDA) and “provisionally accepted” by the “open science” journal Frontiers in Pharmacology. The screenshot of the abstract tweeted by Clare Craig shown here attracted more than 100,000 views. Then, mysteriously, it was rejected and pulled by the Frontiers editor in chief. It is still here in cached form though the Ministry of Truth has been at work and placed it in a memory hole, so no trace survives on Frontiers’ own website.
Intended for a Special Issue on “repurposed drugs” for COVID-19, various guest editors were so incensed at this behaviour that they resigned in protest. You can read their letter here. They concluded that “these unfortunate events constitute gross editorial misconduct by Frontiers.” Fortunately this major paper is now published by the American Journal of Therapeutics and can be read in its final form here.
This nevertheless successfully delayed by nearly six months its circulation to leading public health bodies starting mid-November. A copy was sent to Sir Jeremy Farrar (boss of the Wellcome Trust and member of Sage) who passed it on to Professor Peter Horby (also on Sage), amongst others, on November 18, 2020. So the efficacy of Ivermectin must be well known to the Government’s advisers, but they have done nothing about it. Likewise, the formal and rigorous meta-analysis performed by Dr. Tess Lawrie’s team at the Evidence-Based Medicine Consultancy Ltd has been communicated to Matt Hancock, but without reply.
I am telling you about this, because all that governments, their scientific advisers, Big Pharma (here’s Merck, who originally developed & marketed it) and regulatory agencies will tell you is that Ivermectin doesn’t work in COVID-19. They are lying. I am inviting any of them to sue me, but they won’t, for I would win easily. If Ivermectin was more widely used, there’d be no need for vaccines.
https://www.lifesitenews.com/opinion/former-pfizer-vp-why-are-we-being-lied-to-about-covid-theres-no-good-reason
*
https://www.biznews.com/thought-leaders/2021/05/12/mailbox-ivermectin?fbclid=IwAR0Wt2wMa_Ktgl_qvuHxFIOQpBvtHfSIBCM-sTlepQLb_pfUm7suK92vbRE
*
*
*
Komentar na indijsko študijo o profilaktični uporabi Ivermectina.
Ivermektin je registriran kot antiparazitik, ob tem pa ima dve pomembni dodatni lastnosti: močno zavira vezavo virusov na celice, deluje pa tudi močno protivnetno. Njegovo protivirusno delovanje je pomembno pri preprečevanju in zgodnjem zdravljenju okužbe s sars-cov-2, protivnetno delovanje pa ublaži hudo vnetno dogajanje pri napredovali bolezni, imenovano tudi citokinska nevihta, ki privede do vnetja pljuč in dihalne stiske.
Pri osebah z visokim tveganjem za okužbo, torej pri negovalnem osebju okuženih ali pri članih njihovega gospodinjstva, en odmerek ivermektina na teden za 88 odstotkov zmanjša verjetnost okužbe. Pri okuženih osebah ivermektin za 53 odstotkov zmanjša verjetnost poslabšanja bolezni, skrajša obdobje simptomov in tudi obdobje kužnosti. Najpomembnejši podatek iz metaanalize randomiziranih študij pa je smrtnost pri ivermektinu v primerjavi s kontrolno skupino. Po podatkih, ki jih je zbrala dr. Lawrie, so imeli pri ivermektinu med skupaj 585 bolniki osem primerov smrti, med 522 bolniki v kontrolnih skupinah pa 44 umrlih. Metaanaliza je torej pokazala, da ivermektin za 83 odstotkov znižuje odstotek umrlih (p < 0,01, interval zaupanja 65–92 %).
Za protivirusno delovanje je bila v laboratorijskih raziskavah potrebna sorazmerno visoka koncentracija ivermektina, kakršne pri zdravljenju ne moremo doseči. Očitno pa to zdravilo v živem organizmu deluje drugače. V nobeni od študij zdravljenja bolnikov s covidom-19 niso uporabili visokih odmerkov zdravila, ko bi resnično lahko pričakovali več stranskih učinkov. V mednarodni raziskavi, v kateri so zbrali izkušnje zdravljenja pri več kot 50.000 bolnikih s parazitskimi okužbami, so resne zaplete zdravljenja zabeležili pri manj kot enem odstotku bolnikov, in to skoraj izključno pri tistih z očesno obliko filariaze in s porušeno krvno-možgansko pregrado. V priporočenih odmerkih je torej ivermektin zelo varno zdravilo.
Težave pri objavah
Za ivermektin pri covidu-19 so doslej zaključili 20 randomiziranih študij. Le šest študij je že dočakalo objavo v recenziranih medicinskih revijah, za ostale že zaključene študije pa so rezultati dostopni le na nekaterih spletnih straneh, ki prinašajo tudi še neobjavljena poročila. Pri tem avtorji kar 13 od 14 neobjavljenih študij poročajo o ugodnejšem poteku bolezni pri skupini bolnikov, ki je prejemala ivermektin.
Spodbude »negativni« študiji
V prvih dneh marca je bila v ugledni reviji Jama objavljena študija iz Kolumbije, ki so jo nasprotniki ivermektina brž izpostavili kot dokaz, da to zdravilo pri zdravljenju bolnikov s koronavirusom ni učinkovito. Pozorno branje pa razkrije, na kako trhlih nogah je to zanikanje.
Eno od osnovnih pravil kliničnega raziskovanja je, da novih zdravil ne preskušamo pri dveh skupinah bolnikov: pri umirajočih, ki jim razumljivo prav nič ne more pomagati, in pri bolnikih z blago obliko bolezni, ki bodo ozdraveli, ne glede na to, kako jih zdravimo. Verjetno so imeli tudi sponzorji besedo pri tem, da so kolumbijski raziskovalci v svojo raziskavo vključili bolnike z blago obliko bolezni, mnoge že v obdobju okrevanja. Srednja starost bolnikov v študiji je bila 37 let, vsi so bili ambulantni, velika večina je bila brez spremljajočih bolezni, od potrjene okužbe pa je minilo že 5–7 dni. Tako ni presenetljivo, da so le pri dveh odstotkih bolnikov v skupini z ivermektinom oziroma pri štirih odstotkih bolnikov v skupini s placebom ugotovili poslabšanje bolezni. Ker so številke nizke, razlika ni statistično značilna. Kolumbijska študija ni »negativna«, temveč ima za potrditev tako majhne razlike premajhno napovedno moč. Kljub temu da študija ne pove nič novega in ne prispeva k razjasnitvi dileme, ali je ivermektin učinkovit pri bolnikih s covidom-19, so jo s pomočjo sponzorjev – farmacevtskih podjetij – objavili v ugledni reviji.
Ob robu te, s strani nasprotnikov ivermektina tako cenjene študije še majhna pripomba. Pri obeh skupinah, torej ivermektinu in placebu, so zabeležili povsem enak odstotek glavobolov, vrtoglavice, slabosti, diareje, torej simptomov, ki bi lahko kazali na sopojave zdravljenja. Raziskovalci sami zaključujejo, da so omenjeni simptomi posledica okužbe z virusom in da zdravljenje z ivermektinom nima pomembnih stranskih učinkov.
Primeri cenzure in pristranska mnenja regulatornih agencij
Dr. Pierre Kory je metaanalizo poslal v objavo v revijo Frontiers in Pharmacology. Po ugodnem mnenju recenzentov mu je 13. januarja 2021 urednik sporočil: »Čestitam. Članek je sprejet v objavo.« Šest tednov kasneje mu je isti urednik brez dodatnega pojasnila sporočil, da je članek zavrnjen. Zelo podobno je bilo odločanje pri članku, ki ga je v Lancet – Respiratory Disease poslala dr. Lavrie: ugodno mnenje štirih recenzentov, nato pa odločitev uredništva, da članka ne objavijo.
O ugotovitvah glede učinkovitosti ivermektina je dr. Kory 8. decembra 2020 poročal članom odbora ameriškega senata. Posnetek njegovega pričevanja si je na youtubu v naslednjih tednih ogledalo več kot osem milijonov ljudi. V začetku februarja 2021 so ta posnetek z youtuba odstranili z utemeljitvijo, da je »zavajajoč in nevaren«.
Svetovna zdravstvena organizacija (WHO) je dr. Andrewu Hillu naročila, naj pripravi analizo zdravljenja covida-19 z ivermektinom. Hill je metaanalizo izdelal, poslal na WHO in poročilo objavil na youtubu. WHO poročila na svoji spletni strani ni objavila, v sredini februarja pa je bil izbrisan tudi posnetek na youtubu.
Omenimo še navedke s spletnih strani vplivnih regulatornih agencij. »FDA ni odobrila ivermektina za preventivo ali zdravljenje covida-19. Jemanje zdravila za neodobren namen je lahko zelo nevarno.« (Food and Drug Administration, ZDA). »Na osnovi dosedanjih dokazov ne moremo priporočiti uporabe ivermektina za preprečevanje ali zdravljenje covida-19. Da bi v pljučih dosegli koncentracijo, ki zavira virus, bi bili potrebni visoki odmerki zdravila, pri tem pa ne moremo izključiti resnih sopojavov.« (EMA – European Medicines Agency). »Premalo podatkov je, da bi priporočili ali odsvetovali uporabo ivermektina za zdravljenje covida-19. Potrebujemo dokaze dobro načrtovanih in izpeljanih kliničnih študij.« (NIH, National Institutes of Health).
Kdo je v ozadju?
Vse kaže, da gre za aktivno nasprotovanje širjenju informacije, da ivermektin lahko odigra pomembno vlogo pri preprečevanju okužbe in pri zdravljenju covida-19. Aktivno oviranje objav v strokovnih revijah, cenzura preglednih člankov kljub naklonjenemu mnenju recenzentov, blokada informacij na youtubu, nenaklonjenost regulatornih agencij in aktivna promocija sicer slabo izpeljane, domnevno negativne študije – vse to napeljuje na zaključek, da ivermektinu preprosto ne sme uspeti.
Seveda bi bilo naivno pričakovati, da bomo lahko predstavili konkretnega krivca za takšen odnos. Vprašamo pa se lahko, komu ni v interesu, da se pri preprečevanju in zdravljenju covida-19 uveljavi ceneno generično zdravilo. Vprašamo se lahko, kako daleč sega vpliv farmacevtske industrije, ki si ne želi konkurence novim, bistveno dražjim zdravilom. Medicinske strokovne revije, mednarodna strokovna srečanja, pa tudi regulatorne agencije in celo Svetovna zdravstvena organizacija – vsi z veseljem sprejemajo donacije. Veliko je znanega tudi o lastniških povezavah med farmacevtsko industrijo ter tiskanimi in elektronskimi mediji. Od tu do pristranosti pri uredniški politiki ali pri oblikovanju strokovnih priporočil pa ni daleč.
In vendar se premika
Ivermektin počasi, a nezadržno prihaja tudi v Evropo. Severna Makedonija, Slovaška in Češka so ivermektin že uvrstile med zdravila z začasnim dovoljenjem za zdravljenje covida-19. Dr. Michal Rezek, primarij I. interne kardioangiološke klinike bolnišnice Sv. Ana v Brnu, ivermektin uporablja že od lanskega novembra in je z rezultati zelo zadovoljen. Najnovejšo pošiljko je bolnišnica pridobila iz Bolgarije s pomočjo premiera Babiša, piše iROZHLAS.cz, strežnik javnega Češkega radia. »Gre za premajhno število (30) pacientov, da bi lahko naredili celovite zaključke. Vendar je bila toleranca zdravljenja zelo dobra, nezaželeni učinki pa minimalni, zdravstveno stanje velike večine pacientov se je po jemanju ivermektina toliko izboljšalo, da so lahko bili odpuščeni v domačo oskrbo,« je dejal primarij Rezek za Češko tiskovno agencijo (prevod Peter Kuhar).
Slovenski infektologi ivermektinu (še) niso naklonjeni. Tega jim ne gre zameriti: razumeti moramo, da so že dvanajst mesecev pod neverjetnim bremenom vsakodnevnega dela s hudo bolnimi in da se zato pri izbiri zdravljenja opirajo na mednarodne smernice. Pri tem žal ne upoštevajo, da na te smernice lahko vplivajo komercialni interesi in da želja po zaslužku ni vedno v skladu z interesi bolnikov in interesi celotne družbe, ki ječi pod družbenim in socialnim bremenom epidemije.
Izsledkov opazovalnih in randomiziranih kliničnih študij preprosto ne moremo več spregledati. Prišel je čas, da pokažemo svojo pokončnost. Vsi dokazi so, da lahko ivermektin za hospitalizirane bolnike zniža smrtnost. Pri ambulantnih bolnikih to zdravilo zniža verjetnost za zaplete in skrajša obdobje kužnosti, kar z epidemiološkega stališča pomeni manjši reprodukcijski faktor prenosa okužbe. Pomembno znižanje okuženih lahko pričakujemo tudi, če bi sprejeli ivermektin kot profilaktično terapijo za osebe z visokim tveganjem za okužbo. Dve možnosti imamo: ali tem opažanjem verjamemo in ivermektin sprejmemo v nabor zdravil proti okužbi z virusom sars-cov-2 ali pa zaključimo, da dokazi niso dovolj prepričljivi, in zastavimo svojo, slovensko randomizirano klinično študijo. Bolnikov je (žal) dovolj. V nekaj mesecih lahko sebi in Evropi ponudimo jasen odgovor na vprašanje, ali je to pot iz primeža pandemije.
Naj končam, kjer sem začel: cepljenje in ivermektin se medsebojno ne izključujeta. Potrebujemo zaščito pred okužbo in potrebujemo učinkovito zdravljenje. Ko bo to spoznanje prodrlo tudi pri nas, bo koronavirus izginil s prve in predzadnje strani časopisa.
https://www.delo.si/sobotna-priloga/prepovedano-zdravilo/?fbclid=IwAR0551ZwdIJE-FTo3gLh6R45CkjsNswHDCWq-4q5Oe4ZjpxW4gUp_14KcLo
*
Conclusions:
Meta-analyses based on 18 randomized controlled treatment trials of ivermectin in COVID-19 have found large, statistically significant reductions in mortality, time to clinical recovery, and time to viral clearance. Furthermore, results from numerous controlled prophylaxis trials report significantly reduced risks of contracting COVID-19 with the regular use of ivermectin. Finally, the many examples of ivermectin distribution campaigns leading to rapid population-wide decreases in morbidity and mortality indicate that an oral agent effective in all phases of COVID-19 has been identified.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8088823/
*
*
https://trialsitenews.com/south-valley-university-in-egypts-clinical-trial-reveals-ivermectin-based-nasal-spray-improves-covid-19-outcomes/?utm_source=Contextly&utm_medium=ChannelEmail&utm_campaign=Ivermectin&utm_content=Notification
*
*
*
Sve opasne bolesti najbolje je liječiti rano. Glavni neuspjeh naše strategije protiv COVIDA-19 bio je što se čekalo tjedan dana da bolest postane opasna, kada disanje postane problem. Rano liječenje COVIDA-19, čak i za one s blagim simptomima, sprječava kasniju hospitalizaciju. Postoji nekoliko lijekova za rano liječenje koji obećavaju, ali ivermektin prednjači u pogledu sigurnosti, učinkovitosti i cijene. Nažalost, najveći igrači zapadnih mainstream medija članovi su Trusted News Initiative (TNI). TNI je priča za neku drugu prigodu, ali vrijedno pažnje je to što su veliki mediji jedva izvijestili da su se njegovi članovi dogovorili za promicanje globalnog cijepljenja i da se svaki “dezinformacijski mit zaustavi”. Nažalost, čini se da se na rano liječenje gleda kao na dezinformacijski mit i samim tim se ne spominje. Rano liječenje je vitalno po pitanju tretiranja opasnih bolesti, a COVID-19 nije iznimka.
Uzimajući u obzir ljudske i ekonomske troškove, ovo izbjegavanje ranog liječenja vrlo sigurnim, učinkovitim i nepatentiranim lijekom je kriminalna tragedija ogromnih razmjera i dobitni listić lutrije za neke farmaceutske tvrtke koje dizajniraju i prodaju nove patentirane lijekove koji se inače ne bi mogli natjecati s ivermektinom na slobodnom tržištu. Merck traži odobrenje za hitnu uporabu (EUA) za svoj terapijski molnupiravir, stoga će „Merck dobiti približno 1,2 milijarde dolara za isporuku približno 1,7 milijuna doza molnupiravira vladi Sjedinjenih Država. “ Ivermektinu nije potreban EUA jer je prošao ispitivanja 1986. godine. Samo ga treba preporučiti za liječenje COVIDA-19, ali ako bi službeno bio priznat kao učinkovit tretman, to bi pravno spriječilo molnupiravir da dobije odobrenje za hitnu uporabu dok ne prođe ispitivanja i samim tim bi bio usporen posao vrijedan 1,2 milijarde dolara.
Svjetska zdravstvena organizacija, kao najveća globalna i neprofitna zdravstvena organizacija, donosi odluke koje drugi slijede, vjerujući da je ta organizacija bez komercijalnih interesa. Izvorno financirana u potpunosti od država članica, organizacija sada od njih prima manje od 20% svog proračuna, dok ostatak prima od donatora koji imaju svoje specifične financijske i strateške interese. Margret Chan, bivša generalna direktorica SZO-a, rekla je 2015. godine, “Moram uzeti šešir i ići po cijelom svijetu moliti za novac, a kad nam ga daju, jako je vezan za njihove ciljeve i ono što oni žele. To nisu prioriteti i želje SZO-a, pa ako to ne riješimo, nećemo biti sjajni kao što smo bili ”.
Novinarski veteran Robert Parsons objašnjava da su „program iskorjenjivanja malih boginja u cijelosti financirali donatori koji su možda doveli do problema, da se za posebne projekte moraju prikupiti sredstva, ali privatni sektor se vjerojatno neće uključiti ako ne vidi profit … posljedično tome, malo je neovisnih istraživanja javnog zdravstva”. Od tada je neprikladni financijski utjecaj privatnih dionika u SZO-u porastao. Donacije dolaze s upozorenjima pa je organizacija kompromitirana zbog brojnih pitanja koja uključuju interese donatora.
Na primjer, 2010. godine, nakon pandemije gripe H1N1, istražni upit British Medical Journala (BMJ) i Ureda za istraživačko novinarstvo utvrdio je da su ključni znanstvenici koji stoje iza preporuke Svjetske zdravstvene organizacije o pravljenju zaliha lijekova za pandemijsku gripu, imali financijske veze s tvrtkama koje su profitirale.” Ti su savjetnici uspjeli uvjeriti vladu Velike Britanije da potroši milijarde na cjepivo koje nikada nije bilo potrebno.
Gurajući cijepljenje na globalni dnevni red od 2012., Bill Gates je oživio i izvukao iz neuspjeha industriju cjepiva. Snaga novca Zaklade Gates diktirala je prelazak na cijepljenje, a ne na liječenje. Gates vjeruje da je kapitalizam učinkovitiji od javnih zdravstvenih usluga u poboljšanju zdravlja ljudi i bez sumnje, svoja ulaganja u nekoliko farmaceutskih tvrtki, uključujući Merck, Pfizer, Johnson & Johnson, vidi kao etička ulaganja, čineći tako svijet boljim mjestom. Kapitalizam je obično učinkovitiji od vlade, ali zato profit uvijek vrednuje iznad ljudi. Morgan Stanley vjeruje da bi Pfizer u sljedećih pet godina mogao zaraditi 100 milijardi dolara od cjepiva.
Zaklada Gates drugi je najveći donator SZO-a nakon SAD-a. Gates je, međutim, također osnovao i financira Globalni savez za cjepiva i imunizaciju (GAVI) i Globalni fond. U 2018/19., njihov je zajednički doprinos bio 27% veći od doprinosa SAD-a, što je Gatesov utjecaj učinio moćnijim od bilo koje vlade. Kako su sredstva namijenjena određenim projektima, SZO ne odlučuje na koji će se način potrošiti novac fondacije, već to čini Gates. Prioriteti Gatesaa postali su SZO-ovi, a taj je prioritet globalno cijepljenje protiv COVIDA-19, a ne sustavi javnog zdravstva koji pružaju rano liječenje. Tedros Adhanom, trenutni generalni direktor SZO-a, prethodno je radio za Gatesa dok je bio član odbora GAVI i predsjedavajući Globalnog fonda. Vrlo vjerojatno je da na njega još uvijek utječu ideologija i financijska moć njegovih prethodnih poslodavaca.
U smjernicama SZO za ivermektin, pokazano je smanjenje smrtnosti za 80%, ali s “niskom sigurnošću”, i opet, što je zbunjujuće, ne preporučuje se njegova upotreba. Dokument smjernica SZO-a „zasnovan je na sustavnom pregledu i mrežnoj meta-analizi istražitelja sa Sveučilišta McMaster”. Sveučilište McMaster (uključujući i sve njegove izravne podružnice) trebalo se isključiti iz provođenja smjernica, budući da ima nekoliko objektivnih sukoba interesa kada je u pitanju ivermektin.
McMaster dizajnira i proizvodi drugu generaciju cjepiva COVID-19. Vjerojatno će ljudi oklijevati uzeti cjepivo ako postoji održiva mogućnost sigurnog profilaktičkog liječenja i liječenja za COVID-19. Kao drugo, Sveučilište McMaster prima milijunska sredstva od Zaklade Gates koja se ulažu u tržišno vođene tvrtke, čiji bi se neki proizvodi natjecali s ivermektinom na slobodnom tržištu, s tim da je ivermektin vrlo jeftin. Uz to, McMaster ne samo da prima milijunske iznose od zaklade Gates, već imaju dijelom i zajedničmo osoblje, poput Edwarda Millsa, izvanrednog profesora McMastera i savjetnika za klinička ispitivanja zaklade Gates. Edward Mills glavni je istražitelj ispitivanja „Zajedno za procjenu ivermektina“ (Together trial evaluating Ivermectin).
Mills, u intervjuu za McMasters 2020. godine kaže: “Brzo nam ponestaje mogućnosti za prenamijenjene lijekove, tako da moramo isprobati nove.” Možda je tako, ali s obzirom da Gates posjeduje zalihe nekoliko glavnih cjepiva i konkurentske proizvođače lijekova, postoji očit sukob interesa.
U nedavnom intervjuu, činilo se da Mills umanjuje učinak ivermektina. Mills iznenađujuće tvrdi da profilaksa, kod koje podaci jasno pokazuju da je ivermektin najučinkovitiji, “nije uvjerljiva”. Ako postoji jedno područje u kojem je ivermektin posebno učinkovit, to je kao profilaktičko sredstvo. Bilo je nekoliko studija koje pokazuju da je važan vremenski raspored profilaktičke doze. Pokus Carvallo na 1200 zdravstvenih radnika koji su u direktnom kontaktu sa oboljelima, utvrdio je da je 12 mg ivermektina tjedno rezultiralo s nula slučajeva u odnosu na 58% pozitivnih slučajeva u kontrolnoj skupini, tijekom deset tjedana. Možete pokus rastaviti na najmanje dijelove, ali na kraju uvijek ostajete s izvanrednim rezultatom koji je dodatno ojačan studijom AIIMS na 3500 bolničkih radnika koji su koristili istu dozu, ali samo dva puta mjesečno, i koja je pokazala smanjenje slučajeva za 74% , ali, eto, Edward Mills ne nalazi zanimljivim dokaze o profilaksi. Veliki novac nije u vođenju ispitivanja generički prenamijenjenih lijekova, već u ispitivanjima farmaceutskih tvrtki koje se bore za tržišni udio.
SZO nije smio prihvatiti sudjelovanje McMastersa u izradi smjernica niti sudjelovanje u ispitivanju ivermektina zbog njihovog sukoba interesa. Vjerujem da SZO nije naručio analizu koju su koristili u svojim trenutnim smjernicama, već im je to ponudila Gatesova fondacija, jer tako očito sada funkcionira SZO. SZO sada čeka rezultate ispitivanja „Zajedno za procjenu ivermektina“ koju financira Gates kako bi iznijela svoje mišljenje o Ivermectinu. Što bi moglo poći po zlu?
Na pitanja poslana etičkom uredu SZO-a, tražeći jasnoću u vezi s njegovom preporukom protiv upotrebe ivermektina, odgovoreno je na ovaj način: odbijeno je davanje zapisnika sa sastanka, naglašeno je da glasanje nije bilo potrebno, takođe nijedan intervju neće biti odobren, kao i da oni „uopće ne razmatraju procjenu i dopuštenje ivermektina za profilaktičku uporabu za COVID-19″, da nije bilo uključeno osoblje iz farmaceutske tvrtke, da oni ne smatraju da su ispitivanja od farmaceutskih tvrtki “pristrana zbog financijskog interesa”, a pored svega navedenog u njihovoj je prepisci bila i prijeteća klauzula o povjerljivosti .
Meta-analiza SZO pokazala je da je ivermektin imao tri puta više štetnih učinaka. Doktorica Tess Lawrie, autorica časopisa „Medicinsko savjetovanje zasnovano na dokazima“ (Evidence-Based Medicine Consultancy Ltd), kaže da je „procjena učinka ozbiljno i izuzetno neprecizna i netočna“. Stoga ono što pokazuju dokazi SZO-a jest da ne postoji jasna razlika u ozbiljnim neželjenim događajima između ljudi koji su dobili ivermektin i onih koji nisu. Također, pokazuje da je u meta-analizi bilo vrlo malo događaja – oni ne izvještavaju koliko je događaja, ali može biti ukupno oko 7 za ivermektin i kontrolne skupine kombinirano. Tim za smjernice od SZO-a i McMasters-a, neprimjereno je protumačio ovo otkriće rekavši da “ivermektin može povećati rizik nastajanja ozbiljnih štetnih posljedica”. Svatko u SZO-u tko je uključen u razvoj smjernica mogao bi vam to reći.”
Glavna znanstvenica SZO-a, dr. Soumya Swaminathan, nedavno je na Twitteru upozorila indijske državljane da ne uzimaju ivermektin, pozivajući se na Merckov marketinški materijal. Indijska odvjetnička komora uručila je pravnu obavijest dr. Swaminathan zbog širenja dezinformacija i uzrokovanja mnogih smrtnih slučajeva. Tweet je nakon toga izbrisan.
Nekada plemenita ideja o globalnom javnom zdravstvenom sustavu koji radi u našem najboljem interesu je, umjesto toga, postala nešto čime upravlja privatni financijski interes. Ako neće donijeti profit, malo je vjerojatno da će se lijek ili liječenje testirati u velikom i skupom ispitivanju. Proizvođači lijekova uvjerili su SZO da su prihvatljiva samo skupa ispitivanja, pa se samo njihovi lijekovi, uz financijsku potporu, testiraju prema tom standardu. Pa ipak, dobro prihvaćeno, “ivermektin ne djeluje” ispitivanje Lopez-Media koje su financirali proizvođači cjepiva i koje je imalo nekoliko izuzetno ozbiljnih problema, usprkos svim tim problemima je bilo jedino ispitivanje ivermektina koje je prihvatila JAMA.
Svjetska zdravstvena organizacija je financijski uvjerena da su jedina ispitivanja koja vrijedi pogledati ona koja si mogu priuštiti ulagači. Kao što su pokazala ispitivanja o raku koja su financirale duhanske kompanije, pokuse s ivermektinom uopće ne bi trebao raditi netko tko ima financijski i ideološki sukob interesa u ulaganju u cjepiva. SZO ne bi smio zasnivati svoje mišljenje o ivermektinu na ispitivanjima koja je provodila zaklada Gates. GAVI odnedavno prikazuje Google oglase “zašto se ivermektin ne preporučuje”. Rano liječenje znanstvena je prijetnja industriji globalnog cijepljenja.
SZO mora dokazati da slijedi znanstveni i etički postupak u svojoj preporuci protiv upotrebe ivermektina. Povjerenje javnosti presudno je za pobjedu protiv pandemije. Zapisnik sa sastanka, na kojem je uzeta preporuka protiv ivermektina, mora se objaviti. Bez toga, preporuka ostaje zagađena sumnjom u prekomjerno miješanje korporacija. Treba nam reći i pokazati račune onih koji su platili studiju McMaster zbog koje je SZO dao preporuku protiv ivermektina kao i bilo kakav sukob interesa.
Ispitivanje „Zajedno za procjenu ivermektina“ zahtijeva javne provjere i neovisan nadzor. Ne možemo dopustiti da SZO prihvati još jedno ispitivanje koje diktira globalnu zdravstvenu politiku kao “zlatni standard”, a da nam se ne daju odgovori na pitanja i ne ispitaju komercijalni i ideološki sukobi donatora.
Brojna randomizirana kontrolirana ispitivanja dokazala su učinkovitost ivermektina i potvrdila njegovu sigurnost. Potrebna su nam ispitivanja ivermektina o dozama koje treba primjenjivati, u različitim stadijima bolesti, uključujući i preventivu. Morali bismo ga početi odmah koristiti.
Preuzeto sa: https://trialsitenews.com/conflict-of-interest-in-who-recommendation-against-ivermectin/
*
https://ivermektin.si/ivermektin-clanki.php
*
*
https://www.conservativewoman.co.uk/the-anti-covid-pill-big-pharma-doesnt-want-you-to-have/
*
https://taibbi.substack.com/p/why-has-ivermectin-become-a-dirty-7bd
https://www.youtube.com/watch?v=yOAh7GtvcOs&t=2s -Ivermectin meta-analysis by Dr. Andrew Hill
*
Predavanje prof. Christiana Perronneja, ki dokaže znanstvene prevare, ki so poskušale diskreditirati učinkovitost hidroksiklorokina, klorakina in azintromicina kot zdravil pri protokolu zdravljenja bolezni današnje dobe.
https://www.bitchute.com/video/Qy73Lp4aLxOY/
*
https://www.facebook.com/gerard.rennick/videos/407279220507389/
Avstralija: Professor Robert Clancy backs ivermectin as a COVID-19 treatment
*
https://trialsitenews.com/ivercovid19-study-in-argentina-disappoints-study-underdoses-ivermectin-comes-up-short/?fbclid=IwAR26J2GHQpP0h0cbY-4aMfaMz2Qavt62dYghTNtThJkdYowbKqgg2-RlTwE
*

Ivermektin je antiparazitsko zdravilo, ki se preučuje za ponovno uporabo proti SARS-CoV-2. Ivermektin je pri visokih koncentracijah pokazal delovanje in vitro proti SARS-COV-2. V tej metaanalizi je bil ivermektin preučen v 24 randomiziranih kliničnih preskušanjih (3328 bolnikov), opredeljenih s sistematičnim iskanjem v PUBMED, EMBASE, MedRxiv in registrih preskušanj. Ivermektin je bil povezan z zmanjšanjem vnetnih markerjev (C-reaktivni protein, d-dimer in feritin) in hitrejšim odstranjevanjem virusa s PCR. Virusni izloček je bil odvisen od odmerka in trajanja zdravljenja. V 11 randomiziranih študijah zmerne/težke okužbe se je umrljivost zmanjšala za 56 % (relativno tveganje 0,44 [95%CI 0,25-0,77]; p=0,004; 35/1064 (3 %) smrti pri ivermektinu; 93/1063 (9 %) smrti v kontrolnih skupinah) z ugodnim kliničnim okrevanjem in manjšim številom hospitalizacij. Številne vključene študije niso bile strokovno pregledane, ocenjen pa je bil širok razpon odmerkov. SZO trenutno priporoča uporabo ivermektina le znotraj kliničnih študij. V pripravi je mreža obsežnih kliničnih raziskav, ki naj bi potrdila dosedanje rezultate.
Povzetek študije julij 2021: https://academic.oup.com/ofid/advance-article/doi/10.1093/ofid/ofab358/6316214?fbclid=IwAR3xj6EnfqbJIv1K4wjbA5CjB920pRH2Fcf8ExmjZbFVJdazAvZCXONWEJA
*
https://dokumentarac.hr/ivermektin/video-ivermektin-cenzurirana-istina-koja-je-mogla-spasiti-zivote/
*
*
*
https://ivmmeta.com/?fbclid=IwAR3x5Vv2of3OD4Od-8u3C8JQduWT-SPNf2cG_v0Vhrxmem6l-yQKo4Qvs6I
*
*
*
https://www.youtube.com/watch?v=lPiVgvKIEqw
O Ivermectinu
*
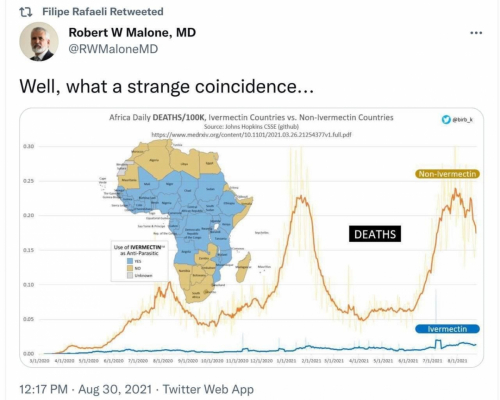
Poglejmo, kaj o njem pravi prof. Zwitter v intervjuju, ki ga je z njim opravila Darja Lovšin in je bil objavljen v reviji Dita (Dita, let. 24, št. 4, avgust 2021, str. 8, 9): »To je staro, zelo preizkušeno zdravilo, ki je imelo odločilno vlogo pri obvladovanju številnih parazitskih bolezni, razširjenih v tretjem svetu.«
Je eno od osnovnih zdravil tudi na spisku Svetovne zdravstvene organizacije, a je žal registrirano samo za zdravljenje parazitskih bolezni. Do spoznanja, da izjemno koristi tudi pri premagovanju okužbe s SARS-CoV2, je prišlo po naključju. Od tedaj pa je bilo opravljenih že veliko zanesljivih kliničnih študij, ki pa so vse pokazale, da ivermektin zmanjša verjetnost okužbe za skoraj 90%, skrajšuje obdobje kužnosti, znižuje odstotek hospitalizacij in za več kot 80% zmanjša smrtnost.
Prof. Zwitter si zelo prizadeva za uveljavitev uporabe ivermektina pri reševanju trenutne zdravstvene krize. Pripravil je osnutek protokola klinične študije, ki bi bodisi potrdila ali ovrgla trditve o koristnosti tega zdravila tudi pri zdravljenju bolezni covid-19. Pravi pa, da je sam ne more izpeljati in bi pri tem potreboval pomoč infektologov, virologov, imunologov, epidemiologov in drugih strokovnjakov. »Takšna študija bi stala toliko, kot en dan zaprtja družbe. Problem je v glavah, v nenavadnem prepričanju, da smo premajhni in da je edina pot, da capljamo za velikimi. Problem je, da nam usodo krojijo ljudje, ki ne premorejo niti odstotka odločenosti in samozavesti, kakršni kaže na primer Tadej Pogačar«, pravi prof. Zwitter.
Pereče je dejstvo, da je Lekarniška zbornica Slovenije vsem lekarnam poslala dopis, s katerim odsvetuje uporabo ivermektina za zdravljenje bolnikov, okuženih s koronavirusom. Kaj je infektologe napeljalo k tako odločnemu zavračanju nadvse preizkušenega in varnega zdravila, ni jasno. Jasno pa je, da bi pravočasna uporaba ivermektina ne samo v Sloveniji, temveč po vsem svetu, peljala potek pandemije v povsem drugo smer. Ni dvoma, da bi se ta že zdavnaj končala in to z neprimerno manj človeškimi žrtvami.
Poraja se nam (retorično) vprašanje, ali je morda tako zagnano in nerazumno zavračanje varnega, preizkušenega in poceni zdravila, kakorkoli povezano s prizadevanji nekaterih farmacevtskih gigantov (izstopa Pfizer), ki obljubljajo že v kratkem, nekako do konca letošnjega leta, razviti svoje zdravilo proti koronavirusu (Dnevnik, 20. 8. 2021, str. 4). Brez kančka dvoma lahko trdimo, da bo cena tega zdravila neprimerno višja od cene ivermektina.
Veliko koristnih in zanimivih informacij o Ivermektinu lahko najdete na spletni strani www.ivermektin.si
Ivermectin: a multifaceted drug of Nobel prize-honoured distinction with indicated efficacy against a new global scourge, COVID-19
*
https://www.embopress.org/doi/full/10.15252/emmm.202114122
*
https://pubmed.ncbi.nlm.nih.gov/34466270/
Ivermectin: a multifaceted drug of Nobel prize-honoured distinction with indicated efficacy against a new global scourge, COVID-19
Povzetek
Leta 2015 je Nobelov odbor za fiziologijo ali medicino s svojo edino nagrado za zdravljenje nalezljivih bolezni po šestih desetletjih počastil odkritje ivermektina (IVM), vsestranskega zdravila, ki se uporablja proti nekaterim najbolj uničujočim tropskim boleznim na svetu.
Od marca 2020, ko je bil IVM prvič uporabljen proti novi svetovni nadlogi, COVID-19, je več kot 20 randomiziranih kliničnih preskušanj (RCT) spremljalo takšno bolnišnično in ambulantno zdravljenje. Šest od sedmih metaanaliz RCT zdravljenja z IVM, o katerih so poročali leta 2021, je pokazalo opazno zmanjšanje smrtnosti zaradi COVID-19, s povprečnim 31-odstotnim relativnim tveganjem smrtnosti v primerjavi s kontrolnimi raziskavami.
Med množičnim zdravljenjem IVM v Peruju se je v desetih perujskih provincah z najobsežnejšim zdravljenjem v 30 dneh v povprečju za 74 % zmanjšala prekomerna smrtnost. Zmanjšanje števila smrtnih primerov je bilo povezano z obsegom razporeditve IVM v vseh 25 provincah s p < 0,002.
Močno zmanjšanje obolevnosti z uporabo IVM je bilo opaženo tudi pri dveh živalskih modelih, s SARS-CoV-2 in sorodnem betakoronavirusu. Navedeni biološki mehanizem IVM, kompetitivna vezava na proteinsko bodico SARS-CoV-2, verjetno ni specifičen za epitope, kar bi lahko omogočilo popolno učinkovitost proti nastajajočim mutiranim virusnim sevom.
*
*
*
*
Invermectin v Indiji
*
Program zdravljenja z Ivermectinom v Afriki: https://www.youtube.com/watch?v=wMfmho9K9hU
*
*
Izkušnje aregentinskih zdravnikov z Ivermectinom: https://media.mercola.com/ImageServer/Public/2021/October/PDF/argentinian-doctor-shares-his-ivermectin-experience-pdf.pdf
*
Generalni državni tožilec Doug Peterson je izdal pravno mnenje, da lahko izvajalci zdravstvenega varstva v Nebraski zakonito predpišejo ivermektin in hidroksiklorokin za zdravljenje s COVIDOM, dokler pacienta pridobijo obveščeno soglasje."
*
Darja Lovšin, urednica revije DITA in predstavnica angleške organizacije BIRD na TV Exodus o Ivermectinu:
https://www.exodus.si/oddaje/na-robu-znanega-zdravilo-ivermectin-in-sedanja-kriza
*
Dokument o Ivermectinu (48 strani): https://dokumentarac.hr/wp-content/uploads/2021/10/21-017_0-HRVATSKI-finale.pdf
*
https://www.logicno.com/politika/tajni-dokumenti-otkrivaju-napad-fda-na-ivermektin.html
*
Odvetnica Dipali Ojha iz indijske odvetniške zbornice in skupina mladih indijskih odvetnikov so Svetovni zdravstveni organizaciji (SZO) poslali pravni opomin zaradi očitne kampanje proti alternativnim načinom zdravljenja.
Do pravnega ukrepa proti SZO je prišlo po tvitu Soumye Swaminathana, glavne znanstvenice SZO, ki je objavila tvit proti ivermektinu in ga podkrepila s povezavo, ki jo je objavilo zasebno podjetje.
Ekipa indijskih odvetnikov si prizadeva, da bi bile množicam na voljo vse možne cenovno dostopne možnosti in da bi najvišji organi odgovarjali za svoje direktive in sum, da so podlegli lobiranju velikih farmacevtskih podjetij.
https://www.facebook.com/watch/?v=1032112187523253
*
Attempt to discredit landmark British ivermectin study
*
https://c19ivermectin.com/?fbclid=IwAR2zOAReD7euUReLV_lLcQLFqozVAgvlqBbcSI7ovLEANSi4scsdFZrBik0
Darija Lovšin Fb 2.11. 2021
*
https://trialsitenews.com/fdas-smoking-gun-disinformation-campaign-targeting-ivermectin/
*
https://odysee.com/@FrontlineCovid19CriticalCareAlliance:c/DrPierreKoryCovidSummit:4
Dr. Pierre Kory: Florida Summit on COVID 11/6/2021
*
https://dokumentarac.hr/featured/preokret-lijecnici-mogu-prepisivati-ivermektin-i-hidroksiklorokin-odlucio-drzavni-odvjetnik-nebraske-sad-opsirno-obrazlozenje/?fbclid=IwAR3aQRsFfSZboRV_40bk_C1oQdR5a55IUfw1pWpscZzOQyrZe8il0YopM-Q
*
*
*
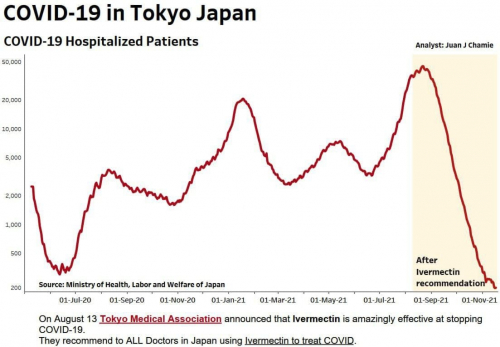
Vir: Dr Pierre Kory
*
Članek dr. Matjaža Zwitra o Ivermectinu v reviji ISIS, april 2021: http://online.pubhtml5.com/agha/lkug/?fbclid=IwAR2SSSyag6nn0mtlq6S4_Gy_vbLSpbS7S6TovUWW0jUWPWE0Rd6PDw3QrOo#p=39
*
Saturacija krvi s kisikom se je v 2 urah po prejemu Ivermectina dvignila iz 65 na 85:
*
Bojan Erjavšek FB 26.11. 2021
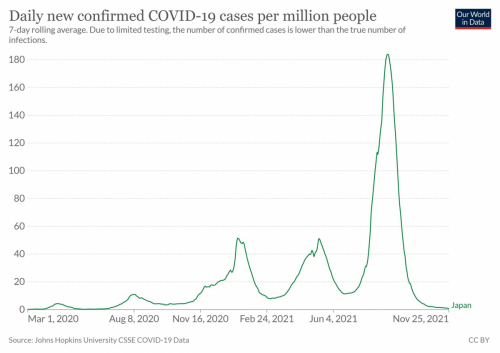
*
Protokol zdravljenja z Ivermectinom- Madagaskar: http://www.spentamexico.org/v15-n2/A0.15(2)1-18en.pdf?fbclid=IwAR3XJvyLoTdoRWZfLA2ytP0mfoN1wd-frSpxSVJUL6v6OTIrTZ5e4dCzYWs
*
A massive pre-print study released in December showed that low preventive dosages of ivermectin, taken every two weeks, reduced mortality by 68%. This apparent good news was not welcomed by Twitter, which immediately moved to censor the paper, slapping it with a “Misleading” warning label without explanation.
*
*
Študija o Ivermectinu na 223128 ljudeh v Braziliji
Zaščita, ki jo zagotavlja ivermektin pri preventivni uporabi za COVID-19, se je morda odrazila v zmanjšanju stopnje hospitalizacije in umrljivosti zaradi COVID-19, opaženem na ravni populacije. V primerjavi s stanjem pred začetkom programa sta se stopnji hospitalizacij in umrljivosti zaradi COVID-19 zmanjšali za 73 % oziroma 59 % (p < 0,0001 za obe). Do teh zmanjšanj je prišlo, če smo upoštevali celotno populacijo ter število primerov COVID-19, hospitalizacij in smrti v mestu Itajaí, ne glede na odstotek bolnikov, ki so preventivno uporabljali ivermektin. Pred začetkom programa in med njim ni bilo sprememb v različicah SARS-CoV-2, nalezljivosti in patogenosti.
*
Jan 07, 2021
