



90% Američanov, ki so bili pozitivni na PCR testu ni prenašalo okužbe s koronavirusi SARS CoV-2 niti s katerim koli drugim virusom
https://www.nytimes.com/2020/08/29/health/coronavirus-testing.html
https://publishwall.si/narava.zdravi/post/560910/who-in-kitajska-studija-zdrave-osebe-zelo-redko-prenasajo-okuzbe-s-koronavirusi-sars-cov-2
*
Slovenski zdravniki: recenzijsko poročilo o napakah v PCR testu
https://slovenskizdravniki.si/corman-drosten-recenzijsko-porocilo/
* * *
Portuguese Appeals Court Deems PCR tests unreliable
*
Študija je pokazala, da je PCR test nad 33 ciklusi neuporaben. V večini držav delajo več kot 33 ciklusov
https://www.facebook.com/frankdatank915/videos/367450191152077
Študija: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7185831/
*
Celovita analiza o zmoti PCR testiranja v Veliki Britaniji
https://lockdownsceptics.org/pcr-based-covid-testing-has-failed-us/
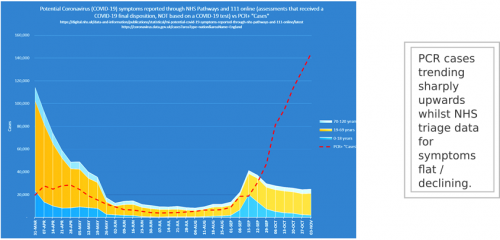
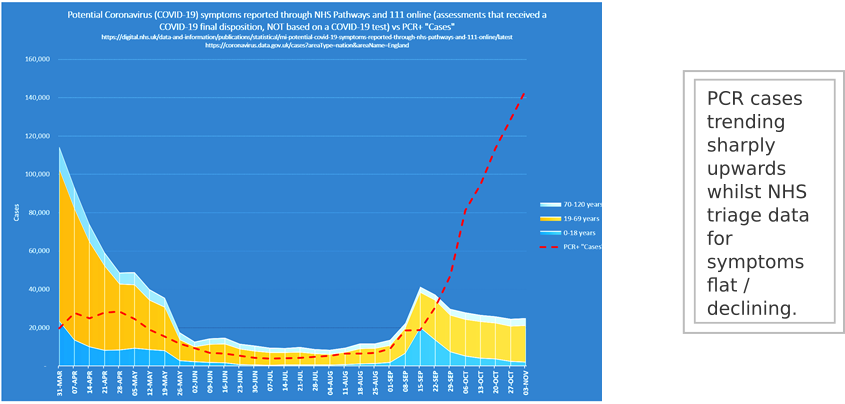
Med tem ko imamo epidemijo lažno pozitivnih PCR testov (rdeča), število primerov COVID-19 s simptomi pada- podatki za Veliko Britanijo od 31.3. do 1.11. 2020
*
Zmedo s PCR testi nazorno pokaže dr. filozofije Ivan Pajovič
(zelo smešno, a žal resnično)
https://www.facebook.com/100004357814821/videos/1777481115740465
*
Izumitelj PCR testa, biokemik Kary Mullis pravi: ni primeren za diagnosticiranje okužbe z virusi
https://www.mojvideo.com/video-kaj-je-povedal-kary-mullis-o-pcr-testih-lekcija-tudi-za-covid19-slovenski-podnapisi/d349f996f5f439d866a1
Kery Mullis, dobitnik Nobelove nagrade za kemijo in izumitelj PCR testa:
Vprašanje: Ali je možna zloraba PCR za oceno t.i prostih virusnih RNK, ki morda niso tam?
Mullis: Mislim da beseda »zloraba« ni primerna, ne morete zlorabiti PCR testa, ampak rezultate oz tolmačenje rezultatov. Če rečejo, da so našli virus v vas, pa dejansko s PCR testom lahko najdete karkoli pri vsakem človeku. To je v skladu z budističnim naukom, da je vse v vsem. Če lahko pomnožite eno samo molekulo do količine, ki jo lahko merite, kar PCR test lahko naredi, potem obstaja zelo malo vrst molekul, ki jih vi nimate v svojem telesu - vsaj ene izmed njih. Napačna uporaba testa je torej v trditvi, da je to pomenljivo. Je zelo malo tega, kar imenujejo HIV, o čemur govori R. Philpot. Meritev zanj ni natančna, virusov ni mogoče prešteti tako kot jabolka. Jabolko je jabolko, lahko pa dobite nekaj, kar je podobno jabolku in ko to sestavite skupaj, je videti kot jabolko. In tako je s HIV virusi. Test temelji na dejstvu da so nevidni in rezultati so informativni. PCR test je proces, ki se uporabi, da iz majhne količine naredite veliko. Ne pove vam, da ste bolni, niti da boste na koncu prizadeti s tem.
https://www.facebook.com/mojca.hanzekovic/videos/5098828680142875
*
* * *
Nemški doktor prava Reiner Fuellmich o ničvrednosti PCR testa
V zvezi z nadvse pomembnimi PCR testi citiram, kar Yeadon piše v članku, objavljenem 20.9. 2020 z naslovom Laži, preklete laži in zdravstvena statistika (Lies, Damned Lies and Health Statistics), smrtonosna nevarnost lažno pozitivnih rezultatov:
"Verjetnost, da je navidezno pozitiven test lažno pozitiven primer, je med 89-94%, kar je blizu gotovosti."
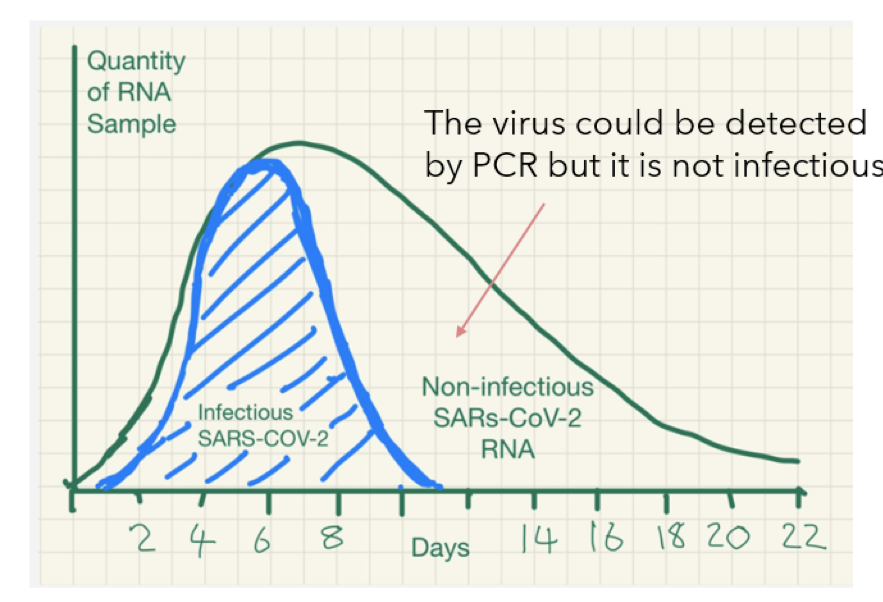
Dr. Yeadon, v dogovoru s profesorji imunologije, dr. Camero iz Nemčije, prof.dr. Pierre Capel-om iz Nizozemske in prof. dr. Dolores Cahill iz Irske ter mikrobiologom dr. Arve iz Avstrije, ki so vsi pričali pred nemškim odborom za korono, izrecno poudarja, da pozitiven test ne pomeni, da je bil najden celoten (angl. intact - nepoškodan ali funkcionalen) virus. Avtorji pojasnjujejo, da kar PCR test dejansko meri, je (citiram):
"....preprosto prisotnost delnih sekvenc RNA, navzočih v nepoškodovanem virusu, ki bi lahko bili deli mrtvega virusa, ki ne morejo povzročiti obolenja v subjektu, ki se ne prenašajo na druge osebe in ne morejo povzročiti bolezni pri nobeni drugi osebi...."
Zaradi popolne neprimernosti testa za ugotavljanje infektivnih bolezni, je bil ta test pozitiven pri kozah, ovcah, papajah in celo piščančjih perutnicah. Oksfordski profesor in epidemiolog Carl Heneghan, direktor Centra za z dokazi utemeljeno medicino (Centre for Evidence - Based Medicine) piše, da COVID-19 virus ne bi nikoli izginil, če bi se ta praksa testiranja nadaljevala, saj bi ga vedno lažno zaznavali v večini tega, kar testirajo.
Namen CLASS ACTION tožbe je, da se pokliče na sodno odgovornost in obremeni z odškodnino vse tiste, ki so evidentno postavljali napačne trditve. To je predvsem Drosten (ki je prilagodil PCR test za koronavirus), ki je očitno po ukazu na začetku leta nenadoma spremenil mnenje. Bilo je že vse pripravljeno, saj je znano, da je napisal dokument v EUROSURVEILLANCE. Nenadoma pa je spremenil mnenje, predvidevamo, da je dobil ukaz in tako izjavil, da je korona nevarna, podobno, kot je to že poskušal pred 12 leti pri svinjski gripi, kar pa se mu je zahvaljujoč delu dr. Wodarga izjalovilo. Drosten je tudi takoj predstavil rešitev, namreč PCR test, ki ga je sam sestavil in bi naj bil primeren za ugotavljanje okužb. WHO je test sprejel in ga na priporočilo Tedrosa predlagal po vsem svetu kot primernega za ugotavljanje okužb. Tako so PCR test seveda tudi tržili. Mislim, da so prvi testi prišli iz laboratorija TIP MOLBIOL, od dolgoletnega, bom previdno formuliral- poslovnega partnerja od Drostna, nato pa so jih začeli na veliko prodajati po vsem svetu. Ker so jih prodajali tudi v Kanadi in Ameriki, drugje pa so jih kopirali, gre v tem primeru za tako imenovano stvarno pristojnost sodišč. Kar pa lahko storimo, je da lahko tožbo vloži kanadsko ali ameriško podjetje (te dve deželi prideta v poštev, ker je pri njih možna CLASS ACTION tožba), ki je bilo oškodovano zaradi lockdown-a, ki je spet temeljil edino na PCR testih. Potrebno je napasti PCR teste, saj je to srž vsega, saj vsega ostalega ni več glede na to, da vemo, da korona po nevarnosti ustreza gripi in glede na to, da je tudi ameriški CDC (Center za obvladovanje bolezni in preventive) ugotovil, da sploh še nimamo izoliranega virusa, tako da se vprašamo, kaj sploh zdravimo. Tako ostane PCR test samo še kot sredstvo za vzbujanje strahu. PCR test z trditvijo, da se z njim lahko ugotovi infekcijo. Dr. Reiner Füellmich 24.10.2020
* * *
Doc dr. Tatjana Lejko Zupanc, klinika za infekcijske bolezni:
Pozitiven PCR test ne pomeni, da je oseba kužna. Lahko gre za neko staro okužbo.
https://www.facebook.com/vizualneresitve.zavrsek.7/videos/170386721302004
* * *
Članica slovenskega kriznega štaba: Tretji val bo zagoneten, ker ko se bo pojavil bolnik, ne bomo vedeli ali ima COVID-19 ali gripo
(od minute 2.45-3.00) https://www.facebook.com/watch/?v=2818293655117403¬if_id=1604345921550872¬if_t=watch_follower_video&ref=notif
V čem je potem pomen PCT testa, če ne loči med gripo in SARS CoV-2 ?
*
*
*
*
*
* * *
Vse več je napačnih Corona - PCR testov
Slučaj v kliniki na Bavarskem: od 60 pozitivnih testov jih je po kontroli 58 le negativnih – šefica navaja razloge
Von Klaus Rimpel
Vsa Bavarska se bori proti Coroni. Kaj pa, če je naš edini pokazatelj, PCR test, naenkrat zmotljiv? Obsežne napake pri testiranju v eni od klinik na Bavarskem nam dajo misliti.
-
Die Corona-Zahlen in Bayern steigen stetig - Jedoch wird auch wesentlich mehr getestet als im Frühjahr 2020.
-
Številke o coroni na Bavarsken so v stalnem porastu. Toda, testirajo tudi bistveno več kot so pomladi 2020.
-
Napačni rezultati testiranja pri nekaj bavarskih klinikah nam glede zanesljivosti zastavljajo vprašanja.
-
V Taufkirchnu so bili za 60 najprej pozitivno testiranih rezultati za 58 oseb napačni.
- https://www.merkur.de/bayern/corona-test-bayern-panne-ergebnisse-isar-amper-klinik-taufkirchen-pcr-test-zr-90082728.html
- * * *
Ali glede na to lahko verjamemo, kar o PCR testu pravi stroka?
PCR- oz. molekularno testiranje
Temelji na tehnologiji verižne reakcije s polimerazo (angl. polymerase chain reaction – PCR).
Posamezniku vzamejo bris iz nosnega dela žrela, nato pa ga v laboratoriju testirajo in majhne količine genskega materiala (dednine) v vzorcu (npr. RNK-virusa v brisu nosu) pomnožujejo do zaznavnih količin. Logika PCR-preiskave je, da majhnih količin dednine virusa v vzorcu ne moremo zaznati, po pomnoževanju do velikih količin pa to lahko.
Gre za zelo občutljive in zelo specifične teste, kar pomeni, da zaznajo izredno majhne količine virusa in zelo dobro razlikujejo med novim koronavirusom in starimi koronavirusi, ki so tudi v populaciji. Tudi ti testi niso 100-odstotno zanesljivi, a so najboljše, kar je trenutno na voljo, je nedavno za STA pojasnila vodja oddelka za mikrobiološke raziskave v Nacionalnem laboratoriju za zdravje, okolje in hrano (NLZOH) Maja Rupnik.
Teorija 1. Pozitiven rezultat na testu PCR ne pomeni bolezni!
Molekularni test, pozitiven za SARS-CoV-2, res ne pomeni enako kot bolezen.
Nikoli ne moremo govoriti o bolezni, če imamo samo pozitiven rezultata testiranja.
O bolezni govorimo, ko se pojavijo bolezenski simptomi/znaki. V primeru pozitivnega testa brez bolezenskih znakov/ simptomov pa govorimo o asimptomatski okužbi ali pa o nosilstvu. Npr.: veliko ljudi ima v žrelu bakterijo Streptococcus pyogenes brez znakov bolezni, ker jo telo tolerira. Ko nosilci to bakterijo prenesejo na dovzetno osebo, bo ta zbolela za angino. Podobno je lahko tudi pri novem koronavirusu. Pri pozitivnem SARS-CoV-2 testu v odsotnosti simptomov govorimo o bodisi predsimptomatski (=pred simptomi) bodisi asimptomatski (=brez simptomov) okužbi. V prvem primeru smo okužbo zaznali še pred nastopom simptomov, ki se bodo razvili v nekaj dneh. Pri asimptomatski okužbi pa bo okužba minila brez bolezenskih znakov. V vsakem primeru ima taka oseba virus na sluznici nosno-žrelnega prostora. Virus lahko tedaj pri govorjenju, petju, kašljanju zelo hitro prenese na druge ljudi. To pomeni, da so vsi pozitivni rezultati na novi koronavirus izjemno pomembni, da prekinemo verigo prenosa, preden virus doseže ranljive skupine.
Teorija 2. V laboratoriju ne znajo ločiti virusov. Vse prehlade se pripisuje SARS-CoV-2. Gripe kar naenkrat ni več.
Molekularni test (PCR) je najbolj zanesljiv izmed vseh oblik testov za dokazovanje virusnih okužb in zelo dobro loči viruse med sabo. Ne samo, da ločimo SARS-CoV-2 od prehladnih koronavirusov (HCoV-229E, HCoV-OC43, HCoV-NL63...), ločujemo še bolj ozko sorodne viruse. Npr.: Ko nekdo zboli za gripo in potrebuje bolnišnično zdravljenje, mu določimo tip gripe (A ali B), pri gripi A pa celo podtip (H1N1, H3N2)... Vse to s PCR testiranjem.
Virusi različnih vrst se namreč razlikujejo po genomu in lahko izberemo gene, ki so edinstveni samo za posamezno vrsto virusa. Ko poznamo zaporedje nukleotidov v dednini virusa, lahko izberemo tiste predele, ki jih ima samo ta virus in noben drug na Zemlji.
Z usmerjanjem PCR testa na gene, ki jih ima samo novi koronavirus, zagotovimo, da test PCR slučajno ne prepozna sorodnega virusa (npr. starih koronavirusov) ali drugih virusov, ki povzročajo prehladna obolenja (npr. rinovirusov, RSV...) kot SARS-CoV-2 in se izognemo situaciji, ko bi pri človeku z običajnim prehladnim obolenjem lažno dokazali novi koronavirus. Poleg tega se v vsakem vzorcu dokazuje več genov iskanega virusa. Pri novem koronavirusu dokazujemo 2 do 4 gene (odvisno od testa). Na vsakem od teh genov mora test prepoznati 3 zaporedja v dolžini cca 20 nukleotidov. S tem, ko imamo toliko ujemanj z dednino novega koronavirusa v vzorcu, lahko zagotovo trdimo, da je v vzorcu točno ta virus. »Lovke« v PCR testu, ki iščejo koronavirusne označevalce, se ne ujemajo z geni drugih virusov in napačen rezultat je skrajno malo verjeten.
Prav tako ni res, da ta trenutek ni drugih virusov. Pri zelo ogroženih bolnikih in otrocih, ki rabijo bolnišnično zdravljenje zaradi respiratornega obolenja, vedno iščemo vse možne povzročitelje okužbe. Najbolj pogosti drugi virusi so trenutno rinovirusi in adenovirusi. Splošne populacije, ki je prehlajena in negativna na SARS-CoV-2, ne testiramo na vse povzročitelje okužbe, če pri njih ne pričakujemo zapletov okužbe.
Drži, da trenutno gripa ne razsaja in je pri nas ni. Vendar je severno od ekvatorja v oktobru v zadnjem stoletju tudi ni bilo. (opomba: Po podatkih WHO od februarja, torej od pojava COVID-19 ni gripe nikjer v svetu. Ali res lahko verjamemo v to?) Zakaj bi se potem morali sedaj cepiti proti gripi? Cepiti se moramo preden začne razsajati, ker telo po cepljenju potrebuje rabi še 2-3 tedne, da se vzbudi imunski odziv proti virusom gripe. Šele potem se je imunski sistem zmožen aktivirati takoj, ko pride v stik z nadležnim virusom. Kakšen problem bo predstavljala gripa to sezono, ne vemo. Ampak ob masovnem cepljenju proti gripi (prva dobava cepiva je že pošla), distanci in uporabi mask, mogoče ne bo hudo. Namreč zaščitni ukrepi proti širjenju novega koronavirusa so učinkoviti tudi za prekinitev širjenja gripe, hkrati pa je virus gripe manj nalezljiv in se širi počasneje kot SARS-CoV-2.
Opomba: kako cepivo za gripo v resnici deluje na cepljenje - poveča tveganje za smrt zaradi COVID-19 pri starostnikih, lahko preberete v objavi
Konec opombe
Teorija 3. Laboratoriji ne opravijo objavljenega števila testov, ker tako velikega števila brisov ni mogoče analizirati v enem dnevu.
Na socialnih omrežjih se vrstijo objave, v katerih je opisan postopek PCR reakcije kot tudi ekstrakcije virusne nukleinske kisline (osamitev virusne NK iz virusa). Res je, da celotna analiza vzorca traja cca 4 ure. Zavedati pa se moramo, da se ti postopki ne izvajajo ročno ter da en analizator procesira do 96 vzorcev naenkrat. Natančno število vzorcev, ki jih je možno analizirati naenkrat je odvisno od sistemov, ki jih laboratorij uporablja in njihovega števila.
To najenostavneje ponazorimo s primerjavo s peko piškotov. Lahko pečeš en po en piškot ves ljubi dan ali pa si omisliš pekač in jih pečeš 30 hkrati. Več kot piškotov rabiš speči naenkrat, večji pladenj izbereš. Če pečeš samo en piškot ali nekaj piškotov, je delo opravljeno relativno hitro. Če jih pečeš zelo veliko, že nastanejo zastoji pri ročni obdelavi, prestavljanju, zlaganju, pregledovanju kakovosti, premajhnem robotu za gnetenje, premajhnem pekaču. Pečica pa peče piškote enako dolgo, če imaš notri en piškot ali cel pekač.
Kaj naredimo, če imamo premajhen pekač? Kupimo več pečic. Npr.: Največji južnokorejski laboratorij SCL lahko dnevno analizira do 10.000 brisov, kar je nazorno posneto v spodnjem videu pri minuti 1:28. Slovenski laboratoriji imamo samo po nekaj analizatorjev, medtem ko jih v tem laboratoriju zlagajo v regale kot vložene kumarice. Ta laboratorij je tako zmogljiv, da so vanj v 1. valu z letali vozili brise iz drugih držav, ki niso zmogle testiranja, npr. Finska.
Teorija 5. Izumitelj tehnike PCR Kary Mullis je trdil, da PCR ni primeren za diagnostiko.
Sploh ni pomembno, ali je to rekel. Mullis je dobil genialno zamisel, ki se vsekakor vredna Nobelove nagrade. Reakcija PCR v izvirni različici res ni bila primerna za diagnostiko, ker je bila premalo specifična, je zelo rada nagajala, bila mukotrpna za izvedbo in nevarna za zdravje laborantov. Včasih je pridelala pozitivne rezultate, kar sama od sebe. Ampak od tistih časov do danes je tehnika PCR prestala neskončno izboljšav, ki so posledica genialnosti in velikih naporov številnih drugih kemikov, biokemikov in biotehnologov.
Opomba: Sodobni PCR test je izpopolnil dr. Drosten, proti kateremu bo vložena oškodninske tožbe zaradi prevare s PCR testom, ki bodo potekale v več kot 1000 odvetniških pisarnah po vsem svetu. Več o spornosti PCR testa v nadaljevanju. Konec opombe
* * *
Ovadba glede brisov (testov), ki razkriva veliko prevaro Covid-19
23. oktober 2020
SKUPNA IZJAVA
Podpisani:
Dr. Fabio Franchi, Infekcijski zdravnik, Strokovnjak za virologijo
Dr. Antonietta Gatti, Znanstvena strokovnjakinja za nanopatologije
Dr. Stefano Montanari, farmacevt, znanstveni raziskovalec in nanopatolog
Dr. Stefano Scoglio, znanstveni raziskovalec, kandidat za Nobelovo nagrado za medicino leta 2018
vsi v vlogi strokovnjakov in znanstvenih raziskovalcev, s sklicevanjem na uporabo tako imenovanih brisov (testov) za Covid-19, ki so podlaga sedanjega upravljanja izrednih razmer, povezanih z znanim problemom Covida-19.
IZJAVLJAJO:
-da so iz dokumenta Evropske komisije in drugega dokumenta od inštituta »Istituto Superiore di Sanita'« '[1] ugotovili, da od 16. maja 2020 po Evropi kroži 78 različnih brisov (testov) za Covid-19, od katerih noben ni bil odobren, ocenjen ali potrjen:
- da so iz istih dokumentov ugotovili, da je večina teh brisov (testov za Covid-19) tudi brez deklaracije o vsebovanih genskih zaporedjih, zato so se odločili, da zadevo bolje raziščejo.
Zato so smatrali, da je potrebno poglobljeno raziskati težave v zvezi z veljavnostjo rezultatov brisov (testov) in iz tega bilo je mogoče ugotoviti sledeče;
1) Skladno s priznanjem samega ameriškega Centra za nadzor in preprečevanje nalezljivih bolezni CDC (dok. 3) in delovne skupine za Covid-19 evropske komisije, virus SARS-Cov2 (dok. 2), domnevno odgovoren za Covid, ni bil nikoli fizično-kemično izoliran.
2) Patogene tekočine, ki so bile uporabljene kot model za ugotavljanje zaporedja genov, niso imele titracije virusa, kar pomeni, da so te tekočine vsebovale milijarde drugih virusom podobnih delcev (vključno z nepatogenimi zunajceličnimi vezikli, ki so naravno prisotni v našem organizmu),
To pomeni, da do danes ni nobenega specifičnega označevalca virusa in zato nobenega standarda, ki bi lahko zagotovil zanesljivost brisov (testov).
3) Brisi oz. testi, ki so trenutno v obtoku, več kot 100 jih je, so izvzeti iz nadzora, ki ga določa evropski zakon o medicinskih pripomočkih iz leta 1997;
4) Hkrati zanje še ne velja nov evropski standard iz leta 2017, ki bo začel veljati šele maja 2022.
5) Ta pomanjkljivost v zakonu omogoča proizvajalcem, da brez kakršnega koli nadzora dajo v uporabo katero koli vrsto naprav (testov, pripomočkov).
To pomeni, da skladnost proizvedenih brisov (testov) ni preverjena s standardi, ki lahko potrdijo njihovo pravilno učinkovitost.
6) Obstajajo številne študije, ki potrjujejo nenehno mutacijo virusa, in zdravstvene oblasti same priznavajo, da v kolikor virus še naprej mutira, brisi (testi) postanejo neuporabni.
7) V bazi virusnih podatkov GISAID je skoraj 150.000 različnih zaporedij virusa; aprila jih je bilo 70.000; in še naprej se njihovo število povečuje, saj se vedno najdejo nove mutacije, zaradi česar so brisi (testi) v obtoku popolnoma neuporabni. Na tej točki prilagamo znanstvene raziskave dr. Scoglia, ki prav tako analizira ta bistveni element [3].
To pomeni, da so brisi (testi) v obtoku, četudi naj bi bili abstraktno učinkoviti in dejansko skladni z veljavno zakonodajo, popolnoma neuporabni, saj ne morejo ugotoviti mutacij.
8) Obstaja tudi velik problem, povezan z metodologijo, uporabljeno v brisih (testih), in sicer metodologija RT-PCR. Kot poudarjajo vodilni strokovnjaki za to metodologijo, bi morali za pravilno delovanje v idealnem primeru uporabljati med 20 in 30 ciklov PCR; in v nobenem primeru se ne sme nikoli preseči 35 ciklov, kajti nad tem pragom začne PCR ustvarjati naključna zaporedja. Kot potrjuje več dokumentov, ki jih prilagamo, skoraj vsi brisi (testi) v povprečju presegajo 35–40 ciklov, zato jih je treba šteti za popolnoma neučinkovite in izkazujoče lažno pozitivne rezultate.
9) Nenazadnje, kot je razloženo v nedavnem dokumentu inštituta »Istituto Superiore di Sanita'«, je učinkovitost brisov (testov) odvisna od treh dejavnikov: občutljivosti, zmožnosti zaznavanja prisotnosti RNA, specifičnosti in zmožnosti omejevanja te RNA na ta specifični virus, ki ga iščete; razširjenost oz. prisotnost virusne patologije v populaciji. To je zato, ker večja kot je razširjenost, večja je cirkulacija virusa in zato tudi večja možnost njegovega odkritja. Do danes je razširjenost, ki v resničnih pandemijah lahko doseže celo 30% prebivalstva,v Italiji 0,1%; in tudi če bi se povečala za 10-krat, bi bila še vedno zanemarljiva stopnja razširjenosti; kar na podlagi tabele avtoritativne mednarodne organizacije FIND [4], ki jo je prevzela ISS, pomeni, da brisi (testi) srednje zmogljivosti v Italiji ustvarijo približno 85% -90% lažnih pozitivnih rezultatov.
To pomeni, da so rezultati brisov (testov) kot že zgoraj poudarjeno, popolnoma nezanesljivi.
Zaradi vseh teh razlogov podpisani verjamemo, da je nadaljnja uporaba brisov (testov), iz katerih se pridobivajo koristni podatki za določanje razglasitve izrednih razmer, posamezne ali skupinske karantene in uvajanje omejitev in zapor, od šol do podjetij oz. do družin, praksa brez kakršne koli znanstvene podlage.
Rim, 10.7.2020
Dr. Fabio Franchi
Infekcijski zdravnik
Virološki strokovnjak
Dr. Antonietta Gatti.
Znanstvenik
Strokovnjak za nanopatologije
Dr. Stefano Montanari
Farmacevt, Znanstveni raziskovalec
Nanopatolog
Dr. Stefano Scoglio
Znanstveni raziskovalec
Kandidat za Nobelovo nagrado za medicino 2018
Originalni tekst v italijanskem jeziku
https://www.nogeoingegneria.com/effetti/salute/la-denuncia-sui-tamponi-che-smaschera-il-grande-inganno-del-covid-19/?fbclid=IwAR2gNqzTGo1Iu4WgmPojI2gZsD7qcehOzB6CyKP-goEZbx5_FyofWJazEDU
https://liberopensiero2019.blogspot.com/2020/10/la-denuncia-sui-tamponi-che-smaschera.html
* * *
Takole so zapisali v časniku Times:
“Do 90 odstotkov ljudi, testiranih na koronavirus, imajo komaj kaj delov virusa. Za vse smo uporabili isti tip podatkov, to je le plus ali minus – to je vse,” je povedal dr. Michael Mina, epidemiolog s Harvarda.
“To uporabljamo za klinično diagnosticiranje, za javno zdravje, za sprejemanje odločitev. Menim, da je izjemno neodgovorno, da se ne upošteva, da gre za kvantitativni problem,” je dodal. Večina ljudi, ki imajo 'potrjeno okužbo' s covid-19, se morajo tako za dva tedna izolirati, da še koga ne okužijo – ne glede na to, ali imajo simptome ali ne. Tako niso mogli na delo (izpad zaslužka), niti videti svojih najbližjih, kar ima lahko uničujoe posledice na mentalno zdravje.
Če upoštevamo izsledke tega poročila in seveda tudi dejstvo, da so testi povsem nezanesljivi in sploh niso namenjeni diagnosticiranju, to pomeni, da so vse izolacije in karantene popolnoma nesmiselne.
* * *
PCR TEST JE NEUPORABEN dr. Lanka Stefan
* * *
System and Method for Testing for COVID-19Uitvinder:
ROTHSCHILD RICHARD A [GB]Aanvrager:
ROTHSCHILD RICHARD A [GB]
* * *
Nekateri testi PCR so bili okuženi:
* * *
*
Dr Mila Alečkovič, profesor psihiatrije o neuporabnosti PCR testa: https://www.youtube.com/watch?v=cRNUbBB93JY&feature=share&fbclid=IwAR0vc5y3I_AMAlycy49OzKSM_8XEH_6PgTfIuVIVZi-UmqVxAqPBRwDhJic
*
*
prof. dr Alek Račić, predsednik odbora Srpskega zdravniškega društva: TEST PCR pokaže več vrst koronavirusov, med drugim tudi tiste, ki povzročajo običajen prehlad:
https://vk.com/bratemojne?w=wall598905357_884/all Test odobren of FDA kaže lahko tudi druge koronaviruse, kot so HKU1, NL63, OC43 ali 229E.
*
*
Laži, preklete laži in zdravstvena statistika - smrtonosna nevarnost lažno pozitivnih rezultatov 20. septembra 2020 dr. Michael YeadonDr. Mike Yeadon je nekdanji vodja organizacij civilne družbe, podpredsednik ter direktor za raziskave alergij in dihal pri Pfizer Global R&D in soustanovitelj Ziarco Pharma Ltd.
Nikoli nisem pričakoval, da bom napisal kaj takega. Sem navaden človek, nedavno upokojen iz kariere v farmacevtski industriji in biotehnologiji, kjer sem več kot 30 let poskušal rešiti probleme razumevanja bolezni in iskati nova zdravila za alergijske in vnetne motnje pljuč in kože. Od nekdaj me je zanimalo reševanje problemov, zato mi pritegne pozornost, kadar pride kaj biološkega. Ko je prišlo leto 2020, je prišel SARS-CoV-2. O pandemiji sem pisal čim bolj objektivno. Znanstvena metoda nikoli ne zapusti osebe, ki se je izučila in delala kot profesionalni znanstvenik. Prosim, preberite ta članek. Moji soavtorji in jaz ga bomo predstavili običajnim strogim strokovnim pregledom, vendar je ta postopek počasen in številna nova znanstvena dela so bili letos predstavljena prek strežnikov za predtisk in drugih manj običajnih spletnih mest. Medtem ko smo pozorno spremljali podatke, smo se vsi sprva osredotočili na žalostno zadevo smrti. Zdelo se mi je izjemno, da večina ljudi, s katerimi sem se pogovarjal, pri razpravi o smrtnih primerih, povezanih s COVID-19, ni imela pojma o velikem številu smrti. Na vprašanje, približno koliko ljudi letno umre v Združenem kraljestvu v običajnih okoliščinah, od katerih je vsaka osebna tragedija, običajno niso vedeli. Moral sem jih obvestiti, da je umrlih približno 620.000, včasih manj, če smo imeli blago zimo, včasih precej višje, če imamo sezono hude gripe. To številko omenjam, ker vemo, da je približno 42.000 ljudi umrlo s COVID-19 ali z njim. Čeprav gre za ogromno število ljudi, je v Združenem kraljestvu to 'le' 0,06% prebivalstva. Ni naključje, da gre za skoraj enak delež tistih, ki so umrli s COVID-19 ali od njega v vsaki od močno okuženih evropskih držav - na primer na Švedskem. Letna smrtnost zaradi vseh vzrokov je 620.000 ljudi, kar je 1.700 na dan, poleti je število nižje, pozimi pa višje. Tako je bilo od nekdaj v zmernih pasovih. Torej, v tem kontekstu je 42.000 smrtnih primerov enako smrtnosti od vseh vzrokov v približno ~ 24 dneh. Prosim, vedite, da ne zmanjšujem pomena, ampak samo poskušam dobiti nekaj perspektive. Takšno število smrtnih primerov ni redko in se lahko pojavi v hujših sezonah gripe. Cepiva proti gripi sicer malo pomagajo, toda v zadnjem desetletju je cepljenje doseglo 50-odstotno učinkovitost. So dobra, vendar še nikoli niso bila čarobne krogle za respiratorne viruse. Namesto tega smo se naučili živeti s takšnimi virusi, od številnih prehladov pa vse do pljučnic, ki lahko ubijejo. Zdravila in skrb za človeka delajo po svojih najboljših močeh. Torej, dalje k temu članku. Gre za testiranje, ki ga opravimo z nečim, imenovanim PCR - ojačevalno tehniko, ki je biologom bolj znana kot raziskovalno orodje, ki se uporablja v naših laboratorijih, ko poskušamo ugotoviti mehanizme bolezni. Iskreno presenečen sem bil, ko sem ugotovil, da se včasih uporabljajo pri preverjanju prebivalstva na bolezni - presenečen, ker je to zelo zahtevna tehnika, nagnjena k nevidnim napakam in je precej težavno z njo pridobiti zanesljive informacije, zlasti zaradi izjemnih količin razmnoževanja, vključenega v poskus pridobivanja sekvenc virusne genetske kode. Test PCR ne more razlikovati med živim virusom in kratkim zaporedjem RNA od virusa, ki se je pred tedni ali meseci razlomil na koščke.Verjamem, da sem ugotovil resno, res usodno napako v testu PCR, ki se uporablja pri tako imenovanem pregledu stebra 2 vlade Združenega kraljestva - torej pri testiranju številnih ljudi v njihovih skupnostih. Skozi to bom šel previdno in podrobno, ker sem znanstvenik in mi ni všeč, kamor me bo ta preiskava pripeljala. Nisem posebej političen in imam raje kompetentno in pošteno upravo kot sedanje izbrane politike. V Združenem kraljestvu smo zelo razumni in nismo preveč skrajni. Še posebej zadržan sem glede tega, da mi z upoštevanjem dokazov ne preostane drugega, kot da pokažem, da je Minister za zdravje Matt Hancock zavedel Spodnji dom (House of Commons) in v radijskem intervjuju tudi dal zavajajoče izjave. To so resne obtožbe. To vem. Nisem neusmiljena oseba. Ampak to vseeno pišem, kajti tisto, kar sem odkril, je izjemnega pomena za zdravje in dobro počutje vseh ljudi, ki živijo v državi, ki sem jo vedno klical domovina.
Nazaj k zgodbi in nato k dokazom. Ko je prvi (in mislim, edini) val COVID-19 prizadel Združeno kraljestvo, sem se skoraj s vsemi drugimi zelo bal. Star sem 60 let in dobrega zdravja, toda ko sem izvedel, da imam približno 1-odstotno tveganje za pogubo, če bi dobil virus, sem odkril, da se še zdaleč nisem pripravljen posloviti. Torej, nisem bil presenečen ali jezen, ko je prišla prva zapora (lockdown). Verjetno se je bilo zelo težko odločiti. Preden se je končalo prvo tritedensko obdobje, pa sem začel razvijati razumevanje dogajanja. Stopnja okužbe, za katero je bilo izračunano, da na vrhuncu vsak dan okužila več kot 100.000 novih ljudi, je začela padati in je pred zapiranjem padala. Okužba se je še naprej širila, vendar z vedno manjšo hitrostjo, in to smo videli na prelomnici vsakodnevnih smrtnih žrtev na mračni tiskovni konferenci vsako popoldne. Zdaj vemo, da zaklepanje (lockdown) sploh ni vplivalo na širjenje virusa. To lahko ugotovimo, ker je interval med med ujetjem virusa in smrti pri tistih, ki niso preživeli, daljši od intervala med zaklepanjem in vrhom dnevne smrtnosti. O tem dejstvu ni nobenega polemike, zlahka ki bi ga bilo mogoče dokazati, vendar se zavedam, da se nekateri radi pretvarjajo, da je pandemijo spremenilo zaklepanje (lockdown), morda zato, da bi upravičili visoko ceno, ki smo jo vsi plačali. Ta cena ni bila samo ekonomska. Vključevala je smrt, ki se ji je bilo mogoče izogniti zaradi bolezni, ki niso COVID-19, saj so bile zdravstvene storitve omejene, da bi se osredotočili na virus (op.prev.: SARS CoV-2). Nekateri pravijo, da je zaklepanje (lockdown) neposredno in posredno ubilo toliko ljudi kot virus. Ne vem. To ni nekaj, o čemur sem se želel poučiti. Ampak to omenjam, ker posegov v vse naše življenje ne bi smeli izvajati zlahka. Zaradi takšnih dejanj so ne le neprijetnosti, ampak resnično trpljenje, izguba dohodka, prijateljstev - sidra, ki so za nas vse zelo pomembna, so bila odrezana zaradi teh ukrepov. Prepričani moramo biti, da je nagrada vredna cene. Čeprav je negotovo, da je bilo, sem prvo zaklepanje podprl, saj nismo vedeli, s čim se soočamo, in odkrito, skoraj vsi ostali so to storili, razen Švedske. Zdaj pa odločno nasprotujem nadaljnjim posegom v tisto, za kar sem se prepričal, da je brezploden poskus "obvladovanja virusa". Po mojem mnenju smo – ki ga delijo tudi drugi, od katerih so nekateri na primernem položaju za oceno razmer - bližje koncu pandemije glede števila smrtnih primerov kot pri njeni sredini. Menim, da bi morali vsem ranljivim ljudem zagotoviti najboljšo zaščito, sicer pa previdno nadaljevati življenje. Mislim, da bomo sčasoma vsi postali bolj podobni Švedom. V zadnjih tednih pa ni ušlo nikogaršnji pozornosti, da je prišlo do oznanil, ki se zdijo vsemu svetu kot uvod v še bolj brezplodne in škodljive omejitve. Pomislite na sredino poletja. Bili smo v času po odpravi lockdowna in kljub zaskrbljenosti zaradi natrpanih plaž, velikih demonstracij, odpiranja trgovin in lokalov, je bila glavna novica v zvezi s COVID-19 pomirjujoč in nezadržen padec dnevnih smrtnih žrtev. Opazil sem, da je bila naša krivulja upadajočih smrtnih žrtev, v primerjavi s številnimi bližnjimi državami, preveč položna. Prijateljem znanstvenikom sem celo omenil, da se je ugotavljala prisotnost nekega fiksnega signala, ki se je pomešal z resničnimi smrtnimi primeri zaradi COVID-19. Predstavljajte si, kako razveseljivo je bilo, ko je bila definicija smrti zaradi COVID-19 spremenjena, da se je ujemala z opredelitvijo v drugih državah, in v trenutku se se je naša upadajoča številka smrtnih žrtev ujemala z drugimi po svetu. Bil sem prepričan, da se bo. Tisto, kar smo doživeli in čemur smo bili priča, je bila strašna vrsta dinamičnega ravnovesja (ekvilibriuma). Virus, ki ubije le malo ljudi, nato pusti preživele, ki so skoraj zagotovo imuni - virus, na katerega je bilo morda od 30 do 50% ljudi že prej imunih, ker ima (SARS CoV-2) sorodnike in smo se nekateri že srečali z njimi, predstavlja v celoti strašen, a tudi fascinanten biološki proces . V zadnjih dneh je bil v BMJ objavljen zelo zanimiv prispevek, ki ponuja potencialno podporo tej trditvi. (https://www.bmj.com/content/370/bmj.m3563 Covid-19: Do many people have pre-existing immunity?) Zdaj, ko smo se naučili o nekaterih nenavadnih lastnostih novega virusa, boljšega zdravljenja (protivnetni steroidi, antikoagulanti in zlasti kisikove maske in ne ventilatorji v glavnem), je „stopnja smrtnosti“ tudi za najtežje prizadete posameznike zdaj precej nižja kot pred šestimi meseci. Ker ni nobene temeljne, medicinske ali znanstvene literature, ki bi govorila, da pričakujemo "drugi val", sem postal bolj pozoren na to besedno zvezo, ki se je pojavila na televiziji, radiu in tiskanih medijih istega dne - in ki jo od takrat dalje neusmiljeno ponavljajo. Pred kratkim je z menoj imela intervju Julia Hartley-Brewer v svoji oddaji talkRADIO in takrat sem vlado pozval, naj nam razkrije dokaze, na katere so se zanašali pri napovedovanju tega drugega vala. Zagotovo imajo nekaj dokazov? Mislim, da ne. Iskal sem in sem za to zelo usposobljen, pri čemer sem se opiral na akademske prijatelje in vsi smo bili presenečeni, ko smo ugotovili, da sploh ni ničesar. Zadnja dva nova koronavirusa, SARS (2003) in MERS (2012), sta imela vsak en val. Tudi "valovi" gripe iz 1. svetovne vojne so bili skoraj zagotovo serija posameznih valov, ki so vključevali več virusov. Verjamem, da je vsak pogovor o drugem valu čista špekulacija. Ali je morda nekje v modelu, ki je po moje nepovezan s svetom dokazov? Smiselno bi bilo pričakovati nekaj omejenega, "ponovnega oživljanja" virusa, saj se ljudje ne mešamo kot v kozarcu vode, ampak bolj pavšalno, človeško. Najbolj ste v stiku z družino, prijatelji in sodelavci in to so ljudje, s katerimi si na splošno izmenjujete prehlade. Dolgo obdobje uvedenih omejitev, je poleg običajnih življenjskih preprečilo, da bi se zadnjih nekaj odstotkov virusov mešalo s prebivalstvom. Z gibanjem med počitnicami, novimi službami, obiski daljnih sorodnikov, uvajanjem novih pogojev na univerzah in v šolah poteka dokončno mešanje. To ne bi smel biti strašljiv proces. To se zgodi z vsakim novim virusom, vključno z gripo. Samo še nikoli v zgodovini ga nismo lovili po podeželju s tehniko, ki je bolj primerna biološkemu laboratoriju, kot parkirišču v supermarketu. Zelo dolg, a nujen uvod. Del zelo očitnega "projekta strašenja", ki vključuje druge valove, je bilo dnevno štetje "primerov". Pomembno je razumeti, da po besedah strokovnjakov za nalezljive bolezni, s katerimi sem se pogovarjal, bi beseda „primer“ morala pomeniti več kot zgolj prisotnost nekega tujega organizma. Vsebovati mora znake (stvari, ki jih opazijo zdravniki) in simptome (stvari, ki jih opazite). In v večini tako imenovanih »primerov« tisti, ki so bili pozitivni na testiranju, sploh niso imeli znakov ali simptomov bolezni. Veliko se je govorilo o asimptomatskem širjenju in kot biologa me je to presenetilo. Skoraj v vsakem primeru je človek simptomatičen, ker ima veliko obremenitev z virusi, ki bodisi napadajo njegovo telo bodisi se imunski sistem bori proti njim, na splošno pa potekata oba procesa. Ne dvomim, da je bilo nekaj primerov asimptomatskega prenosa, vendar sem prepričan, da to ni pomembno.Glede na vse to se je vlada odločila, da osebo imenuje "primer", če je njen vzorec brisa pozitiven na virusno RNA, kar se meri v PCR. Vzorec osebe je lahko pozitiven, če ima virus, in tako bi tudi moralo biti. Pozitivni so lahko tudi, če so imeli virus pred nekaj tedni ali meseci in so si opomogli. Obstaja majhna možnost, da bi se na PCR test lahko odzvali tudi sorodni, a različni koronavirusi v velikih količinah, ki lahko povzročijo nekatere prehlade, ki jih imamo, čeprav mi ni jasno, ali se to tudi dogaja. Toda obstaja končna nastavitev, v kateri je človek lahko pozitiven in to je naključen postopek. To ima lahko več vzrokov, saj na primer tehnika ojačevanja ni popolna in tako ojača zaporedja "vab", nameščenih v vzorec, s ciljem združiti se s sorodno virusno RNA SARS-CoV-2. K takim pozitivnim rezultatom PCR testa lahko prispeva še veliko drugih razlogov. To so tako imenovani lažno pozitivni PCR testi.
Pomislite na kateri koli diagnostični test, ki bi ga zdravnik morda uporabil na vas. Idealen diagnostični test pravilno potrdi vse, ki imajo bolezen, in nikoli napačno ne pokaže, da bolezen imajo zdravi ljudje. Takšnega testa ni. Vsi testi imajo določeno stopnjo šibkosti pri ustvarjanju lažno pozitivnih rezultatov. Pomembno je vedeti, kako pogosto se to zgodi, kar imenujemo stopnja lažno pozitivnih. Če je 1 od 100 vzorcev brez bolezni napačno pozitiven- bolezen ni prisotna - temu rečemo 1% lažno pozitivna stopnja. Dejanska ali operativna stopnja lažno pozitivnih vrednosti se včasih bistveno razlikuje glede na različne nastavitve, tehnične operaterje, metode zaznavanja in opremo.
Osredotočam se izključno na stopnjo lažno pozitivnih PCR testov v drugem stebru, ker večina ljudi nima virusa (v zadnjem času približno 1 na 1000 ljudi in prej poleti približno 1 na 2000 ljudi). Ko je količina bolezni, tako imenovana razširjenost, majhna, je lahko kakršna koli stopnja lažno pozitivnih testov velik problem. Ta težava je lahko tako resna, da je brez sprememb (PCR) test brezupno neprimeren za delo, ki se od njega zahteva. V tem primeru je bil in je še vedno test v drugem stebru zadolžen za identifikacijo ljudi z virusom, vendar, kot bom pokazal, tega ne more storiti. Zaradi visoke stopnje lažno pozitivnih rezultatov in nizke prevalence je skoraj vsak pozitiven test, tako imenovani »primer«, ki ga je od maja letos ugotovil 2. steber, LAŽNO POZITIVEN. Ne le nekaj odstotkov. Ni lažna samo četrtina ali polovica pozitivnih PCR Testov, temveč celo okoli 90%. Preprosto povedano, število ljudi, o katerih nam turobno govori gospod Hancock, je približno desetkrat precenjeno. Prej poleti je bilo število precenjeno za približno 20-krat.
Ta PCR test je usodno napačen in se MORA takoj umakniti in se v tej nastavitvi nikoli več uporabiti, razen če bo dokazano, da je popravljen. Primeri, ki sem jih navedel, so zelo blizu tega, kar se dejansko dogaja vsak dan, medtem ko berete to.
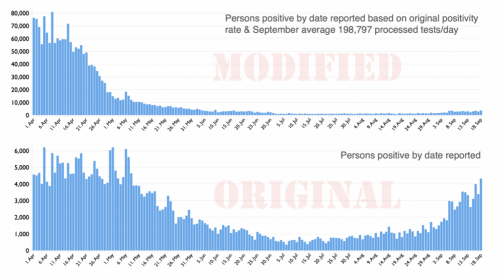
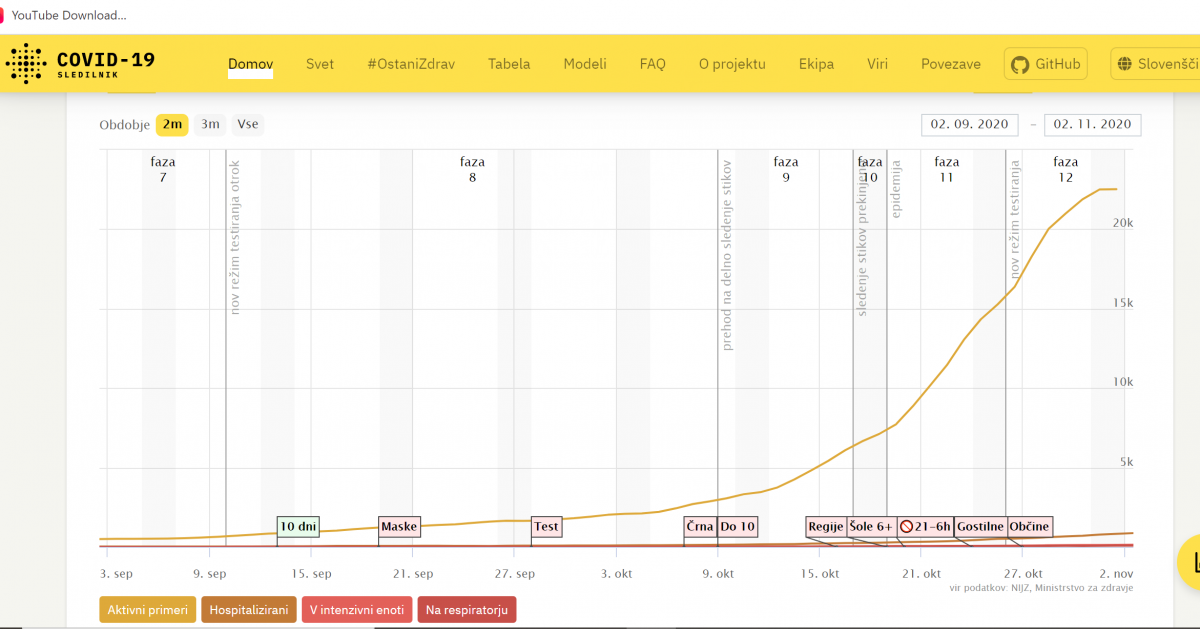
Op. Prev.: Epidemija lažno pozitivnih PCR testov v Sloveniji sep-nov 2020 - pri hospitaliziranih porasta skoraj ni
*
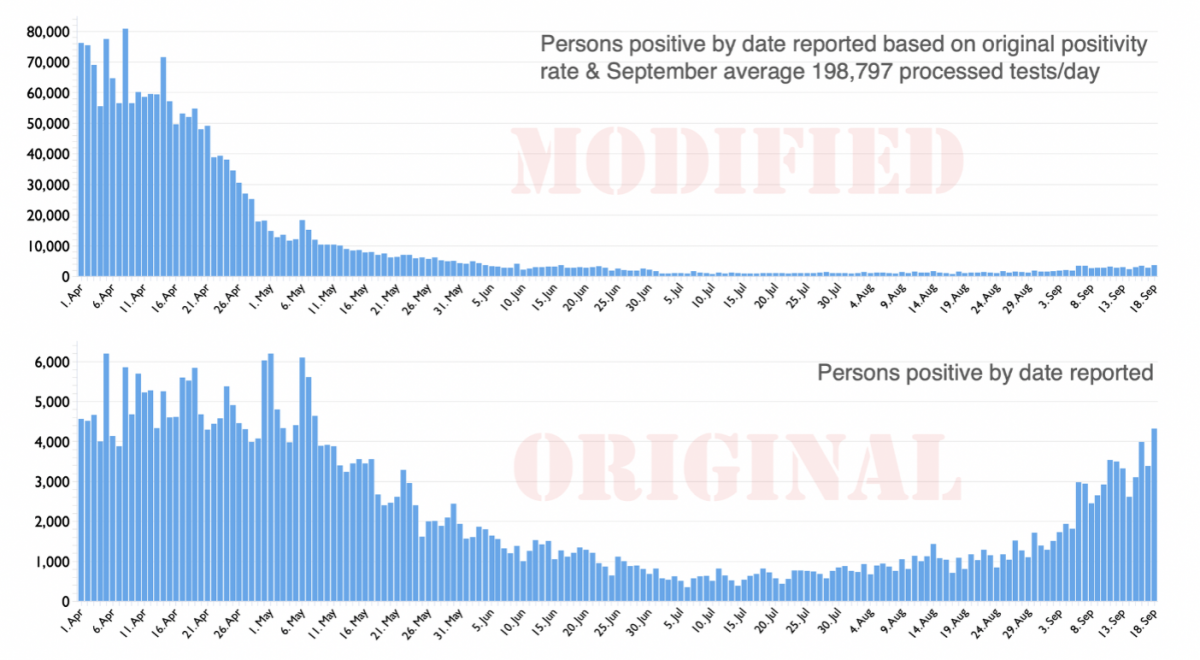
Verjamem, da se resnični primeri okužbe nekoliko povečujejo. To pa velja tudi za gripo, ki je niti ne merimo dnevno niti ne poročamo o njej v vseh novicah. Če bi, bi bili hvaležni za to, da je v prihodnosti zelo verjetno, da bo gripa večje tveganje za javno zdravje kot COVID-19. Verjamem, da popravek primerov (v grafu zgoraj) nedavni porast incidence COVID-19 postavlja v veliko bolj razumen kontekst. Mislil sem, da bi morali videti to razliko, preden sprejmete svojo sodbo o tej žalostni zgodbi. Obstajajo zelo resne posledice grotesknega prevelikega ocenjevanja tako imenovanih primerov v testiranju skupnosti v 2. stebru, za katere menim, da so ga zavestno postavili. Morda g. Hancock verjame v svoj izvod o stopnji tveganja, s katero se zdaj sooča širša javnost? Ni na meni, da to pojasnim. Ta velika pretirana ocena primerov je upočasnila normalizacijo javnega zdravstva. Vsi se zavedamo, da je dostop do zdravstvenih storitev v različni meri omejen. Številne specialistične storitve so bile spomladi močno okrnjene in po nekem okrevanju so nekatere še vedno med tretjino in pol manjše od običajnih zmogljivosti. To je povzročilo nenehne zamude in povečanje čakalnih vrst za številne operacije in zdravljenja. Nisem usposobljen za oceno škode za zdravje naroda in posameznikov kot neposredne posledice tega podaljšanega čakanja na drugi val.Če gremo v zimo s to konfiguracijo, bo poleg že šestmesečnega omejenega dostopa do zdravnikov neizogibno prišlo do velikega števila smrtnih primerov, ki se jim ni mogoče izogniti. To je že dovolj resna obtožba. Manj očitni, v celoti pa dodatni vplivi izhajajo iz strahu pred virusom, neprimerno povečanega po mojem mnenju, ki vključuje: škodo ali celo uničenje velikega števila podjetij, zlasti malih podjetij, s spremljajočo izgubo sredstev za preživetje, izgubo možnosti za izobraževanje, obremenjevanje družinskih odnosov, motnje hranjenja, naraščajoči alkoholizem in zlorabe v družini ter celo samomori, če omenimo le nekaj.
Na koncu želim opozoriti, da je bilo samo v zadnjih 40 letih v Združenem kraljestvu sedem uradnih epidemij / pandemij; AIDS, prašičja gripa, Creutzfeldt-Jakobova bolezen, SARS, MERS, ptičja gripa in letna sezonska gripa. Vse je bilo zelo zaskrbljujoče, vendar so šole ostale odprte in javno zdravstveni sistem je obravnaval vse in večina prebivalstva ni bila prizadeta. Država bi bila redko odprta, če bi jo ob vsaki epidemiji zaprli. Pojasnil sem, kako je bil brezupno neuspešen diagnostični PCR test uporabljen in se še vedno uporablja, ne za diagnozo bolezni, ampak, kot kaže, zgolj za ustvarjanje strahu. Ta zloraba moči mora prenehati. Vsi zgornji stroški so tudi na tehtnici, ko presojamo tveganja za družbo zaradi COVID-19 in sprejemanje ustreznih ukrepov, če sploh katerih. Karkoli se že zgodi, je treba PCR test, uporabljen v 2. stebru, takoj umakniti, saj ne vsebuje nobenih koristnih informacij. V odsotnosti močno napihnjenih števil primerov, ki bi izhajali iz tega testa, bi bila pandemija bolj realno vidna in zdi se skoraj kmalu končana.* * *
COVID-19 v Rusiji: Več kot polovica testov na novi koronavirus napačnih
Znanost in tehnologija, 09 nov 2020, Russia Beyond Slovenija
Strokovnjaki Sečenovske univerze so skupaj s kolegi iz drugih držav ugotovili, da so PCR testi, ki naj bi zaznali prisotnost koronavirusa, v več kot polovici primerov napačni.
Znanstveniki so izvedli študijo o problemu diagnosticiranja COVID-19 v Rusiji in preučevali potek bolezni pri dveh skupinah bolnikov. V vzorec je bilo vključenih 3,5 tisoč bolnikov. Polovica jih je z laboratorijskim testom potrdila prisotnost virusa, ostali pa so bili negativni. Pri tem pa so vsi imeli specifične simptome, stanje njihovih pljuč pa je nakazovalo na COVID-19.
Kot je pojasnil Daniil Munblit, profesor na Oddelku za pediatrijo in otroške nalezljive bolezni Sečenovske univerze, ni bilo bistvenih razlik med simptomi bolnikov, katerih diagnoza je temeljila na rezultatih PCR testa v primerjavi s tistimi, ki so jih diagnosticirali na podlagi klinične slike.
Strokovnjak je poudaril, da v večini držav statistika o koronavirusu ne upošteva ljudi, pri katerih COVID-19 ni laboratorijsko potrjen. "Predvidevamo lahko, da je število ljudi, ki so ozdraveli ali umrli zaradi COVID-19, bistveno večje," je dejal Mublit.
Po mnenju Andreja Prodeusa, raziskovalca na Baltski zvezni univerzi Immanuela Kanta, ni dovolj, da se osredotočimo samo na PCR teste. Ocena klinične slike je veliko pomembnejša. "Če je (test) negativen, še ne pomeni, da virusa ni v telesu," je dejal.
Pred časom je glavni pulmolog ruskega ministrstva za zdravje Sergej Avdejev dejal, da 30-40 odstotkov testov na koronavirus pokaže nepravilen rezultat. Poudaril je, da so napake povezane z nekakovostno odvzetimi vzorci in ne s kakovostjo testov. Pojasnil je, da se verjetnost napačne analize pri PCR diagnostiki za koronavirus povečuje zaradi dejstva, da so bolniki sprejeti v bolnišnico v poznejših fazah razvoja bolezni.
Vir: https://si.rbth.com/science/87435-testi-covid-19-rusija-napacni
*
COVID19 PCR Tests are Scientifically Meaningless
Torsten Engelbrecht and Konstantin Demeter
Datum: 26.6. 2020
Vir: https://off-guardian.org/2020/06/27/covid19-pcr-tests-are-scientifically-meaningless/ ali
Bolgarska zveza patologov : https://bpa-pathology.com/covid19-pcr-tests-are-scientifically-meaningless/?fbclid=IwAR2u0rzjwJ_t13rv9pe8UZeCUb0I3kbPOR2KZvc8CJpp_gY4LaG1GJKl3OE
Del stroke trdi, da je PCR test neprimeren za ugotavljanje, ali je oseba okužena s Koronavirusom SARS CoV-2 ali ne, ker pokaže navzočnost marsikaterih drugih snovi, med ostalim morda tudi prisotnost nukleotidnih sekvenc človeške DNK (ali tudi exosomov).
Drugi del stroke trdi naslednje:
“Druge tehnike (na primer hibridizacija is RT-PCR testom[verižno reakcijo polimeraze z reverzno transkriptazo) lahko zaznajo virusno RNA v tkivih. Poleg tega elektronska mikroskopija lepo omogoča vizualizacijo virusa s konicami (od tod tudi ime koronavirus) v obolelih organih. »Slike koronavirusa, kot so jih patologi opazili v človeških tkivih, lahko vidimo v člankih M. Ackerman [sic] et al. (NEJM 2020) [6], I. Colmenero in sod. (Brit J Dermatol 2020) [7], V.G. Puelles et al. (NEJM 2020) [8] in Z. Varga et al. (Lancet 2020) [9], med drugim.
»...trenutno je relativno sporno, če [ali] gre za resnične virusne delce....«
V članku Health Feedback je tudi zapisano: „Spletni seminar ESP je vključeval posebno sejo, namenjeno metodam za odkrivanje SARS-CoV-2 v človeškem tkivu. Ta seja je pokazala, da patologi z različnimi tehnikami ugotavljajo, ali je bila oseba okužena s SARS-CoV-2, vključno z molekularnimi tehnikami, kot je hibridizacija in situ (ISH).
V spletnem seminarju ESP 25.6. 2020 dr. Varga razpravlja o metodah za odkrivanje SARS-CoV-2 v obdukcijskih tkivih. Vendar zaključuje, ko je razpravljala o članku, ki sta ga skupaj z dr. Mochom napisala skupaj z drugimi do zdaj objavljenimi prispevki o slikah z elektronskim mikroskopom, ki trdijo, da kažejo virusne delce (in je referenca 9 v pregledu Health Feedback), ki vizualizira virus z elektronsko mikroskopijo:
»….zahtevno [in] dolgotrajno, iskanje virusa pa traja včasih tudi nekaj ur. ..«
Dr. Varga tudi ugotavlja, da zahteva veliko strokovnega znanja, ker je mogoče druge strukture in pritrdilne artefakte v tkivih zamenjati za virusne delce. Slednje so popačenja, ki nastanejo med obdelavo tkivnih odsekov za pregled. Predlaga, da so za zagotovitev, ali so virusni delci prisotni v obdukcijskem tkivu, potrebne nadaljnje študije z imunsko elektronsko mikroskopijo, ki je še bolj mučna - in draga - tehnika.
Upoštevajte tudi, da sta Torsten Englebrecht in Konstantin Demeter vprašala skupine znanstvenikov, ki so trdile, da so prečistile in sekvencirale novi koronavirus SARS CoV-2, ali elektronski mikrografi v njihovih objavljenih ugotovitvah kažejo prečiščene viruse. Odzivi znanstvenikov so bili v bistvu "NE". Presenetljivo je, da je virus SARS CoV-2, ki naj bi bil nenehna grožnja vsem nam in preplavlja telesa sto tisoč njegovih žrtev, tako izjemno izmuzljiv. Detekcija koronavirusa v tkivu obdukcije, zlasti v ciljnem pljučnem tkivu, bi morala biti enostavna, saj se virusi razmnožujejo, dokler niso prisotni v dovolj velikih količinah, da ubijejo osebo. Na podlagi vseh dokazov je edini logičen zaključek, da je zelo negotovo, ali so ti "virusni delci" novi koronavirus SARS CoV-2. Doslej objavljene ugotovitve obdukcije niso dokončno pokazale, da je novi koronavirus SARS CoV-2 prisoten v tkivu ljudi, za katere se šteje, da so umrli zaradi COVID-19. Tudi na spletnem seminarju ESP 8. maja 2020 je udeleženec med vprašanji na koncu vprašal: "Ko se ukvarjamo s statistiko, ali vemo, kdo je umrl in kdo umrl s COVID-19?" Dr. Moch je odgovoril: Načeloma ne moremo reči; ne vemo. Ker ima vsak bolnik s COVID-19 posamezen vzrok smrti. Po mojem bi morali opraviti obdukcije in izpeljati izsledke obdukcije, če je bolnik umrl s COVID-19 ali zaradi njega. ""Vendar moramo bolje razumeti potek bolezni pri bolnikih, ki umrejo;" je dejal dr. Moch, ker nekateri bolniki pridejo v bolnišnico z zelo blagimi simptomi in v enem tednu razvijejo hude krvne strdke [trombemboli v pljučih].) Ko so nekaj minut kasneje voditelje spletnega seminarja ESP 8. maja 2020 vprašali, kakšne razlike pri obdukciji obstajajo med bolniki s COVID-19 in bolniki z običajno sezonsko gripo, je dr. Moch po tišini in ponovnem vprašanju rekel: »Težko je odgovoriti. Imamo zelo slabo opisane morfološke slike [tj. ugotovitve patologije] iz primerov sezonske gripe.« Članek Financial Timesa iz 26. aprila 2020 navaja, da so presežno smrtnost opazili v 14 državah. V pregledu je ugotovljeno, da: „Presežno smrtnost, opaženo po vsem svetu leta 2020, lahko pripišemo le pandemiji COVID-19, saj ni nobenega drugega dejavnika, ki bi lahko pojasnil to nenadno povečanje smrtnosti v primerjavi s prejšnjimi leti, ko COVID-19 ni bil prisoten. " Toda ta trditev je zelo neznanstvena: ni podprta z nobeno resnično neodvisno analizo, ali je bila ta smrt posledica novega koronavirusa SARS CoV-2 ali pa drugih vzrokov.
-
Prvič, test PCR, na katerega se sklicujejo pri številu primerov COVID-19, je zelo netočen. Prav tako je zdaj dobro znano, da je domnevnih primerov veliko preveč. Več držav je to končno priznalo. Glejte na primer ta članek 17. julija urednika Off-Guardian Kit Knightly-a.
Drugič, raziskovalec Združenja civilnih svoboščin Ontario dr. Denis Rancourt je opravil analizo, ki je pokazala, da je "vrh COVID-19" umrlih pozimi, to je takrat, ko število smrtnih primerov doseže vrh vsako leto. Vendar je ugotovil, da vrh COVID-19 ni skladen z nobenim drugim vrhom smrtnosti zaradi vseh vzrokov.
Povečanje števila smrtnih primerov, povezanih s COVID-19, se je v ZDA zgodilo le na nekaterih žariščnih točkah, kot je New York City (in se ni zgodilo v zveznih državah, ki niso imele zapore); je trajalo le štiri tedne; in je skoraj v celoti posledica prekomernih smrtnih primerov v domovih za ostarele in ustanovah za oskrbo. Rancourt je zaključil, da:
„Vrh števila umrlih zaradi COVID-19 je posledica pospešene množične smrti imunsko ranljivih posameznikov in posameznikov, ki so postali bolj imunsko ranljivi zaradi vladnih in institucionalnih ukrepov, ne pa epidemiološki podpis novega koronavirusa SARS CoV-2, ne glede na to, v kolikšni meri je virus nov v primerjavi z drugimi virusnimi vrstami.«Tretjič, obstaja veliko drugih pomembnih dejavnikov, ki bi bili lahko povezani s temi smrtnimi primeri, vendar jih Health Feedback in njegovi gospodarji v Svetovni zdravstveni organizaciji (WHO) in drugih "organih", kot je Center za nadzor bolezni (CDC), niso upoštevali.
Tu je sedem glavnih dejavnikov: 1. Resna zdravstvena stanja, ki segajo od bolezni srca in so na smrtnih listih COVID-19 navedena kot zgolj spremljajoča obolenja, vendar so zelo verjetno resnični morilec 2. Uradniki so verjetno šteli, da naj bi veliko smrtnih primerov zaradi gripe povzročil COVID-19. In kot je navedeno v napaki št. 6 zgoraj, je dr. Moch na vprašanje, kakšne so razlike v obdukcijskih ugotovitvah med bolniki s COVID in tistimi s sezonsko gripo, odgovoril: "Težko je odgovoriti. Imamo zelo slabo opisane morfološke slike iz primerov sezonske gripe."3. Med zaustavitvami -karanteno (lock-down) je bilo ogromnemu številu ljudi prepovedan obisk zdravnika ali reševalnih operacij in zdravljenj;
4. Povečale so se tudi stopnje samomorov zaradi zelo obsežne izgub službe, socialne izolacije in drugih pritiskov, povezanih z drakonskimi ukrepi, sprejetimi v predpostavki boja proti COVID-19 5. Poleg tega je bilo zaradi teh ukrepov veliko več nasilja v družini 6. Na območjih, za katera se šteje, da je zaradi novega koronavirusa umrlo veliko ljudi, je bil močno onesnažen zrak 7. V državah, kot je Italija, je povečanje stopnje cepljenja obvezno, kar vodi do višjih stopenj umrljivosti starejših. Osmi dejavnik smrtnosti bi lahko bila tuberkuloza (TB). TB je že dolgo prava pandemija; po podatkih Svetovne zdravstvene organizacije (WHO) letno ubije približno 1,5 milijona ljudi (čeprav je oznaka "pandemija" izginjala iz opisa WHO o stanju TB po vsem svetu). In simptomi tuberkuloze se znatno prekrivajo s simptomi, ki jih pripisujejo COVID-19. Na primer, v vprašanjih in odgovorih WHO za tuberkulozo „Kakšen je potencialni vpliv pandemije COVID-19 na bistvene storitve v zvezi s tuberkulozo?“, piše: Modeli kažejo, da če bi pandemija COVID-19 povzročila skupno zmanjšanje pričakovanega odkrivanja TB za 25% za 3 mesece – kar je realna možnost glede na stopnje motenj v storitvah za TB v več državah - potem lahko pričakujemo 13% povečanje števila smrtnih primerov zaradi tuberkuloze, kar nas vrača na raven smrtnosti zaradi tuberkuloze, ki smo jo imeli pred petimi leti. To je lahko celo konzervativna ocena, saj ne upošteva drugih možnih vplivov pandemije na prenos TB, prekinitve zdravljenja in slabše rezultate pri ljudeh z okužbo s TB in COVID-19 (predvideni vpliv pandemije COVID-19 na smrtne primere zaradi globalne tuberkuloze leta 2020, P. Glaziou). Med letoma 2020 in 2025 bi lahko zabeležili dodatnih 1,4 milijona smrtnih primerov zaradi tuberkuloze kot neposredno posledico pandemije COVID-19 (analiza partnerstva Stop TB). Do danes razviti serološki testi temeljijo na odkrivanju protiteles. In kot smo pokazali v poglavju o napaki št. 2, tudi do danes proizvedena monoklonska protitelesa niso specifična za novi koronavirus SARS CoV-2.PCR TEST ZA COVID-19 JE BREZ ZNANSTVENE VREDNOSTI
Razlog je v tem, da je bila predvidena uporaba PCR uporabljena in je še vedno uporabljena kot proizvodna tehnika, ki lahko milijone in milijarde krat ponovi zaporedja DNA in ne kot diagnostično orodje za odkrivanje virusov. Kako se razglasitev pandemije virusov na podlagi testov PCR lahko konča s katastrofo, je opisala Gina Kolata v svojem članku New York Times iz leta 2007: Vera v hitri test vodi v epidemijo, ki je ni.
Jessica C. Watson z univerze v Bristolu to potrjuje. V prispevku "Razlaga rezultata testa za COVID-19", ki je bil nedavno objavljen v The British Medical Journal, piše, da "ni tako jasnega" zlatega standarda "za testiranje na COVID-19."
A namesto da bi teste PCR označili kot neprimerne za odkrivanje SARS-CoV-2 in diagnozo COVID-19 ali namesto, da bi opozorili, da je le virus, dokazan z izolacijo in čiščenjem, lahko trdni zlati standard, Watson z resnostjo trdi, da je sama "pragmatična" diagnoza COVID-19, ki izjemno vključuje tudi testiranje PCR, " morda najboljši razpoložljivi" zlati standard "." A to ni znanstveno utemeljeno. Poleg tega, da je naravnost nesmiselno jemati test PCR kot del zlatega standarda za oceno PCR testa, za COVID-19 ni posebnih posebnih simptomov, saj to priznajo celo ljudje, kot je Thomas Löscher, nekdanji vodja Oddelek za infekcije in tropsko medicino na univerzi v Münchnu in član Zveznega združenja nemških internistov. [2]. In če za COVID-19 ni posebnih posebnih simptomov, diagnoza COVID-19 - v nasprotju z Watsonovo izjavo - ne more biti primerna za veljaven zlati standard. Poleg tega "strokovnjaki", kot je Watson-ova, spregledajo dejstvo, da je zlati standard lahko le izolacija virusa, torej nedvoumen dokaz virusa. Zato sem Watson-ovo vprašal, kako je diagnoza COVID-19 "morda najboljši razpoložljivi zlati standard", če za COVID-19 ni posebnih posebnih simptomov in tudi, ali virus sam, to je izolacija virusa, ne bi bil najboljši razpoložljivi / možni zlati standard. Toda na ta vprašanja še ni odgovorila - kljub večkratnim prošnjam. In se še ni odzvala na našo objavo o hitrem odzivu na njen članek, v katerem obravnavamo popolnoma enake točke, čeprav nam je zapisala 2. junija: "Odgovor bom poskušala objaviti konec tega tedna, če bom imela priložnost. "PCR test je izjemno občutljiv, kar pomeni, da lahko zazna tudi najmanjše koščke DNA ali RNA - ne more pa določiti, od kod ti delci. To je treba določiti vnaprej. In ker so PCR testi kalibrirani za genska zaporedja (v tem primeru RNA zaporedja, ker naj bi bila SARS-CoV-2 virus RNA), moramo vedeti, da so ti genski delčki del iskanega virusa. Da bi to vedeli, je treba izvesti pravilno izolacijo in čiščenje domnevnega virusa.
Zato smo znanstvene skupine, ki so oblikovale ustrezne dokumene, ki so omenjeni v okviru SARS-CoV-2, prosili za dokaz, ali elektronsko-mikroskopski posnetki, prikazani v njihovih poskusih in vitro, kažejo prečiščene viruse. Toda niti ena ekipa ni mogla odgovoriti na to vprašanje z "da". Nihče ni rekel, da čiščenje ni nujen korak. Dobili smo samo odgovore, kot so »Ne, nismo dobili elektronskega mikrografa, ki prikazuje stopnjo prečiščenja« (glej spodaj).But not a single team could answer that question with “yes” — and NB., nobody said purification was not a necessary step. We only got answers like “No, we did not obtain an electron micrograph showing the degree of purification” (see below).
Study 1: Leo L. M. Poon; Malik Peiris. “Emergence of a novel human coronavirus threatening human health” Nature Medicine, March 2020
Replying Author: Malik Peiris
Date: May 12, 2020
Answer: “The image is the virus budding from an infected cell. It is not purified virus.”
Study 2: Myung-Guk Han et al. “Identification of Coronavirus Isolated from a Patient in Korea with COVID-19”, Osong Public Health and Research Perspectives, February 2020
Replying Author: Myung-Guk Han
Date: May 6, 2020
Answer: “We could not estimate the degree of purification because we do not purify and concentrate the virus cultured in cells.”
Study 3: Wan Beom Park et al. “Virus Isolation from the First Patient with SARS-CoV-2 in Korea”, Journal of Korean Medical Science, February 24, 2020
Replying Author: Wan Beom Park
Date: March 19, 2020
Answer: “We did not obtain an electron micrograph showing the degree of purification.”
Study 4: Na Zhu et al., “A Novel Coronavirus from Patients with Pneumonia in China”, 2019, New England Journal of Medicine, February 20, 2020
Replying Author: Wenjie Tan
Date: March 18, 2020
Answer: “[We show] an image of sedimented virus particles, not purified ones.”
http://tapnewswire.com/2020/10/there-is-no-proof-sars-cov-2-causes-covid19/?fbclid=IwAR2JcmdRdfJYio2zWt6Squu_v2HfMD87zUHIXyxkqanEJn_zIqwusRAIgE8
* * *
Več avtorjev študij smo vprašali "Ali vaši elektronski mikrografi kažejo očiščen virus?", Odgovorili so, da ne. Tako avtorji štirih glavnih študij iz začetka leta 2020, ki trdijo, da so odkrili nov koronavirus, priznavajo, da niso imeli nobenega dokaza, da so izvor genoma virusa podobni delci ali celični ostanki, čisti ali nečisti ali kakršni koli delci. Z drugimi besedami, obstoj RNA SARS-CoV-2 temelji na veri in ne na dejstvih. Kontaktirali smo tudi virologa dr. Charlesa Calisherja, ki je povedal o PCR testu naslednje: Sodobne metode odkrivanja virusov, kot je gladka verižna reakcija s polimerazo [PCR test…], malo ali nič ne govorijo o tem, kako se virus razmnožuje, katere živali ga prenašajo, ali kako ljudje zbolijo. To je, kot če bi s pogledom na prstni odtis osebe poskušali ugotoviti, ali ima slab zadah.« To dejansko pomeni, da ni mogoče sklepati, da genska zaporedja RNA, ki so jih znanstveniki odvzeli iz vzorcev tkiva, pripravljenih v omenjenih preskusih in vitro in za katere se PCR testi končno »kalibrirajo«, spadajo v določen virus - v tem primeru SARS-CoV-2. Poleg tega ni znanstvenih dokazov, da so ta zaporedja RNA povzročitelji tega, čemur pravimo COVID-19. Da bi vzpostavili vzročno zvezo, tako ali drugače, torej onstran izolacije in čiščenja virusov, bi bilo nujno izvesti eksperiment, ki bi ustrezal štirim Kochovim postulatom. A takšnega eksperimenta ni, kot sta pred kratkim za OffGuardian razkrila Amory Devereux in Rosemary Frei. Nujnost izpolnjevanja teh postulatov Kocha glede koronavirusa SARS-CoV-2 dokazuje tudi dejstvo, da so bili poskusi, da bi jih izpolnili. Toda tudi raziskovalci, ki trdijo, da so to storili, v resnici niso uspeli. Čeprav trdijo, da so "virusologi v Charitéju prepričani, da testirajo na koronavirus," v svojem prispevku (Corman et al.) Navajajo: RNA so ekstrahirali iz kliničnih vzorcev s sistemom MagNA Pure 96 (Roche, Penzberg, Nemčija) in iz supernatantov celičnih kultur z mini kompletom virusne RNA (QIAGEN, Hilden, Nemčija), kar pomeni, da so samo domnevali, da je RNA virusna. Laboratorij za diagnostiko je 22. marca 2020 poslal pismo skupini za odziv na koronavirus pri Svetovni zdravstveni organizaciji (WHO) in Anthonyju S. Fauciju, (vodji kriznega štaba v ZDA), v katerem pravijo: V družabnih medijih so pogosto poročali, da testni kompleti RT-qPCR [Kvantitativna PCR reverzna transkriptaza], ki se uporabljajo za odkrivanje RNK SARSCoV-2 v človeških vzorcih, dajejo veliko lažno pozitivnih rezultatov in niso dovolj občutljivi za odkrivanje nekaterih resničnih pozitivnih primerov. " Z drugimi besedami, tudi če teoretično predpostavimo, da lahko ti PCR testi resnično odkrijejo virusno okužbo, bi bili testi praktično brez vrednosti in bi med "pozitivnimi" testiranimi ljudmi povzročili le neutemeljeno prestrašenje. Več o pomanjkljivostih PCR testa je v članku: https://off-guardian.org/2020/06/27/covid19-pcr-tests-are-scientifically-meaningless/
* * *
Sladoljev Srećko je delila objavo.
Zbog prekjučerašnje objave šest „dalekovidnih“ političkih ciljeva preko društvenih mreža, „kažnjen“ sam jednodnevnom uskratom objavljivanja radi „kršenja standarda zajednice“!? Cenzori jesu u pravu ako je razmišljanje „svojom glavom“ kršenje tih „standarda“. Ali njihovo nametanje u informativnom prostoru suverene zemlje briše dvojbu je li Duboka država uzela sebi za pravo intervenirati u njen suvereni prostor!
U objavi ću upozoriti na vjerodostojnost RT-PCRa, metode kojom se ljudima globalno „pumpaju“ glave panikom i strahom od smrti. Pogrešno interpretirajući rezultate RT-PCR testa, Imunološki zavod je još prije dvadesetak godina globalno zazivao bojkot svog najperspektivnijeg proizvoda – prirodnog leukocitnog nativnog interferona. Objaviti ću sramotu da provjerimo da li je Dubokoj državi svaka istina „kršenje standarda zajednice“?
-
Covid gripa, to znaju i vrtićka djeca, „dokazuje“ se RT-PCR-om, i najosjetljivijim i najnepouzdanijem testom istovremeno. Dovoljno je da u uzorak zaluta mikroskopska čestica kože da test možda pođe ukrivo. Zbog toga će vam „prekjučer“ „dokazati“ da imate Covid i strpati s kovidašima, danas ga nećete imati, a sutra je opet tu (jer ste ga pokupili od kovidaša). Mogu dati i podatke.
-
Ne tvrdim, ali moguće da sam prvi u svijetu JAVNO osporio istinitost rezultata dobivenih RT-PCR testom koji su objavljeni u znanstvenom radu, u "evidence based". Objasnio sam i gdje se pogriješilo. Iako sam bio u pravu (jer je WHO je kratko nakon toga promijenio naputak za izvođenje testa!), dobio sam zbog toga i prvo upozorenje iz radnog odnosa. bilo je to prije dvadesetak godina. Idemo redom.
Imunološki zavod uveo je RT-PCR za otkrivanje virusa hepatitisa C (HCV) u doniranoj krvi 1996.g., dvije godine prije preporuke WHO-a. U prilogu 1. rezultati su RT-PCRa na HCV od 1997. do 2002. g. (u proizvodnji interferona koriste se ljudski leukociti!). Crveno su HCV pozitivne, a plavo HCV negativne serije. Do sredine 1998. sve su serije (uglavnom) bile pozitivne, a od sredine 1998., kada sam i preuzeo proizvodnju, sve su bile (uglavnom) negativne.
-
Međutim serije interferona nisu bile odbačene zbog HCVa, već niskih titrova i zagađenja (prilog 2). U dopisu direktoru od 8.9.1998., ukazujem na 4 slaba mjesta proizvodnog postupka, među njima i „neadekvatno sakupljanje i transport leukomase“ što se kasnije pokazalo preduvjetom ispravnog izvođenja testa i vjerodostojnosti RT-PCR rezultata (prilog 3)!
-
Po uvedenim izmjenama, proizvodnja je krenula već krajem 1998. Desilo se „čudo“! Nije se dugo čekalo na „intervenciju“ predstojnice Finalne kontrole (čije su „aktivnosti“ i dovele do gašenja proizvodnje!), cit. „Ne dvojim da ste u stanju poboljšati proizvodni postupak za pripravu HAS-a, virusa induktora, primera i gotovog proizvoda, no važeći Vas zakoni obvezuju da u pismenoj formi Odjelu za kontrolu kvalitete obrazložite svaku promjenu proizvodnog postupka bilo koje ulazne tvari ili međuproizvoda. Promjene koje ste uveli tijekom proizvodnje serije 1138 su ozbiljne promjene……“ …. , „Vaš prigovor o neupućenosti Vaših ljudi u zahtjeve pri uzorkovanju (za RT-PCR) neosnovan je. Osobno sam održala dva sastanka na temu ispitivanja HCV-RNA pomoću RT-PCR s Vašim ljudima, no to je bilo prije Vašeg dolaska na tu dužnost.“ (prilozi 4 i 5).
-
Da, desilo se i drugo „čudo“ - prva serija interferona ne samo da je „prošla“ već je bila i HCV negativna!
11.2.1999. šaljem naputak Kontroli kako ispravno uzorkovati međuproizvod interferona za RT-PCR (u cc dr Markotić , tada voditeljica kontrole interferona) (prilog 6).
18.2.1999. stiže odgovor predstojnice, „Bojim se da Vaše iskustvo u izvođenju RT-PCR za HCV RNA nije dovoljno da biste mogli argumentirano inzistirati na promjenama uspostavljenog sustava. U Imunološkom zavodu je uspostava in-house RT-PCR za HCV RNA i validacija istog trajala je tri godine (obzirom na Vaše osobno iskustvo u rekonstrukciji postojeće proizvodnje, uzmite u obzir da prije toga nije bilo molekularne biologije u Imunološkom zavodu). Kroz to su vrijeme suradnici Odsjeka za molekularnu biomedicinu sudjelovali u kolaborativnoj studiji na europskoj razini (Viral Qaulity Control ….. etc.) …..
-
….“ Rado ću s Vama raspraviti Vaše teorije KADA ONE DOBIJU EKSPERIMENTALNU POTVRDU. U međuvremenu Vas uvjeravam da je RT-PCR vrlo skup test te da Imunološki zavod u ovom trenutku nema dovoljno sredstava za nedovoljno obrazožene eksperimente, odnosno prijedloge eksperimenata koji nemaju ZADOVOLJAVAJUĆU ZNANSTVENU POTPORU.“ (prilog 7)
Niti riječi na činjenicu da je proizvodnja nakon dvije godine krenula i to BEZ virusa hepatitisa? I nije točno da „prije toga nije bilo molekulske biologije na Imunološkom zavodu“. Započeo sam kao voditelj Laboratorija za molekulsku biofiziku. A to je još "sofisticiranije".
-
Niz HCV negativnih serija interferona prekinule su tri pozitivne. Internom istragom shvatili smo da je došlo do propusta u postupku prikupljanja i transporta leukocita zbog čega je u proizvodni postupak i testiranje dospjelo neuobičajeno mnogo mrtvih stanica. Desilo se čega sam se pribojavao. Iako sam UNAPRIJED upozorio Kontrolu da bi serije radi interferencije s humanim nukleinskim kiselinama mogle biti HCV pozitivne (!), Kontrola se žuri objaviti znanstveni rad radi vlastite znanstvene promičbene ne mareći što teško kompromitira Imunološki zavod, cit. "The aim of this study was to determine the rate of HCV RNA positive batches of human native leukocyte interferon during large-scale production. Our findings indicate the presence of HCV RNA in 6,1% batches despite acidification of intermediates in order to inactivate Sendai virus.“ (prilog 8).
-
Agencija za lijekove Hrvatske uvodi posebne mjere nadzora i zaustavlja proizvodnju.
S kolegama, dr Toothom iz Mađarske i dr Filipičem iz Slovenije, sastavljama i šaljemo Pismo urednicima (Letter to the Editors) pod naslovom "On the responsibility and ethics of scientific contribution" kojim osporavamo vjerodostojnost objavljenog rada! Isključujem se kao supotpisnik da tvrtku ne bih izvrgao većem ruglu (prilozi 9, 10, 11).
Interveniram i kod ravnateljice Hrvatskog zavoda za kontrolu imunobioloških preparata. Vjeruju mi i vraćaju proizvodnju.
-
Uprava (SDP) promptno šalje Upozorenje iz radnog odnosa pred otkaz, cit. "Dana 25.3.2003. uputili ste ravnateljici Hrvatskog zavoda za kontrolu imunobioloških preparata dopis vezan za proizvodnju interferona i Vaše osobno viđenje problematike, a bez znanja Uprave – Glavne direktorice. Time ste prekršili ovlaštenja koja imate temeljem Ugovora o radu i skrećem pozornost na posljedice ovakvog Vašeg istupa bez mog znanja i odobrenja.“ (prilog 12)
14.4.2003. odgovaram na Upozorenje Uprave (prilozi 13 i 14)
14.6.2004. nakon podvala na granici kriminala (podmetanje krađe iza koje je mogla stajati jedino Uprava!), ova me obavještava da je protiv mene pokrenula Postupak prije otkazivanja ugovora o radu (prilog 15).
Otkaz je i otpravljen, ali nije realiziran jer je Nadzorni odbor desetak minuta prije uručenja smijenio Upravu zbog štetnih radnji.
Svjetska zdravstvena organizacija (WHO) kratko nakon toga izdala je nove preporuke za izvođenje RT-PCR na uzorcima iz ljudske krvi. Ako je od uzimanja do testiranja uzoraka prošlo više od dva sata, rezultati se nisu bili vjerodostojni. Dva znanstvena rada rada potvrdila su kako nukleinske kiseline ljudi kompromitiraju test dajući LAŽNO POZITIVNE rezultate.
-
Ne trebate mnogo mašte da zamislite što je s uzorcima za testiranje Covida RT-PCR testom? Zamislite koliko je tek MRTVIH STANICA u ispljuvku prehlađenih i gripoznih!
Objavljeno na FB Svobodo odločanja glede cepljenja otrok 22.6. 2020
Dokumentarac 8.7. 2020:
https://dokumentarac.com/covid-19/pouzdanost-pcr-testova-u-svrhu-detekcije-covid-19/
Ništa na ovom Svijetu nije u tako kratkom vremenu promijenilo živote toliko ljudi kao PCR test za kojeg neki tvrde da je pogodan i za otkrivanje živih virusa i za davanje dijagnoze. Dapače neki idu još dalje pa na temelju tog testa čak određuju uzrok smrti. Stoga sam ja odlučio pisati o tome testu koji je umnogome promijenio naš život. Pisati ću na način da i ljudi koji nisu stručnjaci, dapače da i ljudi koji imaju završenu samo osnovnu školu mogu razumjeti. Zbog toga tekst mora biti širok i detaljan, a što nažalost znači i dug. Ali taj test vam može promijeniti život pa vam preporučam da ustrajete s čitanjem teksta do kraja.
PCR je osmišljen kako bi od vrlo male količine genetskog materijala napravio puno više. Zbog toga da bi razumjeli PCR test trebamo znati osnove genetskog materijala.
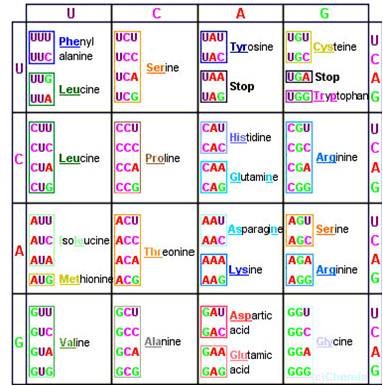
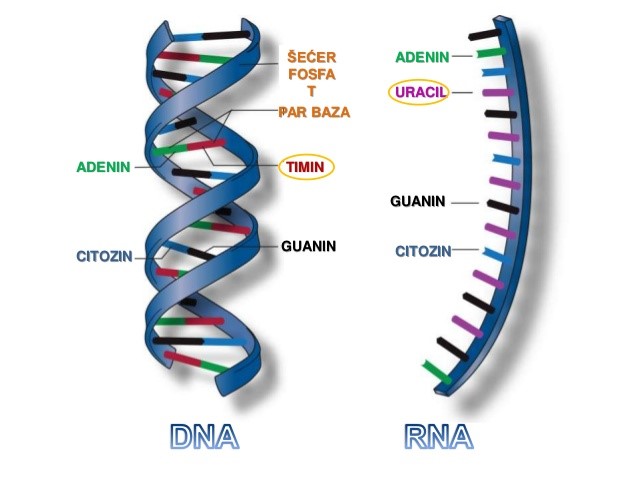
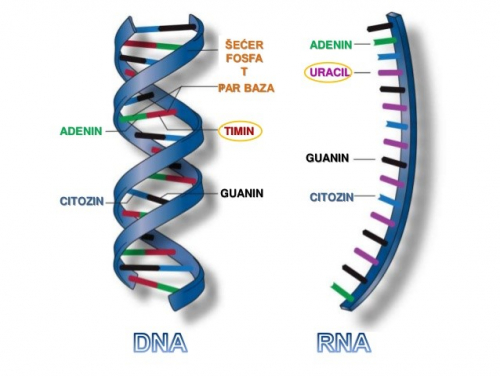
Genetski materijal se sastoji od četiri različite baze Ademin, timin, citozin i guanin. Po prvom slovu njihovog imena skraćenice su im A, T, C i G. Cijeli genetski materijal se sastoji od slijeda puno takvih baza. Predstavlja se da ljudi imaju slijed od oko 4*10^9, a corona virus slijed od samo oko 30 000 takvih baza. Još jedna važna razlika je što se ljudski genetski niz sastoji od dvostrukog lanca komplemetarnih baza i to DNA a kod korona virusa je samo jednostruki lanac i to RNA. Komplementarne baze su A i T te C i G koje se zbog različitih vodikovih veza međusobno vežu pa se zato i nazivaju komplementarnima. Kod RNA se umjesto, kao što se slici može vidjeti, Timina nalazi malo promijenjena baza Uracil.
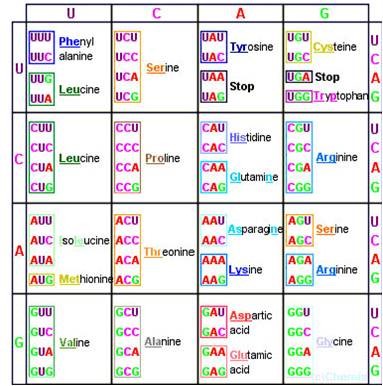
Te 4 baze služe kao kod za izradu proteina. Međutim, aminokiselina koje grade proteina imamo 20. Pa se postavlja pitanje kako 4 različite baze mogu šifrirati 20 različitih aminokiselina. Pa tako što ćemo očito trebati neki dulji niz baza, a ne samo jednu. Slijed od 1 baze može dati 4 različita koda (A, T, C, G) ali zato slijed od dvije baze može dati 16 različitih kombinacija (AA, AT, AC, AG, TT, TA, TC, TG, CC, CA, CT, CG, GG, GA, GT,GC). Ali ni to nije dovoljno da bi kodiralo 20 različitih aminokiselina. Ali zato slijed od 3 baze može dati 4^3=64 različitih kombinacija. To je mnogo više kombinacija od 20 potrebnih za različite aminokiseline plus Start i Stop kod. Zbog toga više različitih kodova kodira istu aminokiselinu. Koga zanima na slici može vidjeti koji kodovi odgovaraju kojoj aminokiselini.
Sada smo vidjeli kako genetski kod kodira aminokiseline koje su osnovne građevne jedinice proteina. Kako bi mogli obavljati svoju funkciju proteini se sastoji od mnogo različitih aminokiselina. Funkcija proteina je izgradanja stanice te obavljanje rada. Oni proteini koji ne sudjeluju u izgradnji stanice i njenih struktura su u biti nano roboti koji obavljaju rad u stanici.
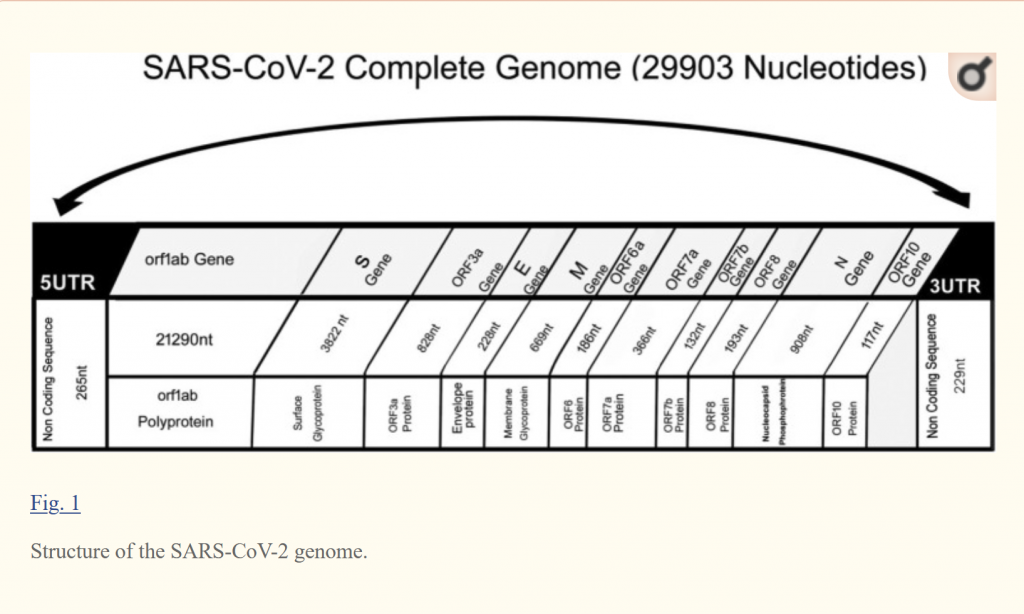
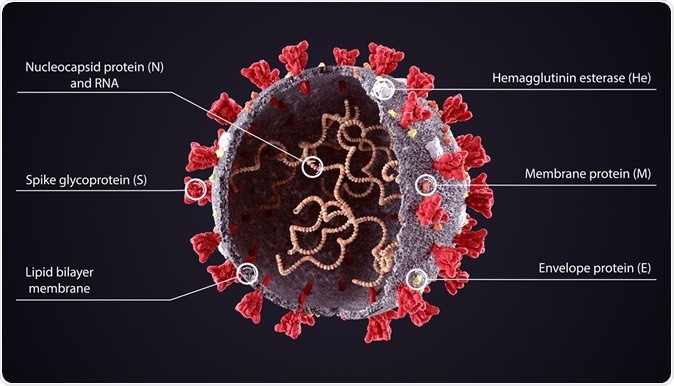
Virusi su najjednostavniji biološki entitet. Oni nemaju jezgru. Oni se sastoje od genetskog materijala obavijenog membranom. Na slici je prikazan Sars-Cov-2 virus sa proteinima koje šifrira RNA koja se nalazi unutar membrane.
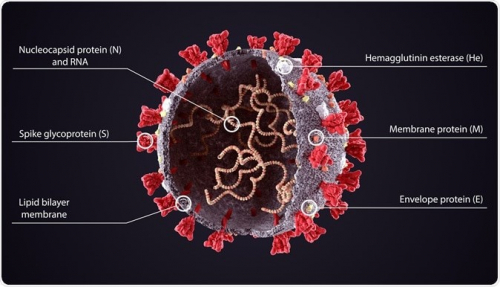
U tih 30 000 baza SARS-COV-2 virus kodira Spike protein, Hemagglutinin esterase, membranski protein i envelope protein. U ovom članku https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7161481/ , objavljenom 19.6., možete vidjeti koliko baza(nukleotida(nt)) kodira koji od gore navedenih proteina
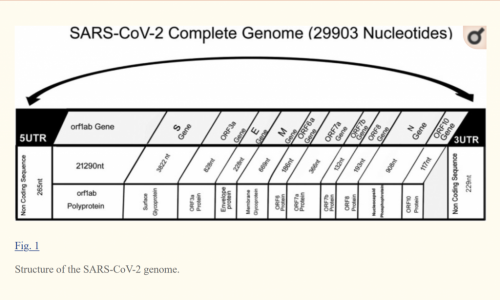
S gen, koji kodira spike protein ima 3822 nukleotida(baza), E gen samo 228, a N gen 908. To su svi podaci koji će nam trebati o virusu zbog kojeg su vam neki odlučili promijeniti život.
A sada ćemo opisati PCR tehniku. Na ovom videu je lijepo objašnjena PCR tehnika https://jubitu.com/videos/watch/a81edc45-cbb2-4838-8026-28d6fea8443e
Možemo ju podijeliti u 3 djela: prikupljanje uzorka, priprema uzorka te umnožavanje genetskog materijala i detekcija kratkog slijeda baza. Prikupljanje uzorka je najosjetljiviji dio te samim time treba mnogo iskustva kako bi se uzorak ispravno prikupio, tj. kako rezultati PCR testa ne bi ovisili o načinu prikupljanja uzorka. Nakon toga tako prikupljene uzorke je potrebno obraditi da način da u njima ostane samo genetski materijal. Ako pretpostavimo da je u uzorcima bio cijeli virus, to znači da treba razoriti njegovu ovojnicu, pročistiti sve te krhotine kako bi se ekstrahirao samo genetski materijal. U zadnjem koraku se taj genetski materijal umnožava.
Zadnji, treći korak, umnožavanje i detekcija kratkog slijeda baza se odvija na slijedeći način. U epicu (mala posuda) u kojoj se nalazi RNA se doda reverzna transkriptaza i DNA polimeraza (to su 2 nano proteinska robota), forward i reverse primer, te proba koja na sebi ima molekulsku boju i na drugom kraju quencher, te mnoštvo nukleotida. U prvom koraku se od RNA napravi komplementarna DNA na način da se reversni primer veže na RNA na mjesto na koje će potom doći reversna transkriptaza (nano robot) i sintetizirati drugi lanac iz nukleotida koji se nalaze u otopini. Nakon toga se temperatura povećava do 95 stupnjeva Celzijusa kako bi se takva dvolančana RNA denaturirala u dvije jednolančane te u isto vrijeme deaktivirala reversna transkriptaza i aktivirala DNA polimeraza. Nakon toga na te dvije jednolanačne RNA vežu se forward i reverse primeri te proba sa bojom. DNA polimeraze (nano proteinski roboti) dolaze na mjesto gdje se primer vezao i sintetiziraju drugi lanac. Tijekom sinteze sa probe otkače molekulsku boju i quencher. I tako nakon prvog koraka od dvije jednolančane RNA imam dvije DVOLANČANE RNA, te jedan par molekularne boje i quenchera koji nisu spojeni, tj. nalaze se negdje u otopini na velikoj udaljenosti. Ova procedura se ponavlja mnogo puta i tako se u svakom koraku dobije duplo više dvolančane RNA i duplo više molekularnih boja koje su udaljene od svojih quenchera.
Molekularna boja kada je pobuđena svijetlom emitira svijetlo malo niže frekvencije od one kojom je pobuđena. Međutim, molekularna boja ne emitira svijetlo ako se u blizini nje nalazi quencher. Tako da tek kada se quencher udalji od molekularne boje ona može emitira svjetlo. Bilježenjem intenziteta tog svijetla se može odrediti da li se u epici nalazi genetski materijal na kojeg su se vezali primeri i proba.
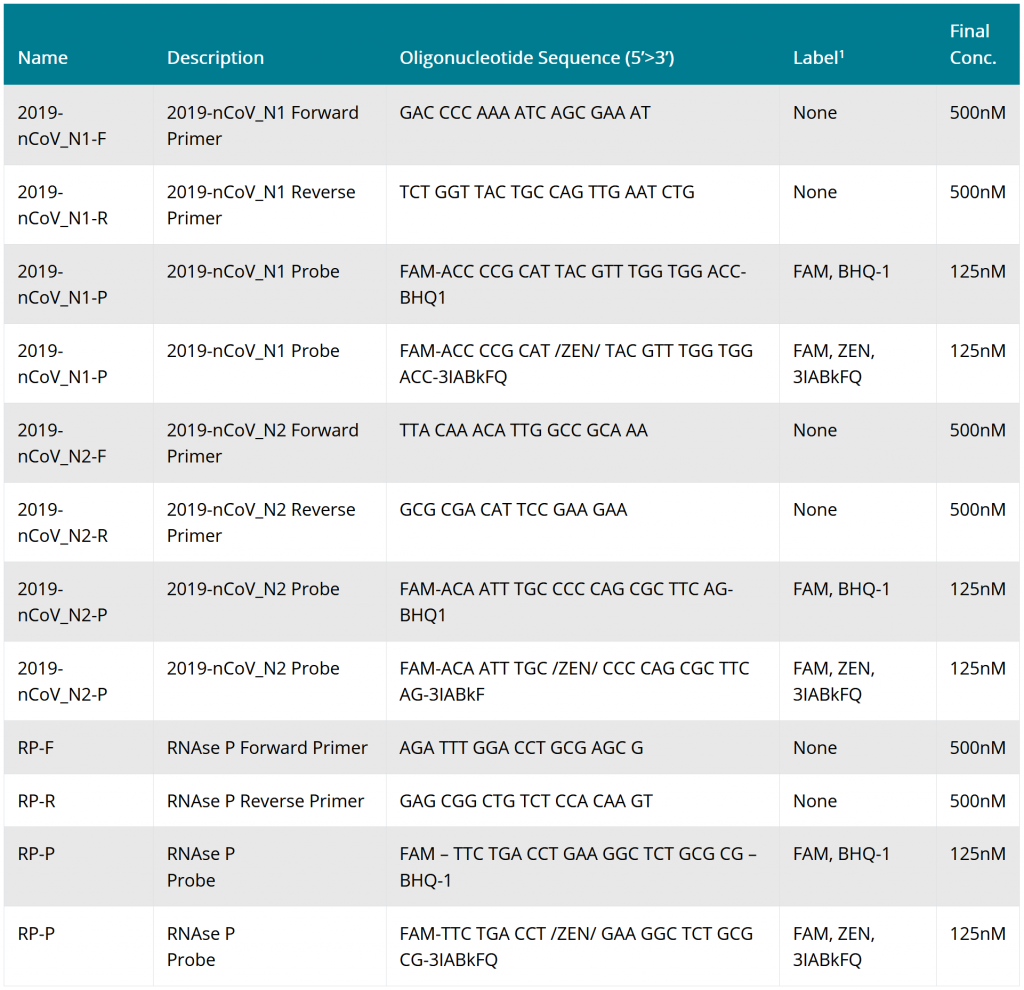
Sijed baza forward i reverse primera i proba koji CDC predlaže za test na SARS-Cov-2 možete vidjeti na njihovim stranicama https://www.cdc.gov/coronavirus/2019-ncov/lab/rt-pcr-panel-primer-probes.html
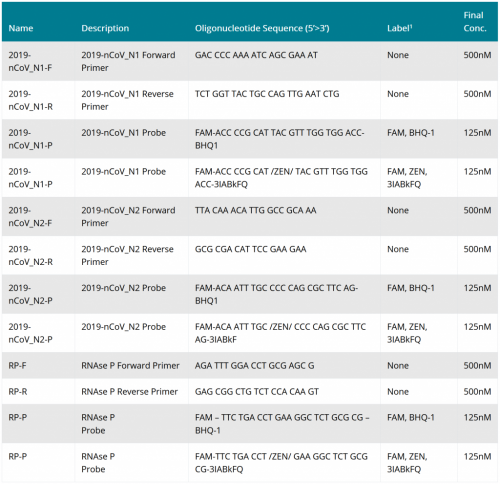
Iz cijele ove tablice glavni podatak koji bi trebalo zapamtiti je da i forward i reverse primere i boje (probe) se sastoje od samo otprilike dvadesetak nukleotida.
Sada možemo zaključiti što u biti PCR tehnika detektira. PCR tehnika ne detektira kompletan, funkcionalan virus nego samo fragmente genetskog materijala. I to od 2×30 000 baza genetskog materijala dovoljno je samo dvadesetak baza reverse primera i dvadesetak baza boje te na drugom lancu samo dvadesetak baza forward primera da bi dobili pozitivan signal. Znači od 30 000 baza genetskog materijala na temelju samo 60 baza može se dobiti pozitivan odgovor. To je samo 0.2% cjelokupnog genetskog materijala Sars-cov-2 virusa.
Sada ćemo navesti samo neke načine kako tako mala specifičnost testa može dovesti do lažno pozitivnog rezultata.
1. U uvodu članka objavljenog 2012 godine https://www.sciencedirect.com/science/article/pii/S1879625711001908 napisano je:“ Viral metagenomic analyses of environmental samples suggest that the field of virology has explored less than 1% of the extant viral diversity… One L of seawater can contain as many as 1010 virus-like particles (VLPs) [1], approximately 10 times more than the number of prokaryotes. Terrestrial environments often have 109 VLPs per gram. By extrapolation from the estimated number of prokaryotes in different environments [2], viruses are the most abundant entities in the biosphere totaling an estimated number of 1.2 × 1030, 2.6 × 1030, 3.5 × 1031, and 0.25–2.5 × 1031 in the open ocean, in soil and in oceanic and terrestrial subsurfaces, respectively… While no VLPs could be detected in the earliest infant stool samples, there were ∼108 virus particles per gram wet weight of feces by the end of the first week.“
U članku, objavljenom 2014 godine https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4147198/ piše:“ There are some amounts of the virus in the air constantly. These amounts is generally not enough to cause disease in people, due to infection prevention by healthy immune systems.“
Iz ta dva rada možemo izvući jako puno, ali ja ću navesti samo ono najznačajnije za PCR testove. U 1 litri morske vode nalazi se 1010 čestica nalik virusima (to je više nego ljudi na zemlji). Svaka od tih čestica sadrži genetski materijal. Virusi se konstantno nalaze u i zraku. Osim toga procjenjuje se da je virologija otkrila manje od 1% virusa.
Kada znamo te činjenice postavlja se pitanje kako se uzorci za PCR analizu štite od kontaminacije?
Tvrtke koje proizvode mikro čipove su osmislile kompleksne sustave, čiste sobe (eng. cleanroom) kako da osiguraju da im mikroskopske čestice ne unište čip tijekom proizvodnje. Na ovom filmu možete vidjeti kako izgleda njihovo rješenje za uklanjanje sub mikroskopskih čestica.
I tu je prikazan samo prvi stupanj sustava koji osigurava sub mikroskopsku čistoću. Taj sustav služi da bi dovoljno očistio zrak kako bi drugi stupanj koji ga još više pročisti mogao funkcionirati. Drugi dio sustava se sastoji od kontejnera u kojem se transportiraju čipovi. Oni su u potpunosti bez sub mikroskopskih čestica.
Nakon ovoga postavlja se pitanje kako oni koji uzimaju uzorke za PCR analizu osiguravaju da se uzorak ne kontaminiraju? Oni uzorke uzimaju na parkiralištu a da osoba uopće ne treba izaći iz automobila dok se uzorka uzima? Cijelu pripremu uzoraka prije stavljanja u PCR mašinu rade u labosima koji nemaju čistoći čiste sobe za proizvodnju čipova? Kada bi se tak moglo osigurati da se uzorka ne kontaminira submikronskim česticama onda bi tako radili i proizvođači mikro čipova i uštedjeli bi značajno svoj proizvodni proces a samim time i svoj proizvod.
Iz toga možemo zaključiti da nije isključeno da PCR test bude pozitivan zato što se uzorak kontaminirao sa genetskim materijalom iz zraka sa nekim od 99% virusa koji još nisu otkriveni a koji imaju 60-tak baza koje ima i tast za Sars-cov-2.
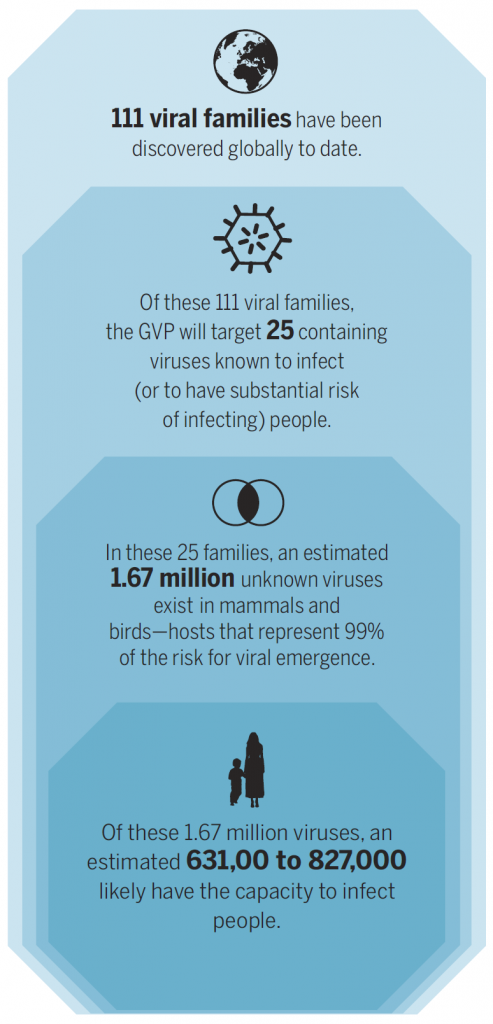
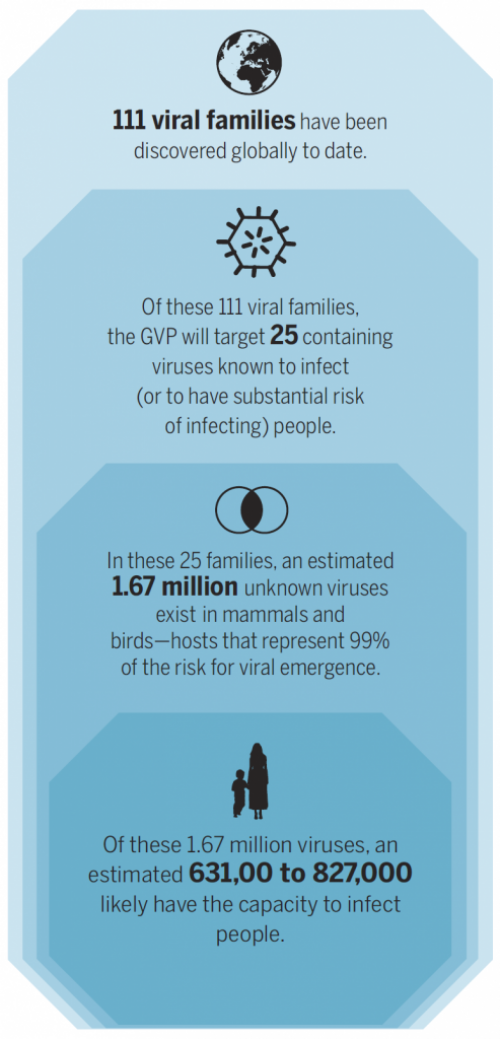
2. Do danas je otkriveno 111 porodica virusa. Od tih 111 porodica 25 je pronađeno u ljudima. U samo tih 25 porodica pretpostavlja se da se u sisavcima i pticama nalazi neotkrivenih 1.67 milijuna virusa. Global virome project si je dao za zadatak da katalogizira te dosad neotkrivene viruse. https://science.sciencemag.org/content/359/6378/872.full
Ako je toliko puno virusa u sisavcima neotkriveno i ne znamo njihov genetski kod kako možemo biti sigurni da on ne sadrži onih 60 baza koje traži PCR test kod detekcije Sars-cov-2?
3. In the human holobiont, the 1013 human cells are outnumbered 10-fold by bacteria and 100-fold by viruses. https://www.sciencedirect.com/science/article/pii/S1879625711001908
It has been estimated that there are over 380 trillion viruses inhabiting us, a community collectively known as the human virome.https://www.inverse.com/article/49747-what-is-the-human-virome
U prosječnom čovjeku nalazi se 10 puta više bakterija i 100 puta više virusa nego ljudskih stanica. Procjenjuje se da se u prosječnom čovjeku nalazi 0.4*10^15 virusa. To je otprilike 100 000 puta više nego što je trenutno ljudi na planeti. Kako je netko isključio da niti jedan od 0.4*10^15 virusa i niti jedna od 0.4*10^14 bakterija nema tih 60-tak baza koje se koriste u testa za Sars-Cov-2 kada još uvijek ne znamo slijed baza svih tih virusa i bakterija
4. Although the human genome has been completely sequenced for some practical purposes, there are still hundreds of gaps in the sequence and an uncertainty of about 5–10% (300 million basepairs added in 2018).[26] A study, published in 2015, noted more than 160 euchromatic gaps of which 50 gaps were closed.[27] However, there are still numerous gaps in the heterochromatic parts of the genome which is much harder to sequence due to numerous repeats and other intractable sequence features. https://en.wikipedia.org/wiki/Human_genome
Iako su neki proglasili da smo u potpunosti sekvencirali genom jednog čovjeka to nije točno. U njegovoj sekvenci još uvijek postoji mnoge praznine. Samo je u 2018 nadodano 300 miliona parova baza. Na koji način netko može osigurati da 60-tak baza na koje se vrši test nisu i negdje i u još uvijek ne sekvenciranom dijelu DNA tog čovjeka? Osim toga svaki čovjek ima drugačiju DNA. Pa čak i ako taj jedan čovjek kojem još nismo do kraja sekvencirali DNA ne posjeduje tih 60-tak baza, kako možemo biti sigurni da drugi ljudi čiji genom nismo sekvencirali nemaju tih 60-tak baza u svom genomu.
5. Čak i da se doista genetski materijal virusa nalazi na štapiću za uzimanje brisa postavlja se pitanje da li je on došao iz osobe kojoj je bris uzet ili iz zraka? Kada je proglašena panedmija i obaveza nošenja maski možemo pretpostaviti da tog virusa u zraku ima u izobilju. A to znači da se virus na štapić za bris mogao zakačiti dok se taj štapić nalazio na zraku.
6. PCR test detektira fragmente genetskog materijala a ne prisustvo cijelog virusa. Tako da čak i da je test ispravno pozitivan i da je genetski materijal došao iz brisa pacijenta to još ne znači da je taj virus bio funkcionalan u pacijentu. Možda je imuni sustav pacijenta neutralizirao virus i sada se fragmenti tog virusa nalaze u tom zdravom čovjeku te ih on putem sekreta izbacuje van.
7. Na pakiranju seta za testiranje i sam CDC kaže da oni ne mogu osigurati da primeri stvarno i imaju tu sekvencu koju su naveli:“ Every effort has been made to assure the accuracy of the sequences, but CDC cannot provide any warranty regarding their accuracy. „
Zbog toga je upitno i ono što smo do sada uzimali da nije. Upitna je sekvenca primera koju ste dobili kada ste kupili set za testiranje
8. U svojoj objavio Srećko Sladoljev je opisao kako je Imunološki zavod za testiranje prisustva virusa hepatitisa C metodom PCR vršio validaciju 3 godine. https://www.facebook.com/sladoljev.srecko/posts/3314283395268576
Te tri godine su u Imunološkom zavodu stalno dobivali pozitivni rezultat na prisustvo virusa hepatitisa C u doniranoj krvi za proizvodnju interferona. Tri godine je trajala validacija testa i 3 godine su dobivani lažno pozitivan rezultat. To govori o tome koliko je i samo uzimanje uzoraka podložno davanju lažno pozitivnih rezultata. Kao kuriozitet navodim da je tada dr. Markotić bila voditeljica kontrole interferona. U 3 godine dr. Markotić nije uspjela napraviti da test na hepatitis C iz krvi, ne daje lažno pozitivne rezultate, a sada bi trebali vjerovati da je u par mjeseci dr. Markotić uspjela validirati test na Sars-Cov-2 u ljudi, što je mnogo kompliciraniji test nego test na hepatitis C iz krvi, i da test ne daje lažno pozitivne rezultate
9. Moglo bi se još mnogo točaka napisati koji govore o (ne) točnosti PCR testa da detektira virus ali zaustaviti ću se i dati viđenje čovjeka koji je izmislio PCR test Kary Mullisa i za to dobio nobelovu nagradu:“ In the early 1990’s, PCR, came into popular use, and Kary Mullis was awarded the Nobel Prize for it in 1993. PCR, simply put, is a thermal cycling method used to make up to billions of copies of a specific DNA sample, making it large enough to study. PCR is an indispensable technique with a broad variety of applications including biomedical research and criminal forensics.” According to Mullis himself, PCR cannot be totally and should never be used as a tool in “the diagnosis of infectious diseases.”
Izumitelj PCR metode kaže da se PCR ne bi trebao nikada koristiti u dijagnozi zaraznih bolesti.
*
Dvom v uporabnost PCR testa dokazuje tudi raziskava, ki jo je ameriški Center za nadzor bolezni objavil junija 2020: https://wwwnc.cdc.gov/eid/article/26/6/20-0516_article
Kot razlaga dr. Tom Cowan je bila ta študija izvedena na podlagi vzorca virusov, ki so jih pridobili iz bolnika in za katere so s PCR testom na podlagi 37 nukleotidov ugotovili, da naj bi šlo za vzorec koronavirusov SARS CoV-2. S tem so okužili linije človeških in živalskih celic (človeške adenokarcinoma celice A549, celice človeških jeter HUH 7.0, celice ledvic človeškega fetusa HEK 293T, celice ledvic opice Vero 6E in Vero CCL81). Ugotovili so, da so se domnevni SARS CoV-2 lahko replicirali samo v celicah opičjih ledvic in ne v človeških celicah, kar naj bi pomenilo, da SARS CoV-2 ne more okužiti človeških celic. Prav tako so se replicirali v opičjih celicah le, ko so dodali dvoje toksičnih zdravil za ledvice (gentamicin in amfotericin). Če bi bilo tako, da domnevni koronavirusi SARS CoV-2 iz vzorca bolnika niso mogli okužiti človeških celic, potem epidemija COVID-19 ne obstaja. Bolj verjetno pa je, da je PCR test neuporaben, kot kažejo dokumenti v tej objavi ter da znanstveniki iz bolnika sploh niso pridobili vzorca koronavirusa SARS CoV-2. Zaključek študije je, da koronavirus SARS CoV-2 lahko vzgjajo samo v Vero celicah opic. Vir: https://drtomcowan.com/only-poisoned-monkey-kidney-cells-grew-the-virus/
* * *
vzorci znotraj človeških celic, ampkaDr. Srećko Sladoljev: “Vjerodostojnost RT-PCRa testa, metode kojom se ljudima globalno „pumpaju“ glave panikom i strahom od smrti”
Autor: dr. Srećko Sladoljev
U objavi ću upozoriti na vjerodostojnost RT-PCRa, metode kojom se ljudima globalno „pumpaju“ glave panikom i strahom od smrti. Pogrešno interpretirajući rezultate RT-PCR testa, Imunološki zavod je još prije dvadesetak godina globalno zazivao bojkot svog najperspektivnijeg proizvoda – prirodnog leukocitnog nativnog interferona. Objaviti ću sramotu da provjerimo da li je Dubokoj državi svaka istina „kršenje standarda zajednice“?
Covid gripa, to znaju i vrtićka djeca, „dokazuje“ se RT-PCR-om, i najosjetljivijim i najnepouzdanijem testom istovremeno. Dovoljno je da u uzorak zaluta mikroskopska čestica kože da test možda pođe ukrivo. Zbog toga će vam „prekjučer“ „dokazati“ da imate Covid i strpati s kovidašima, danas ga nećete imati, a sutra je opet tu (jer ste ga pokupili od kovidaša). Mogu dati i podatke.
Ne tvrdim, ali moguće da sam prvi u svijetu JAVNO osporio istinitost rezultata dobivenih RT-PCR testom koji su objavljeni u znanstvenom radu, u “evidence based”. Objasnio sam i gdje se pogriješilo. Iako sam bio u pravu (jer je WHO je kratko nakon toga promijenio naputak za izvođenje testa!), dobio sam zbog toga i prvo upozorenje iz radnog odnosa. bilo je to prije dvadesetak godina. Idemo red
Imunološki zavod uveo je RT-PCR za otkrivanje virusa hepatitisa C (HCV) u doniranoj krvi 1996.g., dvije godine prije preporuke WHO-a. U prilogu 1. rezultati su RT-PCRa na HCV od 1997. do 2002. g. (u proizvodnji interferona koriste se ljudski leukociti!). Crveno su HCV pozitivne, a plavo HCV negativne serije. Do sredine 1998. sve su serije (uglavnom) bile pozitivne, a od sredine 1998., kada sam i preuzeo proizvodnju, sve su bile (uglavnom) negativne.
U dopisu direktoru od 8.9.1998., ukazujem na 4 slaba mjesta proizvodnog postupka, među njima i „neadekvatno sakupljanje i transport leukomase“ što se kasnije pokazalo preduvjetom ispravnog izvođenja testa i vjerodostojnosti RT-PCR rezultata (prilog 3)!
Po uvedenim izmjenama, proizvodnja je krenula već krajem 1998. Desilo se „čudo“! Nije se dugo čekalo na „intervenciju“ predstojnice Finalne kontrole (čije su „aktivnosti“ i dovele do gašenja proizvodnje!), cit. „Ne dvojim da ste u stanju poboljšati proizvodni postupak za pripravu HAS-a, virusa induktora, primera i gotovog proizvoda, no važeći Vas zakoni obvezuju da u pismenoj formi Odjelu za kontrolu kvalitete obrazložite svaku promjenu proizvodnog postupka bilo koje ulazne tvari ili međuproizvoda. Promjene koje ste uveli tijekom proizvodnje serije 1138 su ozbiljne promjene……“ …. , „Vaš prigovor o neupućenosti Vaših ljudi u zahtjeve pri uzorkovanju (za RT-PCR) neosnovan je. Osobno sam održala dva sastanka na temu ispitivanja HCV-RNA pomoću RT-PCR s Vašim ljudima, no to je bilo prije Vašeg dolaska na tu dužnost.“ (prilozi 4 i 5).
18.2.1999. stiže odgovor predstojnice, „Bojim se da Vaše iskustvo u izvođenju RT-PCR za HCV RNA nije dovoljno da biste mogli argumentirano inzistirati na promjenama uspostavljenog sustava. U Imunološkom zavodu je uspostava in-house RT-PCR za HCV RNA i validacija istog trajala je tri godine (obzirom na Vaše osobno iskustvo u rekonstrukciji postojeće proizvodnje, uzmite u obzir da prije toga nije bilo molekularne biologije u Imunološkom zavodu). Kroz to su vrijeme suradnici Odsjeka za molekularnu biomedicinu sudjelovali u kolaborativnoj studiji na europskoj razini (Viral Qaulity Control ….. etc.) …..
….“ Rado ću s Vama raspraviti Vaše teorije KADA ONE DOBIJU EKSPERIMENTALNU POTVRDU. U međuvremenu Vas uvjeravam da je RT-PCR vrlo skup test te da Imunološki zavod u ovom trenutku nema dovoljno sredstava za nedovoljno obrazožene eksperimente, odnosno prijedloge eksperimenata koji nemaju ZADOVOLJAVAJUĆU ZNANSTVENU POTPORU.“
Niti riječi na činjenicu da je proizvodnja nakon dvije godine krenula i to BEZ virusa hepatitisa? I nije točno da „prije toga nije bilo molekulske biologije na Imunološkom zavodu“. Započeo sam kao voditelj Laboratorija za molekulsku biofiziku. A to je još “sofisticiranije”.
Niz HCV negativnih serija interferona prekinule su tri pozitivne. Internom istragom shvatili smo da je došlo do propusta u postupku prikupljanja i transporta leukocita zbog čega je u proizvodni postupak i testiranje dospjelo neuobičajeno mnogo mrtvih stanica. Desilo se čega sam se pribojavao. Iako sam UNAPRIJED upozorio Kontrolu da bi serije radi interferencije s humanim nukleinskim kiselinama mogle biti HCV pozitivne (!), Kontrola se žuri objaviti znanstveni rad radi vlastite znanstvene promičbene ne mareći što teško kompromitira Imunološki zavod, cit. “The aim of this study was to determine the rate of HCV RNA positive batches of human native leukocyte interferon during large-scale production. Our findings indicate the presence of HCV RNA in 6,1% batches despite acidification of intermediates in order to inactivate Sendai virus.“
Agencija za lijekove Hrvatske uvodi posebne mjere nadzora i zaustavlja proizvodnju.
S kolegama, dr Toothom iz Mađarske i dr Filipičem iz Slovenije, sastavljama i šaljemo Pismo urednicima (Letter to the Editors) pod naslovom “On the responsibility and ethics of scientific contribution” kojim osporavamo vjerodostojnost objavljenog rada! Isključujem se kao supotpisnik da tvrtku ne bih izvrgao većem ruglu.
Interveniram i kod ravnateljice Hrvatskog zavoda za kontrolu imunobioloških preparata. Vjeruju mi i vraćaju proizvodnju.
14.6.2004. nakon podvala na granici kriminala (podmetanje krađe iza koje je mogla stajati jedino Uprava!), ova me obavještava da je protiv mene pokrenula Postupak prije otkazivanja ugovora o radu.
Otkaz je i otpravljen, ali nije realiziran jer je Nadzorni odbor desetak minuta prije uručenja smijenio Upravu zbog štetnih radnji.
Svjetska zdravstvena organizacija (WHO) kratko nakon toga izdala je nove preporuke za izvođenje RT-PCR na uzorcima iz ljudske krvi. Ako je od uzimanja do testiranja uzoraka prošlo više od dva sata, rezultati nisu bili vjerodostojni.
Dva znanstvena rada rada potvrdila su kako nukleinske kiseline ljudi kompromitiraju test dajući LAŽNO POZITIVNE rezultate.
Ne trebate mnogo mašte da zamislite što je s uzorcima za testiranje Covida RT-PCR testom? Zamislite koliko je tek MRTVIH STANICA u ispljuvku prehlađenih i gripoznih!
*
Your Coronavirus Test Is Positive. Maybe It Shouldn’t Be.
The usual diagnostic tests may simply be too sensitive and too slow to contain the spread of the virus.
https://www.nytimes.com/2020/08/29/health/coronavirus-testing.html
Tests authorized by the F.D.A. provide only a yes-no answer to infection, and will identify as positive patients with low amounts of virus in their bodies.
Some of the nation’s leading public health experts are raising a new concern in the endless debate over coronavirus testing in the United States: The standard tests are diagnosing huge numbers of people who may be carrying relatively insignificant amounts of the virus.
Most of these people are not likely to be contagious, and identifying them may contribute to bottlenecks that prevent those who are contagious from being found in time. But researchers say the solution is not to test less, or to skip testing people without symptoms, as recently suggested by the Centers for Disease Control and Prevention.
Instead, new data underscore the need for more widespread use of rapid tests, even if they are less sensitive.
“The decision not to test asymptomatic people is just really backward,” said Dr. Michael Mina, an epidemiologist at the Harvard T.H. Chan School of Public Health, referring to the C.D.C. recommendation.
“In fact, we should be ramping up testing of all different people,” he said, “but we have to do it through whole different mechanisms.”
In what may be a step in this direction, the Trump administration announced on Thursday that it would purchase 150 million rapid tests.
The most widely used diagnostic test for the new coronavirus, called a PCR test, provides a simple yes-no answer to the question of whether a patient is infected.
But similar PCR tests for other viruses do offer some sense of how contagious an infected patient may be: The results may include a rough estimate of the amount of virus in the patient’s body.
“We’ve been using one type of data for everything, and that is just plus or minus — that’s all,” Dr. Mina said. “We’re using that for clinical diagnostics, for public health, for policy decision-making.”
But yes-no isn’t good enough, he added. It’s the amount of virus that should dictate the infected patient’s next steps. “It’s really irresponsible, I think, to forgo the recognition that this is a quantitative issue,” Dr. Mina said.
The PCR test amplifies genetic matter from the virus in cycles; the fewer cycles required, the greater the amount of virus, or viral load, in the sample. The greater the viral load, the more likely the patient is to be contagious.
This number of amplification cycles needed to find the virus, called the cycle threshold, is never included in the results sent to doctors and coronavirus patients, although it could tell them how infectious the patients are.
In three sets of testing data that include cycle thresholds, compiled by officials in Massachusetts, New York and Nevada, up to 90 percent of people testing positive carried barely any virus, a review by The Times found.
On Thursday, the United States recorded 45,604 new coronavirus cases, according to a database maintained by The Times. If the rates of contagiousness in Massachusetts and New York were to apply nationwide, then perhaps only 4,500 of those people may actually need to isolate and submit to contact tracing.
One solution would be to adjust the cycle threshold used now to decide that a patient is infected. Most tests set the limit at 40, a few at 37. This means that you are positive for the coronavirus if the test process required up to 40 cycles, or 37, to detect the virus.
Tests with thresholds so high may detect not just live virus but also genetic fragments, leftovers from infection that pose no particular risk — akin to finding a hair in a room long after a person has left, Dr. Mina said.
Any test with a cycle threshold above 35 is too sensitive, agreed Juliet Morrison, a virologist at the University of California, Riverside. “I’m shocked that people would think that 40 could represent a positive,” she said.
A more reasonable cutoff would be 30 to 35, she added. Dr. Mina said he would set the figure at 30, or even less. Those changes would mean the amount of genetic material in a patient’s sample would have to be 100-fold to 1,000-fold that of the current standard for the test to return a positive result — at least, one worth acting on
*
Lockdowns and hygienic measures around the world are based on numbers of cases and mortality rates created by the so-called SARS-CoV-2 RT-PCR tests used to identify “positive” patients, whereby “positive” is usually equated with “infected.”
But looking closely at the facts, the conclusion is that these PCR tests are meaningless as a diagnostic tool to determine an alleged infection by a supposedly new virus called SARS-CoV-2.
UNFOUNDED “TEST, TEST, TEST,…” MANTRA
At the media briefing on COVID-19 on March 16, 2020, the WHO Director General Dr Tedros Adhanom Ghebreyesus said:
We have a simple message for all countries: test, test, test.”
The message was spread through headlines around the world, for instance by Reuters and the BBC.
Still on the 3 of May, the moderator of the heute journal — one of the most important news magazines on German television— was passing the mantra of the corona dogma on to his audience with the admonishing words:
Test, test, test—that is the credo at the moment, and it is the only way to really understand how much the coronavirus is spreading.”
This indicates that the belief in the validity of the PCR tests is so strong that it equals a religion that tolerates virtually no contradiction.
But it is well known that religions are about faith and not about scientific facts. And as Walter Lippmann, the two-time Pulitzer Prize winner and perhaps the most influential journalist of the 20th century said: “Where all think alike, no one thinks very much.”
So to start, it is very remarkable that Kary Mullis himself, the inventor of the Polymerase Chain Reaction (PCR) technology, did not think alike. His invention got him the Nobel prize in chemistry in 1993.
Unfortunately, Mullis passed away last year at the age of 74, but there is no doubt that the biochemist regarded the PCR as inappropriate to detect a viral infection.
The reason is that the intended use of the PCR was, and still is, to apply it as a manufacturing technique, being able to replicate DNA sequences millions and billions of times, and not as a diagnostic tool to detect viruses.
How declaring virus pandemics based on PCR tests can end in disaster was described by Gina Kolata in her 2007 New York Times article Faith in Quick Test Leads to Epidemic That Wasn’t.
LACK OF A VALID GOLD STANDARD
Moreover, it is worth mentioning that the PCR tests used to identify so-called COVID-19 patients presumably infected by what is called SARS-CoV-2 do not have a valid gold standard to compare them with.
This is a fundamental point. Tests need to be evaluated to determine their preciseness — strictly speaking their “sensitivity”[1] and “specificity” — by comparison with a “gold standard,” meaning the most accurate method available.
As an example, for a pregnancy test the gold standard would be the pregnancy itself. But as Australian infectious diseases specialist Sanjaya Senanayake, for example, stated in an ABC TV interview in an answer to the question “How accurate is the [COVID-19] testing?”:
If we had a new test for picking up [the bacterium] golden staph in blood, we’ve already got blood cultures, that’s our gold standard we’ve been using for decades, and we could match this new test against that. But for COVID-19 we don’t have a gold standard test.”
Jessica C. Watson from Bristol University confirms this. In her paper “Interpreting a COVID-19 test result”, published recently in The British Medical Journal, she writes that there is a “lack of such a clear-cut ‘gold-standard’ for COVID-19 testing.”
But instead of classifying the tests as unsuitable for SARS-CoV-2 detection and COVID-19 diagnosis, or instead of pointing out that only a virus, proven through isolation and purification, can be a solid gold standard, Watson claims in all seriousness that, “pragmatically” COVID-19 diagnosis itself, remarkably including PCR testing itself, “may be the best available ‘gold standard’.” But this is not scientifically sound.
Apart from the fact that it is downright absurd to take the PCR test itself as part of the gold standard to evaluate the PCR test, there are no distinctive specific symptoms for COVID-19, as even people such as Thomas Löscher, former head of the Department of Infection and Tropical Medicine at the University of Munich and member of the Federal Association of German Internists, conceded to us[2].
And if there are no distinctive specific symptoms for COVID-19, COVID-19 diagnosis — contrary to Watson’s statement — cannot be suitable for serving as a valid gold standard.
In addition, “experts” such as Watson overlook the fact that only virus isolation, i.e. an unequivocal virus proof, can be the gold standard.
That is why I asked Watson how COVID-19 diagnosis “may be the best available gold standard,” if there are no distinctive specific symptoms for COVID-19, and also whether the virus itself, that is virus isolation, wouldn’t be the best available/possible gold standard. But she hasn’t answered these questions yet – despite multiple requests. And she has not yet responded to our rapid response post on her article in which we address exactly the same points, either, though she wrote us on June 2nd: “I will try to post a reply later this week when I have a chance.”
NO PROOF FOR THE RNA BEING OF VIRAL ORIGIN
Now the question is: What is required first for virus isolation/proof? We need to know where the RNA for which the PCR tests are calibrated comes from.
As textbooks (e.g., White/Fenner. Medical Virology, 1986, p. 9) as well as leading virus researchers such as Luc Montagnier or Dominic Dwyer state, particle purification — i.e. the separation of an object from everything else that is not that object, as for instance Nobel laureate Marie Curie purified 100 mg of radium chloride in 1898 by extracting it from tons of pitchblende — is an essential pre-requisite for proving the existence of a virus, and thus to prove that the RNA from the particle in question comes from a new virus.
The reason for this is that PCR is extremely sensitive, which means it can detect even the smallest pieces of DNA or RNA — but it cannot determine where these particles came from. That has to be determined beforehand.
And because the PCR tests are calibrated for gene sequences (in this case RNA sequences because SARS-CoV-2 is believed to be a RNA virus), we have to know that these gene snippets are part of the looked-for virus. And to know that, correct isolation and purification of the presumed virus has to be executed.
Hence, we have asked the science teams of the relevant papers which are referred to in the context of SARS-CoV-2 for proof whether the electron-microscopic shots depicted in their in vitro experiments show purified viruses.
But not a single team could answer that question with “yes” — and NB., nobody said purification was not a necessary step. We only got answers like “No, we did not obtain an electron micrograph showing the degree of purification” (see below).
We asked several study authors “Do your electron micrographs show the purified virus?”, they gave the following responses:
Study 1: Leo L. M. Poon; Malik Peiris. “Emergence of a novel human coronavirus threatening human health” Nature Medicine, March 2020
Replying Author: Malik Peiris
Date: May 12, 2020
Answer: “The image is the virus budding from an infected cell. It is not purified virus.”
Study 2: Myung-Guk Han et al. “Identification of Coronavirus Isolated from a Patient in Korea with COVID-19”, Osong Public Health and Research Perspectives, February 2020
Replying Author: Myung-Guk Han
Date: May 6, 2020
Answer: “We could not estimate the degree of purification because we do not purify and concentrate the virus cultured in cells.”
Study 3: Wan Beom Park et al. “Virus Isolation from the First Patient with SARS-CoV-2 in Korea”, Journal of Korean Medical Science, February 24, 2020
Replying Author: Wan Beom Park
Date: March 19, 2020
Answer: “We did not obtain an electron micrograph showing the degree of purification.”
Study 4: Na Zhu et al., “A Novel Coronavirus from Patients with Pneumonia in China”, 2019, New England Journal of Medicine, February 20, 2020
Replying Author: Wenjie Tan
Date: March 18, 2020
Answer: “[We show] an image of sedimented virus particles, not purified ones.”
Regarding the mentioned papers it is clear that what is shown in the electron micrographs (EMs) is the end result of the experiment, meaning there is no other result that they could have made EMs from.
That is to say, if the authors of these studies concede that their published EMs do not show purified particles, then they definitely do not possess purified particles claimed to be viral. (In this context, it has to be remarked that some researchers use the term “isolation” in their papers, but the procedures described therein do not represent a proper isolation (purification) process. Consequently, in this context the term “isolation” is misused).
Thus, the authors of four of the principal, early 2020 papers claiming discovery of a new coronavirus concede they had no proof that the origin of the virus genome was viral-like particles or cellular debris, pure or impure, or particles of any kind. In other words, the existence of SARS-CoV-2 RNA is based on faith, not fact.
We have also contacted Dr Charles Calisher, who is a seasoned virologist. In 2001, Science published an “impassioned plea…to the younger generation” from several veteran virologists, among them Calisher, saying that:
[modern virus detection methods like] sleek polymerase chain reaction […] tell little or nothing about how a virus multiplies, which animals carry it, [or] how it makes people sick. [It is] like trying to say whether somebody has bad breath by looking at his fingerprint.”[3]
And that’s why we asked Dr Calisher whether he knows one single paper in which SARS-CoV-2 has been isolated and finally really purified. His answer:
I know of no such a publication. I have kept an eye out for one.”[4]
This actually means that one cannot conclude that the RNA gene sequences, which the scientists took from the tissue samples prepared in the mentioned in vitro trials and for which the PCR tests are finally being “calibrated,” belong to a specific virus — in this case SARS-CoV-2.
In addition, there is no scientific proof that those RNA sequences are the causative agent of what is called COVID-19.
In order to establish a causal connection, one way or the other, i.e. beyond virus isolation and purification, it would have been absolutely necessary to carry out an experiment that satisfies the four Koch’s postulates. But there is no such experiment, as Amory Devereux and Rosemary Frei recently revealed for OffGuardian.
The necessity to fulfill these postulates regarding SARS-CoV-2 is demonstrated not least by the fact that attempts have been made to fulfill them. But even researchers claiming they have done it, in reality, did not succeed.
One example is a study published in Nature on May 7. This trial, besides other procedures which render the study invalid, did not meet any of the postulates.
For instance, the alleged “infected” laboratory mice did not show any relevant clinical symptoms clearly attributable to pneumonia, which according to the third postulate should actually occur if a dangerous and potentially deadly virus was really at work there. And the slight bristles and weight loss, which were observed temporarily in the animals are negligible, not only because they could have been caused by the procedure itself, but also because the weight went back to normal again.
Also, no animal died except those they killed to perform the autopsies. And let’s not forget: These experiments should have been done before developing a test, which is not the case.
Revealingly, none of the leading German representatives of the official theory about SARS-Cov-2/COVID-19 — the Robert Koch-Institute (RKI), Alexander S. Kekulé (University of Halle), Hartmut Hengel and Ralf Bartenschlager (German Society for Virology), the aforementioned Thomas Löscher, Ulrich Dirnagl (Charité Berlin) or Georg Bornkamm (virologist and professor emeritus at the Helmholtz-Zentrum Munich) — could answer the following question I have sent them:
If the particles that are claimed to be to be SARS-CoV-2 have not been purified, how do you want to be sure that the RNA gene sequences of these particles belong to a specific new virus?
Particularly, if there are studies showing that substances such as antibiotics that are added to the test tubes in the in vitro experiments carried out for virus detection can “stress” the cell culture in a way that new gene sequences are being formed that were not previously detectable — an aspect that Nobel laureate Barbara McClintock already drew attention to in her Nobel Lecture back in 1983.
It should not go unmentioned that we finally got the Charité – the employer of Christian Drosten, Germany’s most influential virologist in respect of COVID-19, advisor to the German government and co-developer of the PCR test which was the first to be “accepted” (not validated!) by the WHO worldwide – to answer questions on the topic.
But we didn’t get answers until June 18, 2020, after months of non-response. In the end, we achieved it only with the help of Berlin lawyer Viviane Fischer.
Regarding our question “Has the Charité convinced itself that appropriate particle purification was carried out?,” the Charité concedes that they didn’t use purified particles.
And although they claim “virologists at the Charité are sure that they are testing for the virus,” in their paper (Corman et al.) they state:
RNA was extracted from clinical samples with the MagNA Pure 96 system (Roche, Penzberg, Germany) and from cell culture supernatants with the viral RNA mini kit (QIAGEN, Hilden, Germany),”
Which means they just assumed the RNA was viral.
Incidentally, the Corman et al. paper, published on January 23, 2020 didn’t even go through a proper peer review process, nor were the procedures outlined therein accompanied by controls — although it is only through these two things that scientific work becomes really solid.
IRRATIONAL TEST RESULTS
It is also certain that we cannot know the false positive rate of the PCR tests without widespread testing of people who certainly do not have the virus, proven by a method which is independent of the test (having a solid gold standard).
Therefore, it is hardly surprising that there are several papers illustrating irrational test results.
For example, already in February the health authority in China’s Guangdong province reported that people have fully recovered from illness blamed on COVID-19, started to test “negative,” and then tested “positive” again.
A month later, a paper published in the Journal of Medical Virology showed that 29 out of 610 patients at a hospital in Wuhan had 3 to 6 test results that flipped between “negative”, “positive” and “dubious”.
A third example is a study from Singapore in which tests were carried out almost daily on 18 patients and the majority went from “positive” to “negative” back to “positive” at least once, and up to five times in one patient.
Even Wang Chen, president of the Chinese Academy of Medical Sciences, conceded in February that the PCR tests are “only 30 to 50 per cent accurate”; while Sin Hang Lee from the Milford Molecular Diagnostics Laboratory sent a letter to the WHO’s coronavirus response team and to Anthony S. Fauci on March 22, 2020, saying that:
It has been widely reported in the social media that the RT-qPCR [Reverse Transcriptase quantitative PCR] test kits used to detect SARSCoV-2 RNA in human specimens are generating many false positive results and are not sensitive enough to detect some real positive cases.”
In other words, even if we theoretically assume that these PCR tests can really detect a viral infection, the tests would be practically worthless, and would only cause an unfounded scare among the “positive” people tested.
This becomes also evident considering the positive predictive value (PPV).
The PPV indicates the probability that a person with a positive test result is truly “positive” (ie. has the supposed virus), and it depends on two factors: the prevalence of the virus in the general population and the specificity of the test, that is the percentage of people without disease in whom the test is correctly “negative” (a test with a specificity of 95% incorrectly gives a positive result in 5 out of 100 non-infected people).
With the same specificity, the higher the prevalence, the higher the PPV.
In this context, on June 12 2020, the journal Deutsches Ärzteblatt published an article in which the PPV has been calculated with three different prevalence scenarios.
The results must, of course, be viewed very critically, first because it is not possible to calculate the specificity without a solid gold standard, as outlined, and second because the calculations in the article are based on the specificity determined in the study by Jessica Watson, which is potentially worthless, as also mentioned.
But if you abstract from it, assuming that the underlying specificity of 95% is correct and that we know the prevalence, even the mainstream medical journal Deutsches Ärzteblatt reports that the so-called SARS-CoV-2 RT-PCR tests may have “a shockingly low” PPV.
In one of the three scenarios, figuring with an assumed prevalence of 3%, the PPV was only 30 percent, which means that 70 percent of the people tested “positive” are not “positive” at all. Yet “they are prescribed quarantine,” as even the Ärzteblatt notes critically.
In a second scenario of the journal’s article, a prevalence of rate of 20 percent is assumed. In this case they generate a PPV of 78 percent, meaning that 22 percent of the “positive” tests are false “positives.”
That would mean: If we take the around 9 million people who are currently considered “positive” worldwide — supposing that the true “positives” really have a viral infection — we would get almost 2 million false “positives.”
All this fits with the fact that the CDC and the FDA, for instance, concede in their files that the so-called “SARS-CoV-2 RT-PCR tests” are not suitable for SARS-CoV-2 diagnosis.
In the “CDC 2019-Novel Coronavirus (2019-nCoV) Real-Time RT-PCR Diagnostic Panel“ file from March 30, 2020, for example, it says:
Detection of viral RNA may not indicate the presence of infectious virus or that 2019-nCoV is the causative agent for clinical symptoms”
And:
This test cannot rule out diseases caused by other bacterial or viral pathogens.”
And the FDA admits that:
positive results […] do not rule out bacterial infection or co-infection with other viruses. The agent detected may not be the definite cause of disease.”
Remarkably, in the instruction manuals of PCR tests we can also read that they are not intended as a diagnostic test, as for instance in those by Altona Diagnostics and Creative Diagnostics[5].
To quote another one, in the product announcement of the LightMix Modular Assays produced by TIB Molbiol — which were developed using the Corman et al. protocol — and distributed by Roche we can read:
These assays are not intended for use as an aid in the diagnosis of coronavirus infection”
And:
For research use only. Not for use in diagnostic procedures.”
WHERE IS THE EVIDENCE THAT THE TESTS CAN MEASURE THE “VIRAL LOAD”?
There is also reason to conclude that the PCR test from Roche and others cannot even detect the targeted genes.
Moreover, in the product descriptions of the RT-qPCR tests for SARS-COV-2 it says they are “qualitative” tests, contrary to the fact that the “q” in “qPCR” stands for “quantitative.” And if these tests are not “quantitative” tests, they don’t show how many viral particles are in the body.
That is crucial because, in order to even begin talking about actual illness in the real world not only in a laboratory, the patient would need to have millions and millions of viral particles actively replicating in their body.
That is to say, the CDC, the WHO, the FDA or the RKI may assert that the tests can measure the so-called “viral load,” i.e. how many viral particles are in the body. “But this has never been proven. That is an enormous scandal,” as the journalist Jon Rappoport points out.
This is not only because the term “viral load” is deception. If you put the question “what is viral load?” at a dinner party, people take it to mean viruses circulating in the bloodstream. They’re surprised to learn it’s actually RNA molecules.
Also, to prove beyond any doubt that the PCR can measure how much a person is “burdened” with a disease-causing virus, the following experiment would have had to be carried out (which has not yet happened):
You take, let’s say, a few hundred or even thousand people and remove tissue samples from them. Make sure the people who take the samples do not perform the test.The testers will never know who the patients are and what condition they’re in. The testers run their PCR on the tissue samples. In each case, they say which virus they found and how much of it they found. Then, for example, in patients 29, 86, 199, 272, and 293 they found a great deal of what they claim is a virus. Now we un-blind those patients. They should all be sick, because they have so much virus replicating in their bodies. But are they really sick — or are they fit as a fiddle?
With the help of the aforementioned lawyer Viviane Fischer, I finally got the Charité to also answer the question of whether the test developed by Corman et al. — the so-called “Drosten PCR test” — is a quantitative test.
But the Charité was not willing to answer this question “yes”. Instead, the Charité wrote:
If real-time RT-PCR is involved, to the knowledge of the Charité in most cases these are […] limited to qualitative detection.”
Furthermore, the “Drosten PCR test” uses the unspecific E-gene assay as preliminary assay, while the Institut Pasteur uses the same assay as confirmatory assay.
According to Corman et al., the E-gene assay is likely to detect all Asian viruses, while the other assays in both tests are supposed to be more specific for sequences labelled “SARS-CoV-2”.
Besides the questionable purpose of having either a preliminary or a confirmatory test that is likely to detect all Asian viruses, at the beginning of April the WHO changed the algorithm, recommending that from then on a test can be regarded as “positive” even if just the E-gene assay (which is likely to detect all Asian viruses!) gives a “positive” result.
This means that a confirmed unspecific test result is officially sold as specific.
That change of algorithm increased the “case” numbers. Tests using the E-gene assay are produced for example by Roche, TIB Molbiol and R-Biopharm.
HIGH CQ VALUES MAKE THE TEST RESULTS EVEN MORE MEANINGLESS
Another essential problem is that many PCR tests have a “cycle quantification” (Cq) value of over 35, and some, including the “Drosten PCR test”, even have a Cq of 45.
The Cq value specifies how many cycles of DNA replication are required to detect a real signal from biological samples.
“Cq values higher than 40 are suspect because of the implied low efficiency and generally should not be reported,” as it says in the MIQE guidelines.
MIQE stands for “Minimum Information for Publication of Quantitative Real-Time PCR Experiments”, a set of guidelines that describe the minimum information necessary for evaluating publications on Real-Time PCR, also called quantitative PCR, or qPCR.
The inventor himself, Kary Mullis, agreed, when he stated:
If you have to go more than 40 cycles to amplify a single-copy gene, there is something seriously wrong with your PCR.”
The MIQE guidelines have been developed under the aegis of Stephen A. Bustin, Professor of Molecular Medicine, a world-renowned expert on quantitative PCR and author of the book A-Z of Quantitative PCR which has been called “the bible of qPCR.”
In a recent podcast interview Bustin points out that “the use of such arbitrary Cq cut-offs is not ideal, because they may be either too low (eliminating valid results) or too high (increasing false “positive” results).”
And, according to him, a Cq in the 20s to 30s should be aimed at and there is concern regarding the reliability of the results for any Cq over 35.
If the Cq value gets too high, it becomes difficult to distinguish real signal from background, for example due to reactions of primers and fluorescent probes, and hence there is a higher probability of false positives.
Moreover, among other factors that can alter the result, before starting with the actual PCR, in case you are looking for presumed RNA viruses such as SARS-CoV-2, the RNA must be converted to complementary DNA (cDNA) with the enzyme Reverse Transcriptase—hence the “RT” at the beginning of “PCR” or “qPCR.”
But this transformation process is “widely recognized as inefficient and variable,” as Jessica Schwaber from the Centre for Commercialization of Regenerative Medicine in Toronto and two research colleagues pointed out in a 2019 paper.
Stephen A. Bustin acknowledges problems with PCR in a comparable way.
For example, he pointed to the problem that in the course of the conversion process (RNA to cDNA) the amount of DNA obtained with the same RNA base material can vary widely, even by a factor of 10 (see above interview).
Considering that the DNA sequences get doubled at every cycle, even a slight variation becomes magnified and can thus alter the result, annihilating the test’s reliable informative value.
So how can it be that those who claim the PCR tests are highly meaningful for so-called COVID-19 diagnosis blind out the fundamental inadequacies of these tests—even if they are confronted with questions regarding their validity?
Certainly, the apologists of the novel coronavirus hypothesis should have dealt with these questions before throwing the tests on the market and putting basically the whole world under lockdown, not least because these are questions that come to mind immediately for anyone with even a spark of scientific understanding.
Thus, the thought inevitably emerges that financial and political interests play a decisive role for this ignorance about scientific obligations. NB, the WHO, for example has financial ties with drug companies, as the British Medical Journal showed in 2010.
And experts criticize “that the notorious corruption and conflicts of interest at WHO have continued, even grown“ since then. The CDC as well, to take another big player, is obviously no better off.
Finally, the reasons and possible motives remain speculative, and many involved surely act in good faith; but the science is clear: The numbers generated by these RT-PCR tests do not in the least justify frightening people who have been tested “positive” and imposing lockdown measures that plunge countless people into poverty and despair or even drive them to suicide.
And a “positive” result may have serious consequences for the patients as well, because then all non-viral factors are excluded from the diagnosis and the patients are treated with highly toxic drugs and invasive intubations. Especially for elderly people and patients with pre-existing conditions such a treatment can be fatal, as we have outlined in the article “Fatal Therapie.”
Without doubt eventual excess mortality rates are caused by the therapy and by the lockdown measures, while the “COVID-19” death statistics comprise also patients who died of a variety of diseases, redefined as COVID-19 only because of a “positive” test result whose value could not be more doubtful.
NOTES:-
[1] Sensitivity is defined as the proportion of patients with disease in whom the test is positive; and specificity is defined as the proportion of patients without disease in whom the test is negative.
[2] E-mail from Prof. Thomas Löscher from March 6, 2020
[3] Martin Enserink. Virology. Old guard urges virologists to go back to basics, Science, July 6, 2001, p. 24
[4] E-mail from Charles Calisher from May 10, 2020
[5] Creative Diagnostics, SARS-CoV-2 Coronavirus Multiplex RT-qPCR Kit
Torsten Engelbrecht is an award-winning journalist and author from Hamburg, Germany. In 2006 he co-authored Virus-Mania with Dr Klaus Kohnlein, and in 2009 he won the German Alternate Media Award. He has also written for Rubikon, Süddeutsche Zeitung, Financial Times Deutschland and many others.
Konstantin Demeter is a freelance photographer and an independent researcher. Together with the journalist Torsten Engelbrecht he has published articles on the “COVID-19” crisis in the online magazine Rubikon, as well as contributions on the monetary system, geopolitics, and the media in Swiss Italian newspapers.
Vir: https://off-guardian.org/2020/06/27/covid19-pcr-tests-are-scientifically-meaningless/
https://www.researchgate.net/publication/341091306_False_positives_in_reverse_transcription_PCR_testing_for_SARS-CoV-2 - lažno pozitivnih do 16,7% PCR testov
Covid-19 tests may be detecting traces of DEAD virus, giving ‘false positives’ and EXAGGERATING pandemic – research
The study was carried out by experts from the University of Oxford’s Centre for Evidence-Based Medicine and the University of the West of England. It found there was a risk of “false positives” because of how Covid-19 testing is being conducted.
The scientists discovered that, despite people with Covid-19 being infectious for only around a week, one test used to detect the disease can still give a positive reading weeks after the patient has recovered.
The team examined 25 studies on the widely used polymerase chain reaction test, which is used to determine if someone has the virus in their system. The test takes a sample from a suspected Covid-19 case and uses a process that increases the amount of DNA, or genetic material, in the sample, to enable it to be examined.
The research found that the tests can amplify coronavirus genetic material that is not a viable virus and no longer capable of causing an infection.
Professor Carl Heneghan, one of the authors of the study, said there was a risk that a surge in testing across the UK was increasing the risk of this sample contamination occurring and it may explain why the number of Covid-19 cases is rising but the number of deaths is static.
“Evidence is mounting that a good proportion of ‘new’ mild cases and people re-testing positives after quarantine or discharge from hospital are not infectious, but are simply clearing harmless virus particles which their immune system has efficiently dealt with,” he wrote in The Spectator magazine.
Professor Heneghan said an “international effort” was required to avoid “the dangers of isolating non-infectious people or whole communities”.
Vir: https://www.rt.com/news/499944-coronavirus-test-dead-false-positive-exaggerate-pandemic/
* * *
Tjaša Vuzem necenzurirano FB 11.9. 2020·
Objavil je dr. Vladimir Pirnat
Spoštovana kolegica prof.dr. Bojana Beovič, spoštovana kolega Minister za zdravje dr. Tomaž Gantar in direktor NIJZ dr. Krek
Vljudno prosim za vaše cenjeno mnenje glede spodaj navedenih zaključkov, podprtih z obsežnimi evropskimi in ameriškjmi statističnimi podatki o umrljivosti z/zaradi COVID-19 in presežne umrljivosti v državah Evrope in Amerike.
1./pandemija bolezni COVID-19 v Evropi in tudi Sloveniji se je končala v začetku junija 2020, kar kažejo krivulje uradnih podatkov glede hospitaliziranih oz. umrlih oseb.
2./od junija letos dalje pa gre v Evropi za COVID-19 CASEDEMIJO - to je naraščanje števila oseb s pozitivnim PCR laboratorijskim testom, ki niso niti okuženi niti oboleli in ne prenašalci nalezljive bolezni COVID-19, temveč so bolezen COVID-19 že preboleli. Pri teh PCR pozitivnih osebah PCR test iz nosnega brisa ne potrjuje okuženosti temveč dokazuje delčke virusov, ki jih je njihov imunski sistem že uničil.
3./porast števila pozitivnih izvidov laboratorijskih testov PCR ne more biti več razlog za nadaljne restriktivne ukrepe, ki so "unicum" v zgodovini medicine.
4./zapiranje (lockdown) in drugi ukrepi za zadrževanje širjenja virusa SARS COV-2 (maske, distanciranje ljudi) bodo povzročili več umrlih oseb v jeseni in pozimi, ker so zadrževali koristno pridobivanje kolektivne imunosti čez poletje.
* * *
Prof. dr. Dolores Cahill, molekularna biologinja in imunologinja iz Irske:
https://altcensored.com/watch?v=whbxKvLEqMc
Izumitelj PCR testa je povedal, da ni primeren za ugotavljanje okužbe. Koronavirus ima okoli 29.000 nukleotidnih baz, primer testa PCR pa išče majhno število baz- 20 do 30 nukleotidov. SARS CoV iz leta 2002 ima 80% enako genetiko kot nov koronavirus SARS CoV-2. To pomeni, da imata oba virusa okoli 24.000 nukleotidov enakih. 20% genetike SARS CoV in SARS CoV-2 je enaka kot pri virusih navadnega prehlada. Če je primer za 20% genetike virusa, torej za okoli 6000 nukleotidov, ki so enaki pri virusih navadnega prehlada, pri SARS CoV in SARS CoV-2, potem lahko zaznava katerikoli koronavirus. Poleg tega koronavirus SARS CoV-2 povzroča težave samo takrat, ko je aktiven. Otroci na primer skoraj nimajo simptomov, virus se ne replicira. Koronavirusi krožijo običajno od decembra do aprila in po aprilu ne povzročajo bolezni ali simptomov. PCR test tako ugotavlja ali ima oseba v žrelu ali nosu fragmente RNA koronavirusa. To je kot bi testirali, ali je nekdo imel viruse gripe A ali B. Torej pozitiven PCR test pokaže samo to, ali ima oseba fragmente RNA virusa.
Februarja 2020 je ameriški CDC zapisal, da imajo teste iz Kitajske, ki so kontaminirani s koronavirusi, 70% testiranj v mesecu februarju 2020 je bilo kontaminiranih s koronavirusi v samem testu. Ne moremo vedeti, ali je test čist ali kontaminiran. Tudi druge države so poročale, da so imeli kontaminirane teste. Testi bi morali iti skozi 12 mesečno tesiranje, da bi bili specifični za nov koronavirus. 40% primerov navadnega prehlada pri ljudeh povzročajo koronavirusi in simptomi so kot pri gripi, a vzrok niso virusi gripe, ampak koronavirusi, ki krožijo v človeški populaciji že stotine tisoče let. Zaradi SARS CoV-2 je okoli leta 2002/2003 umrlo v 40 državah okoli 770 ljudi, od približno 7.000.000.000 ljudi (op. prev.: to je 0,11 ljudi na 1.000.000 ljudi, kar je stopnja smrtnosti 0,000011 %). To so podatki Svetovne zdravstvene organizacije. Verjetnost smrti zaradi SARS CoV je bila pred 18 leti 1 proti 8.000.000. Ob koncu sezone prehlada koronavirusov aprila 2020 je bilo 4290 smrti in WHO je razglasila pandemijo. Možnost smrti zaradi koronavirusa je bila 1 proti 1. 800.000. Na Irskem je bilo do aprila 2020 umrlih ljudi, ki so bili prej zdravi in so umrli zaradi SARS, samo 8 ljudi, pri številu prebivalcev več kot 6.500.000. To je stopnja smrtnosti 1 človek na 2.000.000 ljudi (op prev.: stopnja smrtnosti 0,00012% če je bilo 8 umrlih na 6,5 mio prebivalcev Irske).
Na splošno zaradi COVID-19 umreta 2 zdrava človeka na 1 milijon prebivalcev v svetu, kar je zelo malo in veliko več ljudi umre zaradi drugih vzrokov, zaradi lock down se je povečala revščina in samomori zaradi revščine. Torej so ekonomske posledice zaklepanja )lock down) veliko hujše od posledic koronavirusa SARS CoV-2.
PCR testi imajo po navadi dva primera (forward and reverse), od 30.000 nukleotidov koronavirusa, test PCR išče zgolj 30 nukleotidov. Če PCR test najde fragmente kakterega koli koronavirusa navadnega prehlada, ki jih potem multiplicirajo, potem ni res, kar trdi HHS, da je ta PCR test samo za korona viruse SARS CoV-2. Na trgu je veliko PCR testov in pogledati je potrebno, katero sekvenco RNA iščejo, ali je res specifična samo za koronavirus SARS CoV-2 ali tudi za katere druge koronaviruse. Pri PCR testu je več ciklusov multiplikacije v laboratoriju. Originalna matrica je RNA in potem so nukleotidi, ki so DNK (DNA). Prvi ciklus je DNK in po vsakem ciklusu se multicirajo na 4, 8, 16, 32 itd...
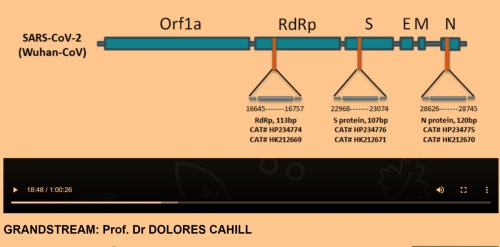
Sekvence PCR testa
Potrebno je veliko število povečanih fragmentov RNA/DNA, da se lahko zaznava okužba. Če se naredi 35 ciklusov, bodo vsi rezultati negativni, če se naredi 60 ciklusov, potem bodo vsi ljudje pozitivni na koronavirus. Zato je potrebno vedeti, koliko ciklusov PCT testa se naredi v laboratoriju. Vsekakor ta PCR test ni primeren, kajti v Južni Koreji so ljudje, ki so preboleli koronavirus, so bili pozitivni na testu, ker je pokazal, da imajo fragmente koronavirusa SARS CoV-2 in je bilo videti, kot da so okuženi. PCR test bi se lahko uporabljal samo ko virus kroži, to je od decembra do aprila. Lahko bi se uporabljal test na protitelesa, a 80-85% ljudi sploh ne proizvaja protiteles, samo 7-15% ljudi bi bilo pozitivnih na testu za antitelesa, ker bi dejansko tvorili protitelesa.
Svetovna zdravstvena organizacija (WHO) je objavila, da je samo 7-15% ljudi pri prejšnjem koronavirusu SARS CoV leta 2002 tvorilo protitelesa. Potem je WHO to informacijo izbrisala s svoje spletne strani. Zakaj do 85% ljudi ne producira protiteles, vključno z maldimi in zdravimi osebami? Ker virus ne vstopi v njihov sistem, ko se okužijo, se aktivirajo imunske T celice in virusi se ne replicirajo, ali nimajo receptorjev. zato sem proti zaklepanju (lock down), ker 85% ljudi sploh ne bo zbolelo, če se okuži s koronavirusom SARS CoV-2, za tistih 15% ljudi pa obstajajo zdravila oz terapije. Poleg tega ti virusi niso smrtonosni. Stopnja smrtnosti SARS 1 leta 2002-2003 je bila 1 na 8.000.000, pri SARS CoV-2 pa je 1 na 1.800.000. Od infekcijske tuberkuloze pa umre 3000 ljudi vsak dan. Zato lock down nikoli ni bil potreben in ni potreben. Če ne bilo politikov in medijev, ne bi bilo pandemije, saj je realna stopnja smrtnosti 1 na 1,8 milijona ljudi. Na Irskem imamo okoli 85 smrti vsak dan, in smrt zaradi koronavirusa SARS CoV-2 v tem številu sploh ni opazna. Sčasoma bo postalo jasno, da COVID-19 ni med vodilnimi vzroki smrti. Umirali so večinoma starejši bolni ljudje, ki so jih dali v domove in ne v bolnišnice. Umrli so bolj zaradi ukrepov, kot zaradi koronavirusa, na primer zaradi strahu, izolacije, postopkov zdravljenja itd....te smrti lahko pripišemo ukrepom vlad in kriznih štabov, ki so sledili navodilom WHO
Če bi testirali na primer na virus gripe A ali B, bi bil test poziteven pri ljudeh, ki so na primer preboleli girpo pred 6 meseci. tako PCR test ne pokaže, kdo je v tem trenutku okužen in je prenašalec virusov. Če je PCR test pozitiev pri osebi meseca junija, lahko to pomeni, da je bila oseba izpostavljena virusom decembra. Število okuženih s PCR testom je popolno zapravljanje denarja, saj bi na Irskem lahko našli na milijone pozitivnih primerov, ki pa so v resnici pozitivni na navzočnot fragmentov RNA virusov gripe influenza A, ki so bili v obtoku v populaciji decembra 2019. Potem bi lahko vsako leto vsak dan poročali, koliko ljudi je bilo okuženih z virusi gripe, ki smo jih večinoma vsi dobro prenesli. In mediji porabljajo ogromne količne časa, da poročajo o teh okužbah. Veliko vrst koronavirusov je v zraku ves čas. (op. prev.: dr. Zack Bush: V zraku okoli nas je 10 na 31 potenco virusov, več kot je zvezd v vesolju)
* * *
dr. Miha Avberšek, mikrobiolog, raziskovalec v zasebnem mikrobiološkem laboratoriju pravi:
Kako zanesljivi so testi? PCR test je sam po sebi zelo zanesljiv, vprašanje pa je, kaj z njim pravzaprav dokazujemo. Test PCR ne zaznava virusa kot celote, ampak zaznava virusno RNA. Le-ta je lahko v samem virusu, se pravi, da govorimo o virusu kot celoti in tak človek je tudi kužen. Lahko pa je RNA na človeški sluznici, vendar ne kot virus, ampak kot neki ostanek. In tukaj imamo težavo, saj bo test PRC pozitiven, človek pa ni kužen. Sam PCR test je torej precej zanesljiv, vendar ne dokazuje kužnosti. Upoštevati moramo še vzorčenje, torej način odvzema brisa, kar za sabo potegne določeno nezanesljivost. Kot pri vsakem testu, tudi tukaj prihaja do lažno pozitivnih in do lažno negativnih rezultatov.
Več na: https://www.zurnal24.si/slovenija/morda-bo-trajalo-se-kako-leto-dve-tri-ampak-v-koncni-fazi-bomo-morali-dojeti-da-je-z-virusom-treba-ziveti-353144?fbclid=IwAR0dSbVTNyB7vzBUWC7KeFuoYJuVdnT5pV7Me2slRF7CMvPzESopv_cXxL8 - www.zurnal24.si
* * *
Dr. Andrew Kaufman o neuporabnosti PCR testa. Če je oseba na PCR testu pozitivna, je 8% možnosti, da je resnično okužena s koronavirusom SARS CoV-2. V Veliki Britaniji načrtujejo s tem lažnim testom testirati vse prebivalce, rekli bodo da je 250.000 novih primerov okužb na dan, v resnici jih bo 20.000 od 10 milijonov Britancev, to je 0,2%.
Mediji bodo širili lažne novice, in strašili javnost, da je okuženih 250.000 ljudi. Vsak teden bodo dobili 1.500.000 lažno pozitivnih PCR testov. Leta 2021 bo v Veliki Britaniji vsaka 43 oseba napačno označena, kot da je okužena s SARS CoV-2. V resnici bodo te osebe popolnoma zdrave. Zato bodo zahtevali digitalni potni list, da bodo lahko obiskali zdravnika, šli v službo, potovali z letalom, obiskali množične dogodke in starejše sorodnike. Kdor bo imel lažno pozitiven rezultat, bo moral biti v karanteni. In vsak teden bo lažno pozitivnih 1.500.000 ljudi, ki bodo morali biti v karanteni in ne bodo smeli v službo.
To je operacija Moon Shot, ki je fašizem. Načrtujejo nenehno testiranje prebivalstva z neuporabnim PCR testom, ki zaznava tudi druge viruse iz družine koronavirusov, ki povzročajo navaden prehlad. Ta test daje velike napake in možnost, da 1.500.000 ljudi vsak teden označi za kužne, čeprav niso okuženi, pač pa so zdravi. To je hudo kršenje človekovih pravic in omejevanje svobode.
Vlade zelo dobro vedo, da je PCR test neuporaben in da nima dovoljenja za uporabo od nobene regulatorne agencije. Ni študij o učinkovitosti PCR testa in leta dolgo bi trajalo, da bi ta test dobil dovoljenje za uporabo od regulatornih agencij. Tudi Dr. Fauci Anthony je rekel, da zdravi ljudje ne prenašajo okužbe in ne širijo pandemije.
https://www.youtube.com/watch?v=vvPQEjnvqfA
*
Kanada: Koronavirus SARS CoV-2 ni izoliran in ni najden pri obdukciji: https://www.fluoridefreepeel.ca/u-k-dept-of-health-and-social-care-has-no-record-of-covid-19-virus-isolation/?fbclid=IwAR0-dSIh5N-BsaeDGDoqr32opy-cxpPsGjaEB2P-_l0T4o9aDMqRuZWVEpc
* * *
90 posto danas službeno inficiranih osoba po novim kriterijima zapravo uopće ne bi bile pozitivne. “I ovdje se ne radi ni o kakvoj manipulaciji ili prikrivanju podataka.
* * *
Ves čas pandemije se v Sloveniji sprejemajo nesorazmerni in kontraproduktivni Covid ukrepi predvsem na osnovi laboratorijskih rezultatov množičnega testiranja prebivalcev s PCR testi, ki ga forsira WHO. Laboratorijski pozitivni izvid PCR testa ne dokazuje virusa SARS CoV-2, ampak zazna le nek manjši del virusne RNA v odvzetem brisu iz nosu preiskovanca. Delčki virusne RNA ostanejo v telesu tudi še več mesecev po tem, ko je imunski sistem virus že uničil. Pozitivni izvid PCR testa ne dokazuje, da je ta oseba bolna in/ali kužna!
Izumitelj PCR metode, nobelovec dr. Kerry Mullis, je izrecno poudaril, da pozitiven PCR test ne dokazuje nalezljive bolezni.
Diagnoza bolezni le na osnovi PCR testa, posebno pri asimptomatskih osebah, JE STROKOVNA NAPAKA!!!
Raziskave eminentnih raziskovalcev (prof. dr. Sunetre Gupta z Oxforda, prof. dr. Jean-Francois Toussainta iz Pariza, nobelovca prof. dr. Michaela Levitta, idr.) dokazujejo, da je zaradi doseženega praga kolektivne imunosti PANDEMIJA CoV19 V EVROPI KONČANA.
To potrjujejo tudi uradni podatki o cca. 100-krat manjšem številu hospitaliziranih in umrlih glede na uradne podatke ob začetku pandemije CoV19 v vseh državah Evrope.
Nadaljnje množično testiranje ljudi s PCR je po mnenju prof. dr. Michaela Levitta kontraproduktivno zapravljanje denarja.
* * *
https://www.technocracy.news/google-pentagon-team-up-for-ai-to-diagnose-covid-19/
* * *
* * *
PCR positives: what do they mean?
September 17, 2020
Updated 23 September 2020
Article by:
info@future-synthesis.com
fsdataanalysis@gmail.com
matteo.chiesa@uit.no
sergio.s.hernandez@uit.no
Department of Physics and Technology, UiT The Artic University of Norway
9037 Tromsø, Norway, Future Synthesis AS Uniongata 18, 3732 Skien, Norway
PCR positives: what do they mean?
Download: PCR test REFERENCE_Infectivity 2020 Sept 18
Contents
- Is the PCR test sensitive enough?. page 2
- Culturing a virus as reference test page 2
- Does a PCR “TRUE POSITIVE” mean INFECTIVITY OR VIRULENCE?. page 2
- PCR true positives versus infectivity and virulence. page 3
- Explanation of the experiment that shows whether a virus is still infective. page 4
- Is there evidence that someone is infectious after PCR results?. page 4
- Can successive tests on the same person give contradictory results?. page 5
- How long can an inactive virus remain in a body? page 5
- PCR kits for SARS Cov2 (manufacturers and asymptomatic) page 6
- Conclusion in relation to PCR positives and an advancing pandemic. page 6
- Are PCR tests helpful?. page 7
- Statistical analysis: PCR positives and deaths (excess deaths) page 7
- CONCLUSIONS. page 9
Is the PCR test sensitive enough?
The PCR is very sensitive and will detect the presence of viral RNA (with PCR the virus is detected by targeting one or more gene fragments). The gene fragment might be detected and the virus “positively found”. But is this viral RNA active? That is, does the detected viral RNA have the capacity to reproduce or infect the person (virulence) or get transmitted to other people (infectivity)?
The Centre for Evidence-Based Medicine (CEBM) says[1, 2]:
“PCR detection of viruses is helpful so long as its accuracy can be understood: it offers the capacity to detect RNA in minute quantities, but whether that RNA represents infectious virus may not be clear.”
Culturing a virus as reference test
What are a reference test and a baseline? Many experiments in science are relative in the sense that they do not give absolute values or need to account for context dependent data. In this sense, it is typical of scientific instrumentation and measurements to require calibration or a baseline. The baseline and calibration allow the scientist to interpret the results. In this respect, the CEBM writes:
“Viral culture [acts] as reference test against which any diagnostic index test for viruses must be measured and calibrated, to understand the predictive properties of that test.”
Does a PCR “TRUE POSITIVE” mean INFECTIVITY OR VIRULENCE?
What does viral culture tell about PCR positives?
A PCR test might find the virus it was looking for. This results in a PCR positive, but a crucial question remains: is this virus active, i.e. infectious, or virulent? The PCR alone cannot answer this question. The CEBM explains why culturing the virus is needed to answer this question:
“In viral culture, viruses are injected in the laboratory cell lines to see if they cause cell damage and death, thus releasing a whole set of new viruses that can go on to infect other cells.”
That is, if the PCR detects the virus in the human sample, this detection might correspond to a virus that is now incapable of infecting cells and reproduce. Biologists can tell if the virus is infectious by injecting it into cells (culture cells). If these cells are not affected by the virus and the virus does not reproduce in them, then the PCR test found a virus that is no longer active.
The meaning is that the PCR positive is a non-infectious positive.
PCR true positives versus infectivity and virulence
Does a PCR positive mean TRUE POSITIVE if the gene fragments targeted in the PCR are unique to the virus and the PCR is VERY ROBUST?
There is speculation as to whether the PCR can indeed find the virus from a person’s sample or maybe the PCR is not sensitive enough and might give positive when other viruses are present. Some PCR manufacturers tell us there is “cross contamination” and “non-specific” interference with a list of viruses and other in their instructions manuals[3, 4].
POSSIBILITY ONE: the PCR test is positive, but this was due to cross-contamination or non-specific interactions. Then the test would be a FALSE POSITIVE because the SARS Cov2 virus is not present in the sample. This means the PCR positive is a FALSE POSITIVE rather than a TRUE POSITIVE. But this is not the only possibility. We want to focus on the CEBM argument that depends on viral culture.
POSSIBILITY TWO: Even if the PCR test only detects TRUE POSITIVES in the sense that the SARS Cov2 virus, or better, the target gene fragment, is present in the sample, it remains to be seen whether the person can infect others or even if the virus is still infecting the very person carrying the virus.
What did Tom Jefferson et al. find in their investigation regarding viral culture of SARS Cov2 in order to assess infectivity (horizontal transmission or capacity for a virus to spreads among hosts) and virulence (a pathogen’s ability to infect or damage a host):
“We, therefore, reviewed the evidence from studies reporting data on viral culture or isolation as well as reverse transcriptase-polymerase chain reaction (RT-PCR), to understand more about how the PCR results reflect infectivity.”
What does this mean? The authors wanted to find out if 1) PCR TRUE POSITIVE meant that the virus found in the person could be transmitted to other people or was virulent or 2) the virus was no longer infective or virulent.
Explanation of the experiment that shows whether a virus is still infective
Imagine that a virus enters your body. In a few months it might not do anything to you anymore. It might not do anything to your cells (virulence), and it might also lack the capacity to move into another person (infectivity) when you speak or sneeze. It is also possible that this virus simply never did anything to you and lacked infectivity from the very beginning. But traces of the virus might still be present in the person. In this case, the virus is present but inactive.
So how do you know if the virus is active? You do the PCR. If the virus is found in the person (PCR TRUE POSITIVE), that virus is injected into a culture cell. If by injecting that virus into culture cells, the virus is not able to reproduce in the cells, that virus cannot infect anybody any longer. This means that even if you are a PCR positive, you are no longer contagious, that is, the virus in you is no longer active.
Conclusion: A TRUE POSITIVE in PCR does not always mean that the person presents any danger to society. The virus cannot be transmitted when cell culture shows that the virus is not infective. Unfortunately relating PCR POSITIVE to infectivity is not easy if we consider the whole population. This would need 1) a model (correlation) that maps PCR POSITIVES and/or symptoms to infectivity as tested by viral culture or 2) viral culture for every individual case. See next.
Is there evidence that someone is infectious after PCR results?
Tom Jefferson et al. claim that after searching for the PCR to viral culture correlation no conclusion was found since time from collection and symptoms severity are needed for the correlation amongst other to find an appropriate model. We recall that currently they (governments) hardly look for symptoms in people. Positives are called PCR Positive asymptomatic if they present no symptoms. In the article the authors say:
“Data are sparse on how the PCR results relate to viral culture results. There is some evidence of a relationship between the time from collection of a specimen to test, symptom severity and the chances that someone is infectious.
One of the studies we found (Bullard et al) investigated viral culture in samples from a group of patients and compared the results with PCR testing data and time of their symptom onset.” Figure 1.
Conclusion:
“It was not possible to make a precise quantitative assessment of the association between RT-PCR results and the success rate of viral culture within these studies.
This means that PCR Positives might or might not lead to concluding that a subject testing positive by PCR is infectious. Why? Because PCR positives have not been correlated to the growth of the virus in culture. They continue to explain why this correlation is not possible:
“These studies were not adequately sized nor performed in a sufficiently standardised manner and may be subject to reporting bias.”
Can successive tests on the same person give contradictory results?
That a PCR test gives positive or negative depends on how the experiment is conducted. Furthermore, since it is not know whether and how PCR positives correlates to infectivity and how it is that this correlation must be interpreted, the interpretation of a PCR POSITIVE is inconclusive. The authors claim:
“Cycle thresholds are the times that the amplifying test has to be repeated to get a positive result. The higher the viral concentration the lower amplification cycles are necessary.”
Some people might give positive after running the PCR test with a high threshold and others with a low threshold. The threshold alone might or might not tell whether someone carries infective viral RNA.
How long can an inactive virus remain in a body?
This is inconclusive since PCR positives to viral culture studies are lacking and cycle thresholds should also be considered. See above. The way in which the experiment is carried out however, matters. This is because one might be PCR Positive long after the virus is no longer active. The authors briefly explain why:
“This detection problem is ubiquitous for RNA virus’s detection. SARS-CoV, MERS, Influenza Ebola and Zika viral RNA can be detected long after the disappearance of the infectious virus. … because inactivated RNA degrades slowly over time it may still be detected many weeks after infectiousness has dissipated.”
The authors show a figure (figure 2) where it is noted that the presence and detection of viral RNA by PCR does not imply that the virus is infectious or virulent any longer.
PCR kits for SARS Cov2 (manufacturers and asymptomatic)
PCR positives on asymptomatic people should be treated with care since it is possible that the asymptomatic people are not infectious. This is even when the PCR tests or the antibody tests are positive. This is because viral culture is required to establish if the viral RNA is capable of infecting cells and “reproduce”.
PCR manufacturers typically remind the users that “the detection result of this product is only for clinical reference, and it should not be used as the only evidence for clinical diagnosis and treatment[3]” and “designed for the specific identification and differentiation of the new coronavirus (SARS-CoV-2) in clinical samples from patients with signs and symptoms of Covid19”.
Conclusion in relation to PCR positives and an advancing pandemic
Conclusion: symptoms and signs of Covid19 are necessary to support the claim that the subject is or can be infectious. But calling PCR positives “cases” does not specify whether the persons have carried the virus for long or whether it is “active”. This could lead to the finding of many “cases” as a function of the number of PCR tests conducted. For example, if 20% of a population are PCR positive, the number of PCR positives will depend on the size of the sample. This means that the more PCR test are carried out the larger the fraction of the population that is confirmed but this might not speak of changes in the population. That is, it is possible that the population was infected already long before deciding to test and PCR positives would therefore not speak of “an advancing pandemic”
Are PCR tests helpful?
It is typical now to call PCR positives that present no symptoms asymptomatic (see above). It is highly likely that these tests are detecting viral RNA in patients where the virus is no longer capable of infecting. A statistical test where biological equipment would not be required could involve correlating deaths to PCR positives (we discuss this next )The CEBM authors claim:
“PCR detection of viruses is helpful so long as its limitations are understood; while it detects RNA in minute quantities, caution needs to be applied to the results as it often does not detect infectious virus.”
Statistical analysis: PCR positives and deaths (excess deaths
We start by claiming that if PCR positives have any predictive power on the number of deaths expected, there should be some correlation, i.e. the more PCR positives (SARS Cov2) today the more deaths by Covid19 in the future (at least a few days later but presumably 2-4 weeks later at least if the PCR is taken just after infection). Figure 3 illustrates this.
However, in figure 4 we show PCR positives versus Covid19 deaths as labelled by the Spanish ministry of health. https://www.mscbs.gob.es/profesionales/saludPublica/ccayes/alertasActual/nCov/documentos/Actualizacion_207_COVID-19.pdf
Covid19 labelled death versus TRUE death by Covid19
We differentiate between labelled Covid19 and death by Covid19 as the true cause of death. Since we cannot know the true cause of death (this is done by medical examiners but the results are or can be relatively subjective) we will also discuss excess deaths later. A ratio between infections and deaths is the typical way in which mortality is considered[5]. A simple function between PCR positives to Covid19 could be a linear function (Eq. 1). We can add a time delay indicating that it takes time for people to die after being infected (Figures 3 and 4). This function should have some predictive power to be useful. If so, there should be correlation. Here D(t) is the number of deaths at time t (or a given day) and P(t*) is the number of PCR positives at an earlier time t*=t-t0, where t0 is the time between the number of deaths D recorded and the number of PCR Positives recorded (typically days to weeks as shown in Figure 5). Here α is the effective mortality rate, i.e. for a number of PCR Positives P, D deaths should be expected after a t0 (α =D/P).
![]()
Figure 5 shows schematically that t0 is expected to be between 20 and 30 days roughly (4 weeks) and on average. Ideally and accordingly, if the PCR tests were performed during the very first days of infection, Eq. 1 would give us some predictive power over the number of deaths by Covid19 expected in t0 days (time).
For the Spanish data (Figures 4, 6 and 7) the key points are:
- Figure 4 shows that the same order of magnitude of positives was recorded in March-April 2020 as in July-August-September 2020 but the number of deaths was much lower in August to September (data from the Spanish Ministry of Health). This means that 1) either we do not have the true infection fatality ratio (IFR) but a (CFR), 3) the cases in March-April correspond to different phenomena to those in July-September, or 3) the virus has mutated so rapidly that the true IFR has changed already and dramatically. We believe that the second point here is key and the explanation is that the cases in March-April were cases of truly infected people whereas in July-September the cases correspond to people that have mostly passed the infection already, i.e. will not die. The confirmation of this hypothesis would be given by viral culture experiments as discussed by Jefferson et al. above.
- Figure 6 shows that the peak in PCR positives in March-April does not lead to a peak in deaths at the end of April. We ran a correlation test and got numbers in the 0.4-0.2 range. If a delay of 10-20 days is allowed, implying that we want to predict deaths in the future from PCR positives today, the correlation coefficient gave us numbers below 0.2 (not shown). The same happens with the more decent data in July August (not shown).
What if we take into account excess deaths instead?
The data for total deaths in 2020 in Spain, mean number of deaths for the years 2010 to 2019 and confidence interval for those years is provided by the Spanish Ministerio de Ciencia e Innovación at https://www.isciii.es/QueHacemos/Servicios/VigilanciaSaludPublicaRENAVE/EnfermedadesTransmisibles/MoMo/Paginas/Informes-MoMo-2020.aspx)
We might argue that labelled deaths are not in agreement with the true number of deaths by Covid19. If we take excess deaths instead, this being the number of deaths in 2020 compared to previous years (2010-2019) we can plot the normalised excess deaths (blue) against normalised PCR positives (black) in Figure 7. There is no time delay between PCR tests and excess deaths as shown in Figure 7 and it could be argued that this could explain the lack of correlation. We applied a time delay and checked the coefficient of determination for delays ranging from 0 to 45 days (Figure 8).
The highest value for the coefficient of determination R2 was found by applying no delay as seen in Figure 8. The implication is that the number of positive PCR cases is proportional to the excess deaths reported that day, i.e. with no time delay. If that was the case the PCR testing would be ultimately redundant since knowing the excess deaths tells you at once excess deaths that day which is the variable targeted in the study. We still find no meaningful correlation (correlation coefficients still much below 0.5, Figure 8) by applying delays as shown in Figure 8. Data from May to the end of August is shown in a scatter diagram, i.e. PCR positives versus excess deaths, in Figure 9.
CONCLUSIONS
As shown in Figure 8, the more delay we give to the PCR positives recorded on a given day in relation to the excess deaths recorded, the lower R2. A delay of at least a few days to weeks would be meaningful, i.e. would imply PCR positives predict the number of deaths in the future since governments could “expect” what is to come in the future on the basis of the number of PCR positive cases recorded on a given day. The R2 number however, and Figures 4, 7, 8 and 9 , show that PCR positives do not correlate to excess deaths in the future. The implication is that PCR positives lack predictive power in terms of telling whether people will die in the future.
A possible explanation could be that the PCR positives simply measure the number of PCR tests taken on a given day, i.e. they might be somewhat proportional to the number of PCR taken on a given day, and positives might or might not be “infectious” positives. Ultimately, this means PCR positives cannot be used to tell if the pandemic is advancing if for that we understand that deaths are to increase or decrease. This agrees with the interpretation of CEBM above.
Finally, we want to point out that the same can be said for all countries we have examined, i.e. other than Spain. For example, in the months of July to September positive cases in Europe are said to have risen, but we find no evidence of excess deaths in the countries in Europe reported by euromomo.eu (Figure 10). We believe the rise in deaths toward August and September corresponds to the heat wave. It seems like this year the heat wave has been displaced toward August and September, rather than July and August as in previous years, in some European countries. In this work we have dedicated most attention to the Spanish data but more curves providing Positive PCR cases versus deaths (not excess but Covid19 as reported by each country) can be found at worldometers.info (https://www.worldometers.info/coronavirus/), John Hopkins, and other sources. Such data can be submitted to either visual inspection or PCR positive to excess death correlation as shown here. Our impression is that most data for all countries is in agreement with our interpretation, namely, PCR positives do not correlate to deaths in the future and are therefore meaningless, on their own, to interpret the spread of the virus in terms of potential deaths.
We suggest that the hypothesis of CEBM, i.e. that viral culture is required as a reference to test for infectivity, and other similar ones such as that by Jared Bullard et al[6]., i.e. search for relations between cycle threshold (Ct), symptom onset and infectivity in cell culture, should be explored in order to increase the predictive power of tests. Such predictive power is central provided the possible advance of the pandemic is to be understood and provided we understand that an advancing pandemic must be related to excess deaths in the future. Finally, regarding deaths, we must consider carefully Covid19 labelled deaths versus excess deaths. Covid19 labelled deaths depend on subjective parameters whether excess deaths have the advantage of being a standard relative to a reference, namely, the number of deaths in previous years. If we find many Covid19 deaths during a period but excess deaths are low or negative, it is likely that we are inflating Covid19 numbers. Furthermore, excess deaths typically depend on high/low temperatures, i.e. cold winters or heat waves (Figure10). Therefore, any light increase/decrease in deaths should be contrasted to the temperature. For example, heat waves might come in June, July, August or even September (2020 -Spain[7]) in Europe and direct comparison between years should consider this.
Vir: https://www.cebm.net/covid-19/pcr-positives-what-do-they-mean/
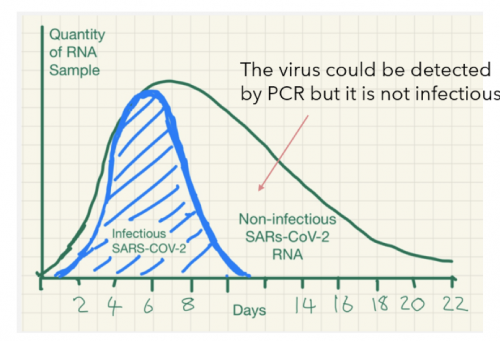
več tabel in diagramov je v članku na naslovu: https://www.cebm.net/covid-19/pcr-positives-what-do-they-mean/
The Bomb in the Basement at the CDC
Firstly, I would like to express my gratitude to Jon Rappoport (www.nomorefakenews.com) for making me aware of the work of Dr. Tom Cowan M.D.
Dr. Cowan is one of those individuals who is much more interested in helping his fellow man or woman than in making a profitable business out of the practice of medicine. This has led him to not only search out alternative solutions where standard therapies have failed but to also question the quality of the “science” espoused and published by the main stream press. In our present circumstances this has turned out to be of overwhelming importance especially in view of his discoveries at the Centers for Disease Control.
Dr. Cowan has looked into the article published in the CDC journal in June 2020 in which a group of about 20 virologists describe the present state of progress in identifying, isolating and purification of “Sars-Cov-2” with a view to establish the genome sequence of the Covid-19 causing “virus” of which the Sars-Cov-2 protein fragment is presumed (without evidence, note!) to be a part.
The CDC report states that “researchers” examined the genetic sequencing of Sars-Cov-2 by using the Polymerase Chain Reaction (PCR) probes to extract them from impure samples. They were able to find just 37 base pairs. This they then fed into a computer which they had programmed to add another 29,973 base pairs to make up the presumed Covid-19 “virus”.
For those not familiar with microbiology, it is undoubtedly useful to put this into a more prosaic analogy to make the enormity of this crime apparent.
Let us say that you are in a football stadium with a crowd of 30,000 people. You select a group of 37 people who happen to be standing together and, from their appearance, you attempt to gain the names and addresses of the other 29,963 people in the stadium. Do you believe that this is possible? Yet this is exactly what is claimed has been done in the basement rooms of the CDC.
37 gene base pairs have actually been found. What their relationship, if any, is to Covid-19 is unknown. A computer, perhaps randomly, has added 29,973 other gene pairs from a database which is then claimed to be the identity of the Covid-19 causing “virus”. Do you find this believable? Honest virologists and other scientists do not! In fact, they call it fraud pure and simple.
A few months earlier, "Prof" Drosten from the Charité teaching hospital in Berlin had done exactly the same thing to spur on the Covid panic-mongering in Germany. The above mentioned "study" of the CDC also refers to a publication with the same content from March 2020. Whether this was done by Mr Drosten cannot be determined from the report. For his "performance", "Prof." Drosten in any case reaped both criminal charges and a damages claim for one billion dollars.
It gets, however, much, much worse.
The experimenters then took samples of Sars-Cov-2 and attempted to grow them in various tissue samples both from humans and from monkeys. The only tissue in which there was any significant replication was in kidney tissues extracted from monkeys. The reaction of the human tissues varied from minimal to complete rejection thus indicating that, whilst Sars-Cov-2 may have some resonance with monkeys, it has none with humans
Pozivamo strokovno javnost, da laični javnosti predstavi resnico o tako imenovanem PCR testu (Polymerase Chain Reaction) na katerem sloni dokazovanje okužbe z COVID-19 oz. vsi vladini ukrepi, vključno z razglasitvijo epidemije. Glede testa je njegov izumitelj, Kary B. Mullis izjavil, da ni namenjen, ne razvit in niti registriran za diagnostične namene. Če se vlada in mediji sklicujejo na strokovnjake pri diagnosticiranju okužb ali ni sam izumitelj testa največja strokovna avtoriteta glede tega?
https://www.youtube.com/watch?v=iWOJKuSKw5c&feature=emb_title
Test namreč ni specifičen na omenjeni korona virus, ampak lahko delček RNK, ki ga s testom iščejo, izvira od drugih korona virusov, ki povzročajo prehlade in so v človeku ves čas prisotni na respiratornih sluznicah. Sezona virusov je med decembrom in aprilom, a so virusi prisotni tudi izven tega obdobja, vendar ne povzročajo bolezni, ker nimajo pogojev za razmnoževanje.
Pozitiven test v resnici ne prinaša nobenega relevantnega podatka saj ne pove ali je človek okužen z novim korona virusom in ne pove ali so ti virusi virulentni, niti koliko je teh virusov v telesu, niti ali bo oseba zbolela za boleznijo COVID-19. Prav tako ne pove ali lahko oseba, ki je bila pozitivna na PCR testu, okuži drugo osebo. Iz tega sledi, da je test za klinično diagnosticiranje neuporaben in zaradi tega je mag. Vladimir Pirnat, dr.med. izjavil, da je diagnoza COVID-19 na osnovi PCR testa strokovna napaka. Vse to pomeni, da NIJZ oz., centri za odvzem brisov delujejo nezakonito in brez naše vednosti zbirajo naš DNK.
Kljub temu NIJZ vsak dan objavlja število novih okužb s katerimi opravičujejo vladine ukrepe in sprejemanje zakonov, ki jih uveljavljajo inšpekcije in policija. Na podlagi neuporabnega testa se nam odvzemajo svoboščine, ustavne pravice in uničuje gospodarstvo!!!
Prav tako lahko gre tudi tukaj za sum kaznivega dejanja korupcije vlade in njenih inštitucij. Namreč, do 21.10. 2020 je bilo opravljeno 307.243 testiranj in cena enega testa je približno 100 eur, kar pomeni da je bilo za testiranja porabljenih 30.724.300 evrov (30.7 milijonov evrov). Glede na vse škandale pri nabavi zaščitne opreme je povsem primerno vprašanje ali tudi tukaj tiči del odgovora glede vladajočih, ki sedaj razmišljajo o množičnem oz., obveznem testiranju?
S tem bodo prestopili še zadnjo ustavno pravico oz. osebno svoboščino glede nedotakljivosti telesa, kar je nedopustno in predstavlja končno izdajo ljudstva. Miha Zimšek
*
Tehnični podatki o PCR testiranju: https://www.youtube.com/watch?v=ThG_02miq-4&t=53s&fbclid=IwAR2c-jnhzX5E4sqsxJgaCZeX2LI2PwNj3Son6YL0yoRMwh7u-n0X6p1d-9o
*
Nekaj clankov v zvezi z PCR testi pred letom 2020:
- •
For swab tests taken for screening purposes before elective procedures or surgeries: unnecessary treatment cancellation or postponement
- •
For swab tests taken for screening purposes during urgent hospital admissions: potential exposure to infection following a wrong pathway in hospital settings as an in-patient
- •
Financial losses related to self-isolation, income losses, and cancelled travel, among other factors
- •
Psychological damage due to misdiagnosis or fear of infecting others, isolation, or stigmatisation
- •
Misspent funding (often originating from taxpayers) and human resources for test and trace
- •
Unnecessary testing
- •
Funding replacements in the workplace
- •
Various business losses
- •
Overestimating COVID-19 incidence and the extent of asymptomatic infection
- •
Misleading diagnostic performance, potentially leading to mistaken purchasing or investment decisions if a new test shows high performance by identification of negative reference samples as positive (ie, is it a false positive or does the test show higher sensitivity than the other comparator tests used to establish the negativity of the test sample?)
- •
Misdirection of policies regarding lockdowns and school closures
- •
Increased depression and domestic violence (eg, due to lockdown, isolation, and loss of earnings after a positive test).
Kljub pomoči z vseh koncev je bilo v zadnjem času kadra na nekaterih vstopnih točkah, kjer jemljejo brise po Sloveniji, premalo, da bi lahko bris vsakomur, za katerega je osebni zdravnik presodil, da je to potrebno, vzeli v 24 urah. Nekateri so tako čakali tudi po teden dni. Tudi zato so se v začetku tedna, kot pove prof. dr. Bojana Beović, vodja strokovne skupine, začasno odločili, da bodo po novem s PCR-testi testirali manj ljudi, le tiste, pri katerih zaradi starosti ali pridruženih bolezni pričakujejo težji potek bolezni, in tiste, ki imajo stik z ranljivo populacijo ali imajo zaradi dela, ki ga opravljajo, veliko stikov. Ali vas bodo poslali na PCR-test ali ne, ostaja odločitev osebnega zdravnika.
Ker bo v prihodnje testiranja s PCR-testi manj, je vlada pred dnevi napovedala uvedbo hitrih antigenih testov.
Gre za teste, ki so hitrejši, rezultat dobijo v 15 minutah, tudi cenejši, a so manj zanesljivi kot prej omenjeni PCR-testi. Dr. Mateja Logar z Infekcijske klinike: "Pri PCR-testih dokazujemo delček virusnega genoma, pri antigenskih pa dokazujemo prisotnost antigena, ki je prisoten na virusni površini. Glavna razlika je v tem, da je PCR-test bolj specifičen, zazna res ta virus, ki ga določamo, in tudi ima boljšo občutljivost, se pravi zazna manjšo količino virusa." Hitre antigenske teste so v nekaterih slovenskih bolnišnicah, tudi na ljubljanskem kliničnem centru, že testirali, torej uporabljali vzporedno s PCR-testi. Potrjeno negativen hitri antigenski test je pri tistih bolnikih, za katere že zdravnik presodi, da je verjetnost z okužbo nizka, za bolnišnice zelo pomembna informacija. "Konkreten primer je recimo bolnik, ki pride po poškodbi na urgentni kirurški blog, ne more podajati ustrezno svoje anamneze, nimamo ustreznih podatkov o tem, da bi imel kakšen tvegan kontakt, v njegovi okolici ni bolnih, v tem primeru nam bo negativen test povedal to, da je verjetnost, da je bolnik okužen, zelo majhna in ga lahko umestimo v navadno sobo, ni ga treba izolirati. Enako pri internističnih bolnikih, ki prihajajo zaradi miokarnega infarkta, pa ima bolnik tudi vročino, nima pa drugih znakov, ki bi govorili v prid covida," razlaga dr. Logar.
Zdaj naj bi hitre antigenske teste začeli uporabljati tudi za testiranje tistih - čeprav so trenutno zdravi -, ki delajo z ranljivimi skupinami ali so zaradi svojega poklica v stiku z veliko ljudmi. "Na ta način bi našli vsaj nekatere pozitivne med ljudmi, ki so sicer brez znakov bolezni, hodijo v službo, vedno se pri tej bolezni bojimo tega zgodnjega izločanja virusa, preden človek zboli, če ga najdemo v tem obdobju, potem mislimo, da bi lahko, to kažejo tudi tuje raziskave, lahko zmanjšali breme bolezni. Predstavljajte si, da bi vse zaposlene v Kliničnem centru, ki delamo z bolniki, dvakrat na teden testirali, da se ujame tiste, ki bodo kmalu zboleli, že izločajo virus in so nevarni za druge," je rekla dr. Beović. Na vprašanje, kdo vse bo testiran s hitrimi antigenskimi testi, "samo tisti, ki ste jih ravnokar omenili ali tudi splošna populacija, ljudje, ki jih zdravniki zdaj ne bodo naročili na PCR-teste", je odgovorila: "O tem se še pogovarjamo, kakšen bo pristop, ampak prav gotovo je smiseln takšen usmerjen pristop, da testiramo tiste, pri katerih je ta informacija pomembna, torej ljudje, ki delajo z ranljivimi skupinami in imajo veliko stikov, recimo policija, in je pomembno, da se vedo, ali so sami okuženi ... Temu se lahko pridruži neko testiranje splošne populacije, ampak mislimo, da je testiranje ljudi, ki kar tako grejo na test, ne da bi ali da ne bi imeli kakršnekoli indikacije zaradi slabega počutja ali stika z bolnim, to prinese najmanj dobrobiti. Pomembno se je fokusirati na tiste probleme, kjer je veliko izbruhov ali pa gre za ljudi, ki lahko hudo zbolijo." Ključni problem hitrih antigenskih testov seveda je, da niso tako zanesljivi kot PCR-testi. O tej razliki tudi nocoj v 24UR Inšpektor. In o vseh opozorilih, kako naj se obnašamo, tudi če nismo napoteni na testiranje: vsi s simptomi, tudi če so videti zgolj kot blag prehlad, naj ostanejo doma, opozarja dr. Beović; naj ne hodijo v službo, trgovine ...
https://www.24ur.com/novice/korona/testi-na-koronavirus.html
* * *umX Metrics
Tweet 13.11. 2020
Elon Musk
Sep 05, 2020

