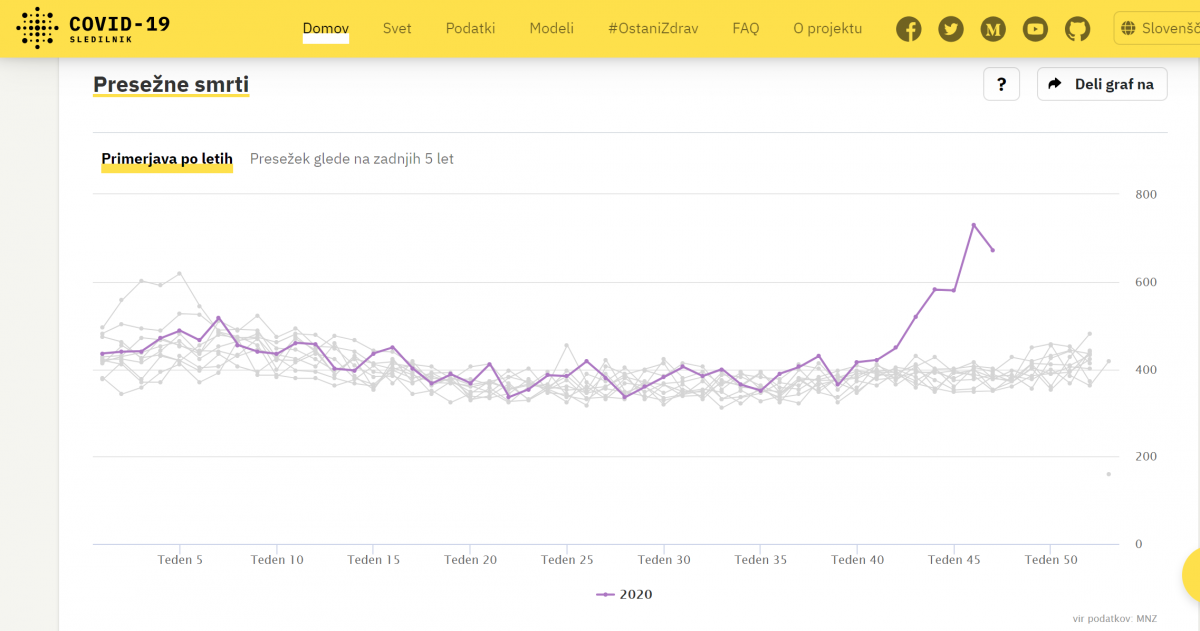

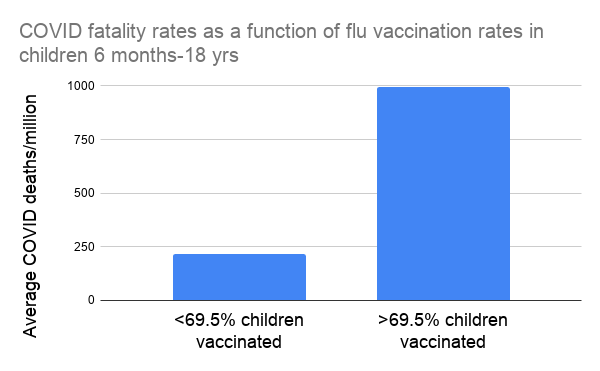
Umrli od korone so stari in bolni ljudje, ki so leta dolgo bili cepljeni proti gripi
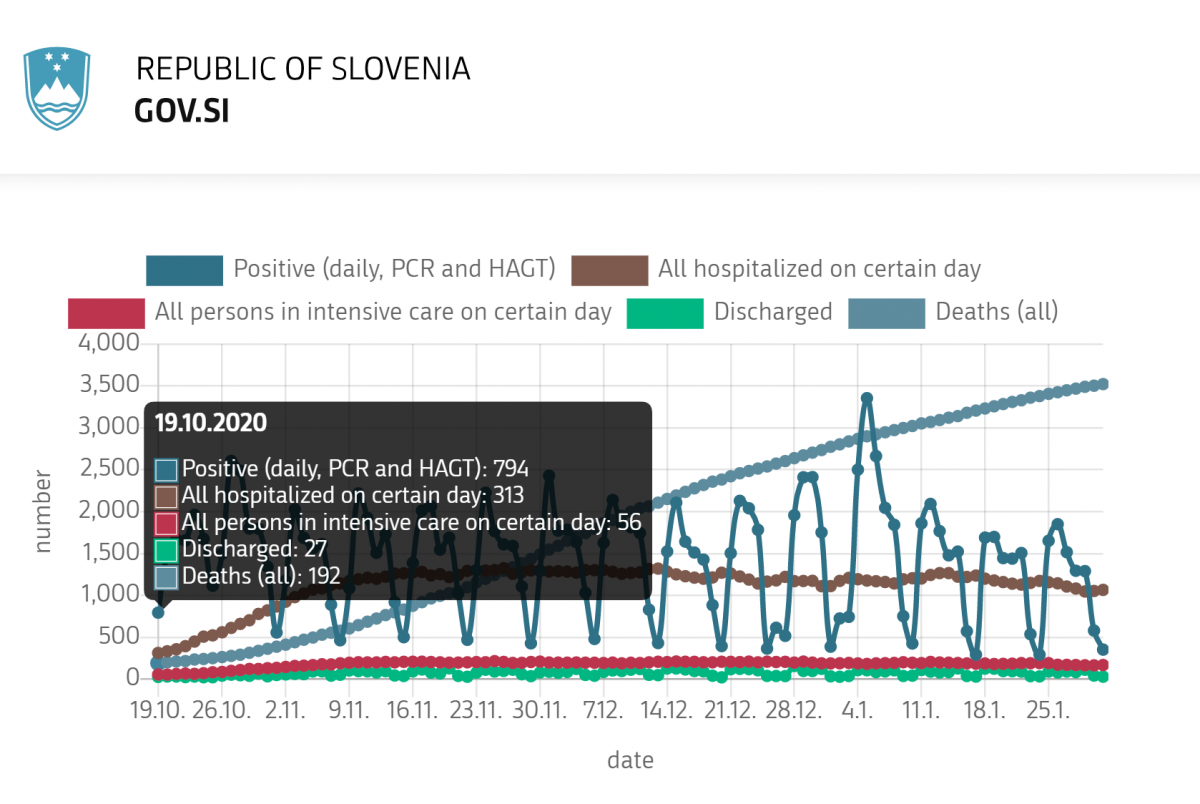
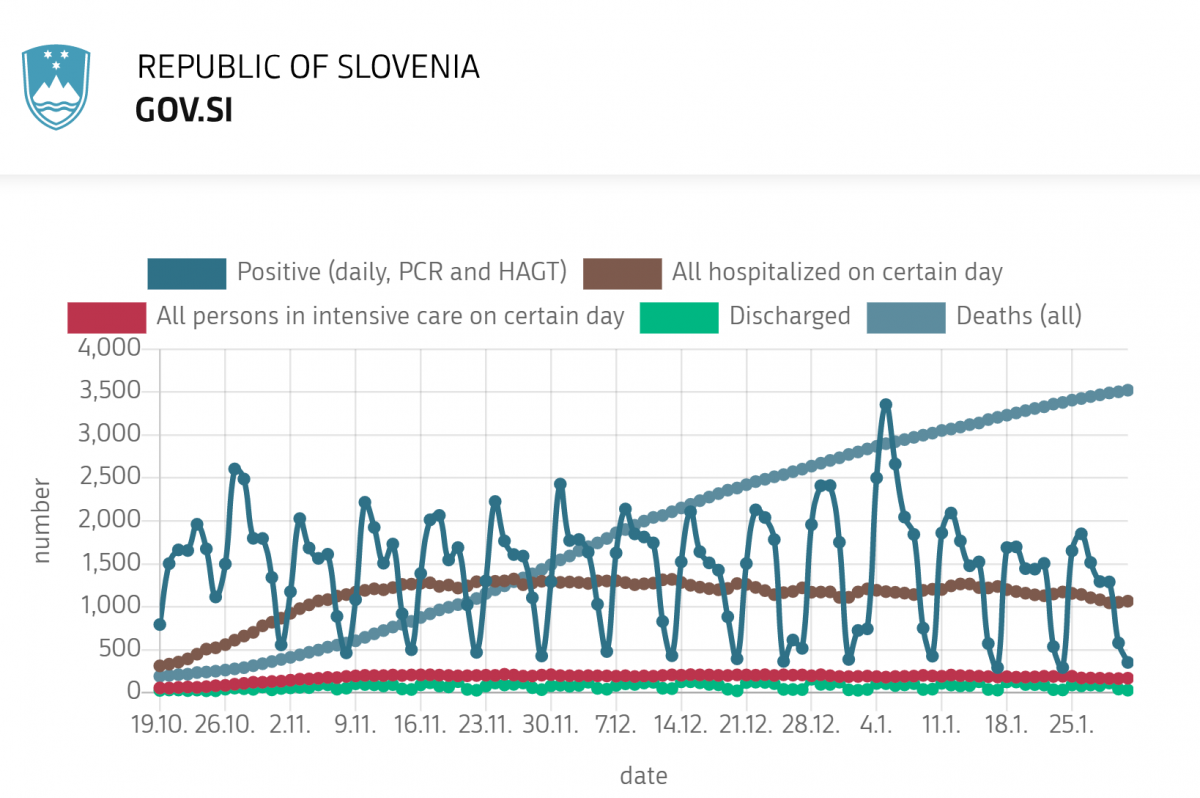
Vir: https://www.worldometers.info/coronavirus/country/slovenia/
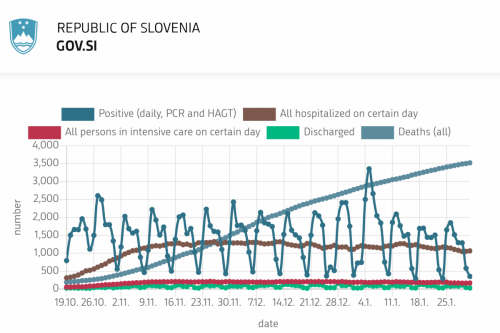
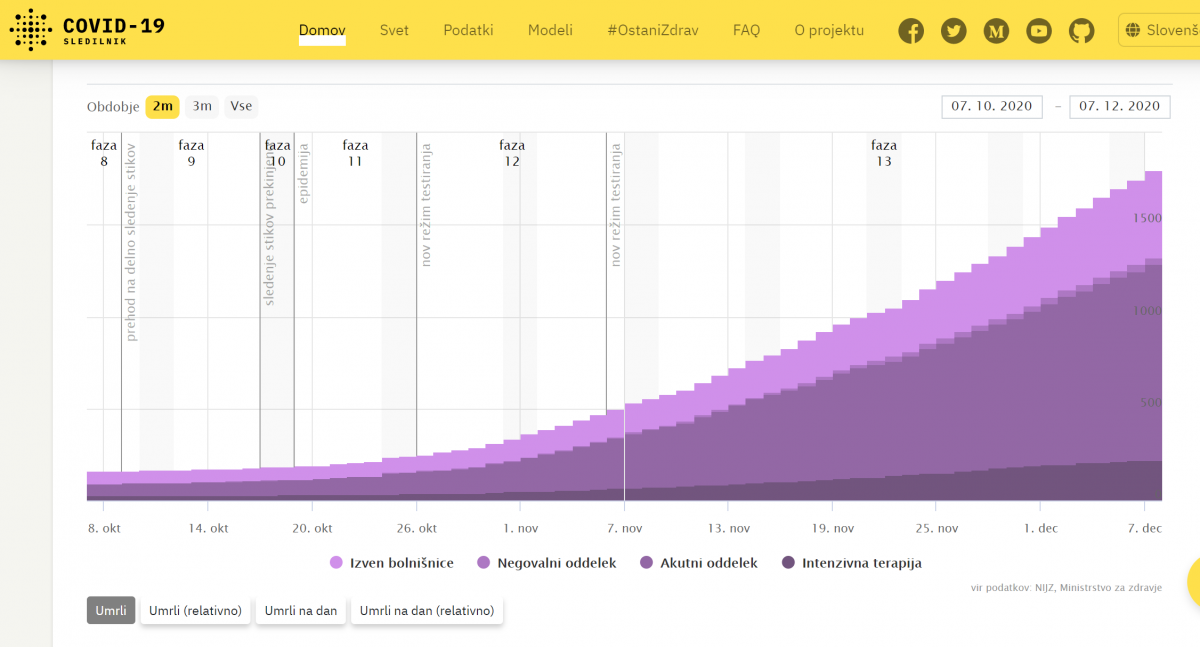
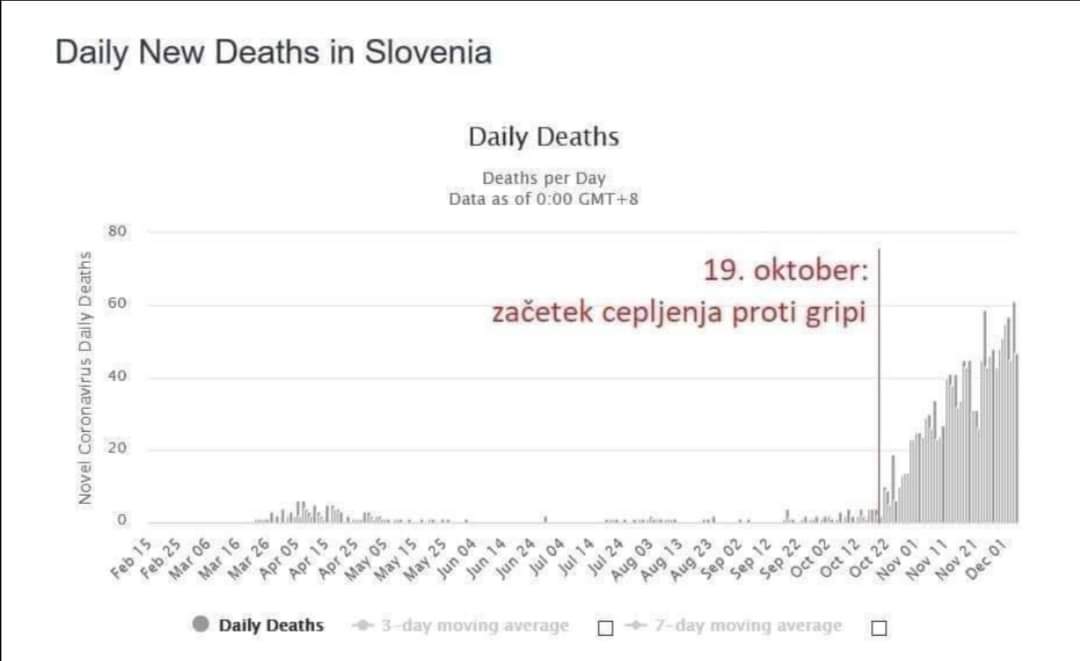
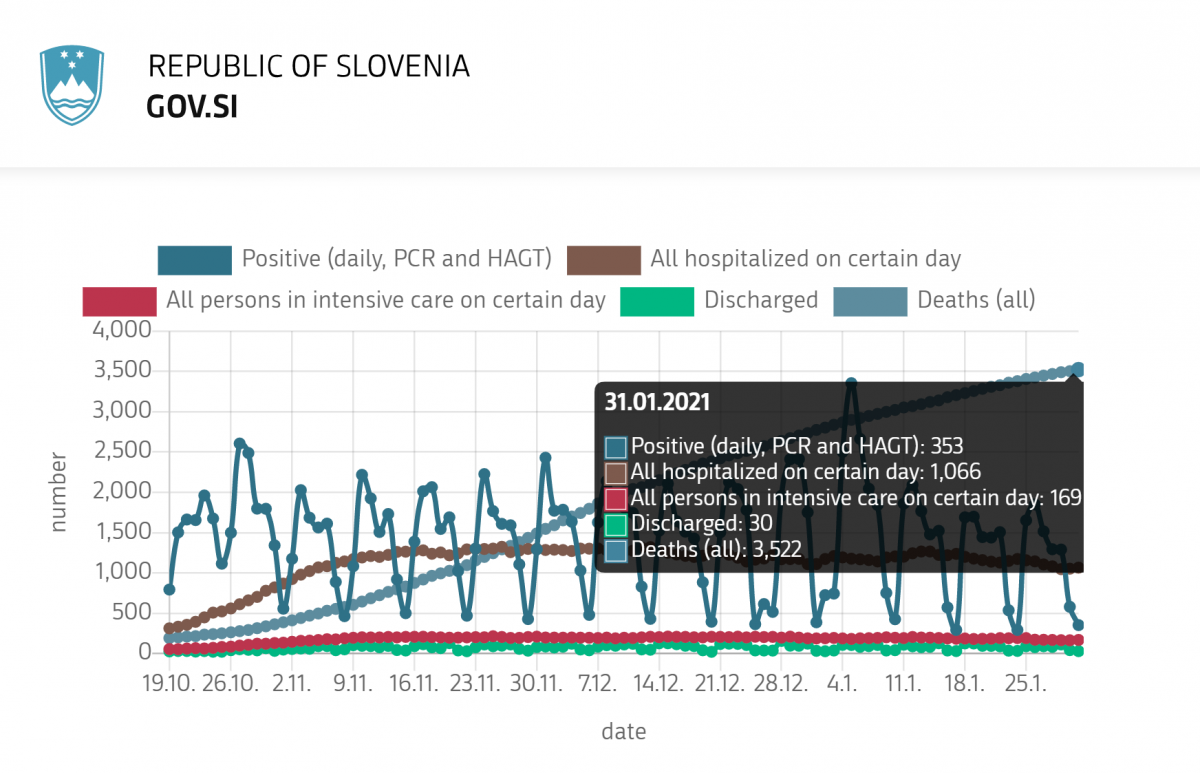
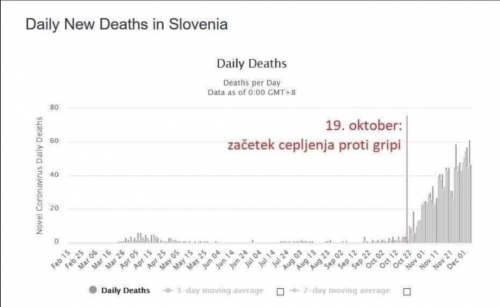
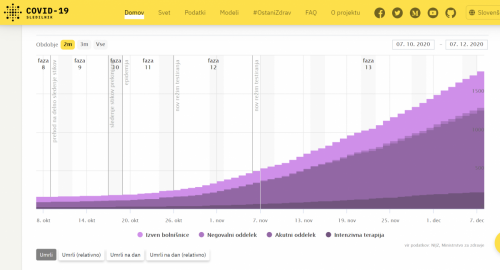
Začetek cepljenja 19.10. 2021 je v korelaciji z začetkom povečanja smrti zaradi COVID-19 (na sliki prikazano s točkovno krivuljo, ki strmo narašča). Dne 19.10. 2020 je bilo 192 umrlih in 31.1. 2021 je bilo 3522 umrlih
*
Imunolog Srečko Sladoljev o cepljenju za gripo, ki lahko povzroči avtoimuno bolezen s protitelesi na interferon, ki je osnova celične imunosti, kar lahko povzroči smrti zaradi COVID-19
(od 28.40 min dalje)
https://www.youtube.com/watch?v=sQ5dd5CmUq8
***
Daniel Colnar 30.9. 2020
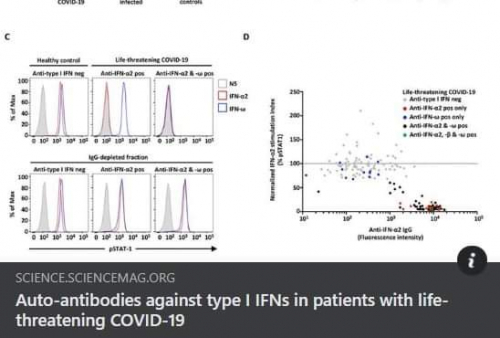
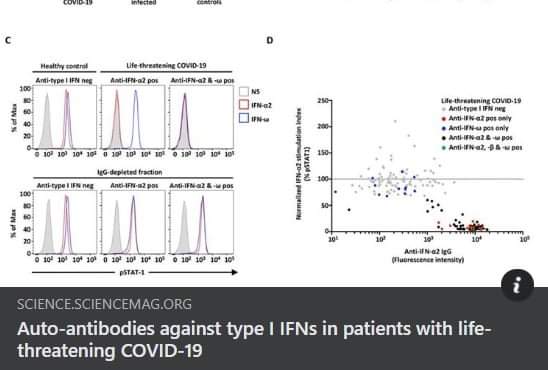
https://science.sciencemag.org/content/early/2020/09/23/science.abd4585
Zdaj je vse jasno! Najnovejše raziskovanje objavljeno v Science, kjer so pri umrlih od korona prehlada COVID-19 odkrili protitelesa na interferon (to je nova avtoimunska bolezen, imenujemo jo avtoimunska bolezen interferonske signalizacije, ABIS!), zaokroža zgodbo o cepivih! Znano je, da so umrli od COVID-19 večinoma bili starejši ljudje s kroničnimi boleznimi, ki so se zelo verjetno v letih odzivali na pozive Hrvaškega zavoda za javno zdravje, da bi se cepili proti sezonski gripi! In oni so to tudi naredili!
Pri vsaki okužbi, zlasti pri LAŽNI in DOLGOROČNI, ki se inducira z cepivom, organizem poskuša locirati okužbe z kompleksnimi mehanizmi IMUNOLOŠKEGA NADZORA, s čimer se pojavi fragmentiranje in analiziranje VSEH proteinov, ki proizvajajo VSE CELICE (ne pozabimo, da se inficirane celice proizvajajo tudi virusne beljakovine). To je EDINI NAČIN, s katerim prilagodljivi imunski sistem lahko SPECIFIČNO prepozna neznano, a nepoznano lahko postane tudi spremenjeno lastno tkivo (kot pri tumorju), in celo podrobnosti lastnega, ki ga imunološki sistem med fetalnim razvojem ni opazil in se ga je tako naučil tolerirati!
V opisani situaciji imunskega nadzora imunski sistem preveri VSE in seveda strukturno pravilnost lastnih signalnih molekul, vključno z interferonom! In prav z interferoni VSE CELICE (razen eritrocitov) intenzivno komunicirajo med seboj in iščejo okužbo tako, da aktivirajo na stotine genov, da se pred njo branijo. Imunologi dobro vedo, kaj je predelava in predstavitev antigena! Brez tega ni imunskega nadzora, nobene posebne obrambe.
No, vse je pod nadzorom interferona!
In končno, pri nekaterih ljudeh imunski nadzor pri cepljenju zaradi mobinga očitno "najde" napako - v interferonu!
In potem se zgodi, da namesto, da bi jih cepivo varovalo pred gripo, ostanejo zaradi cepiva "brez" interferona, BREZ OBRAMBE PRED VSEMI VIRUSI.
Zdaj še ne morem, a prva stvar, ki jo bom naredil, ko se vrnem v Zagreb, bo pismo vladi, opoziciji, poslancem, ministru za zdravje, hrvaški zdravniški zbornici itd., da epidemiološko "evidentiram" starejšo populacijo, zlasti v domovih za ostarele in nemočne, glede ABIS, natančno tako, kot je opisano v Science. Če testi še niso na voljo v prodaji, jih bom naredil sam, kot že tolikokrat. Takoj morate preveriti tudi zdravstveni karton umrlih zaradi prehlada, ali in koliko so bili cepljeni s cepivi proti sezonski gripi!
Namesto na stotine milijonov kun, ki jih dobesedno vržemo na RT-PCR za določitev COVID-19 pri zdravih ljudeh, bo za določitev ABIS, za določitev SMRTNO OGROŽENIH, potrebno komaj nekaj sto tisoč kun!
Podpisal dr. Srećko Sladoljev, nekdanji predstojnik Laboratorija za molekularno biofiziko, predstojnik Laboratorija za tehnologijo hibridoma, predstojnik Oddelka za imunodiagnostiko, predstojnik Oddelka za naravni interferon, svetovalec uprave in vodja razvojno-raziskovalne službe na Imunološkem inštitutu v Zagrebu.
Vir: https://dokumentarac.com/covid-19/umrli-od-korone-su-stari-i-bolesni-ljudi-koji-su-godinama-cijepljeni-protiv-gripe/
Drugo, radi se o važnom otkriću objavljenom prije mjesec dana u Science. U njemu je sudjelovalo preko sto znanstvenika iz osamdesetak instituta cijelog svijeta. Kod velikog broja umrlih otkrivena su autoprotutijela protiv interferonske signalizacije što je blokiralo sve prirodne načine obrane od virusa. Takvi ljudi su u najvećem riziku. Otkriće je ubrzo potvrđeno i laboratorijski u „in vitro“ uvjetima i nedavno objavljeno u Nature.
S Koronom stradaju, to se zna, starije osobe s kroničnim bolestima. Baš ti, godinama se uporno cijepe protiv gripe kako im preporučuje struka. Cjepiva su izvan svake sumnje okidač za autoimune bolesti. Vjerujući da će im cijepljenje pomoći, ovi ljudi čine sebi gore. Povećavaju rizik da cjepivima obole od autoimune bolesti interferonske signalizacije. Više je epidemioloških studija napravljeno u Italiji, Francuskoj i Njemačkoj. Sve su potvrdile kako je među umrlima od Covida -19 najviše bilo onih cijepljenih protiv gripe!
* * *
Ali so cepiva za gripo povzana s smrtmi, pripisanimi COVID-19 v drugem valu pandemije?
* * *
UK Medical Freedom Alliance o agendi cepljenja proti COVID-19
Angleška zveza za medicinsko svobodo je 23.11. 2020 naslovila odprto pismo (47) na regulatorno agencijo za medicinske produkte (MHRA), Združen odbor za cepljenje in imunizacijo (JCVI) in Državnega sekretarja za zdravstveno in socialno oskrbo Matt Hancock-a v zvezi s promocijo, ponudbo in dajanjem cepiv proti COVID-19 v Veliki Britaniji. Zapisali so med drugim:
Predlaga se sočasno dajanje cepiva proti gripi s cepivom Covid. To bi lahko povzročilo nadaljnja varnostna vprašanja, saj ta kombinacija cepiv ni preizkušena in dokazano varna in učinkovita, če se daje skupaj. Znano je, da cepivo proti gripi izziva imunski sistem cepiv in jih lahko začasno ogrozi zaradi drugih okužb zgornjih dihal (brez gripe), vključno s koronavirusi. Obstajajo tudi dokazi, da lahko cepiva proti gripi pri starejših povečajo smrtnost zaradi Covid-1934.
* * *
prof. dr. Dolores Cahill
Hidroksi klorokin je zelo varno zdravilo za malarijo že 50 let in lahko se daje otrokom, starejšim, nosečnicam in doječim materam. Deluje proti koronavirusom in tudi proti virusom gripe, zato ni potrebe po cepivu za gripo. Starejši lahko vzamejo preventivno 100 mg hidroksi klorokina, polovična doba razpada je 3 tedne. Tudi druga populacija lahko uporablja to uspešno zdravilo, ki deluje tudi proti mutiranim inačicam koronavirus SARS CoV-2. Donald Trump je govoril o tem zdravilu. Zato ni potrebe po cepivu proti COVID-19.
1.03.20 min: In zakaj je toliko ljudi umrlo v Bergamu? Oktobra 2019 so prejeli cepivo za gripo, v katerem je bilo pasje tkivo s koronavirusi - razdelili so 185.000 odmerkov. Starejši v Bergamu so prejeli decembra 2019 tudi cepivo za pneumokoke in meningitis in potem so dobili koronavirus SARS CoV-2 in imeli so »priming« (prekomerno stimulacijo imunskega sistema). Študija je pokazala, da je tkivo ledvic v cepivu za gripo povzročilo virusno interferenco – Gregg Wolff je po povedal v Pentagon študiji in to sem omenila v prvem intervjuju z Del Bigtree-jem maja 2020. Zgodil se je virusni »priming«, zaradi katerega je veliko cepljenjih vojakov imelo neželene posledice. Farmacevtska industrija lahko ljudem s cepivi povzroči virusni »priming«. V Bergamu so imeli zato veliko smrti.
1.05.00 min: Potrebujemo tudi obdukcije, kajti če nekdo umre zaradi virusne infekcije, ima vnetje v ustih, grlu, na vrhu pljuč, zlasti če je oseba starejša. Če pa umre zaradi virusne interference koronavirusa in mRNA cepiva ali zaradi koronavirusov iz pasjega tkiva v cepivu za gripo, potem bodo cela pljuča enomerno vneta, ker je prišlo do avtoimunske bolezni z napadom na pljuča. In bo vnetje v celih pljučih. Tako lahko razlikujemo virusno interferenco zaradi cepiv od naravne smrti zaradi COVID-19. Drugi razlog zakaj potrebujemo obdukcije je, ker bodo starejši ljudje umirali zaradi odpovedi organov in obdukcija bo razlikovala med odpovedjo organov zaradi cepiva mRNA ali cepiva za gripo od smrti zaradi naravne okužbe s SARS CoV-2. Oni to imenujejo smrti zaradi COVID-19 koronavirusa SARS CoV-2, a brez obdukcije. Zato ne delajo obdukcij, ker to, kar oni imenujejo COVID-19 simptomi, se bo z obdukcijo spremenilo. V marcu in aprilu 2020 so bile prave smrti zaradi SARS CoV-2 virusa, potem pa je prihajalo do virusne interfernce zaradi cepiv (za gripo) in v letu 2021 in 2022 bodo smrti zaradi odpovedi organov.
https://www.youtube.com/watch?v=vca1uVerXGQ&feature=youtu.be
https://publishwall.si/narava.zdravi/post/558680/irska-prof-dr-dolores-cahill-pandemije-covid-19-ni
* * *
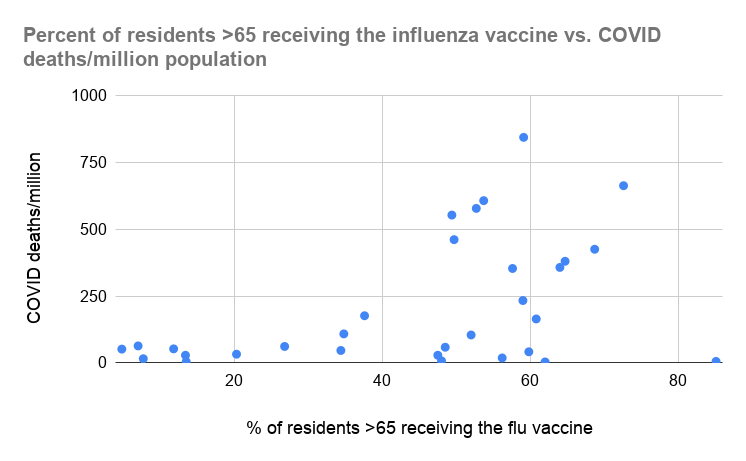
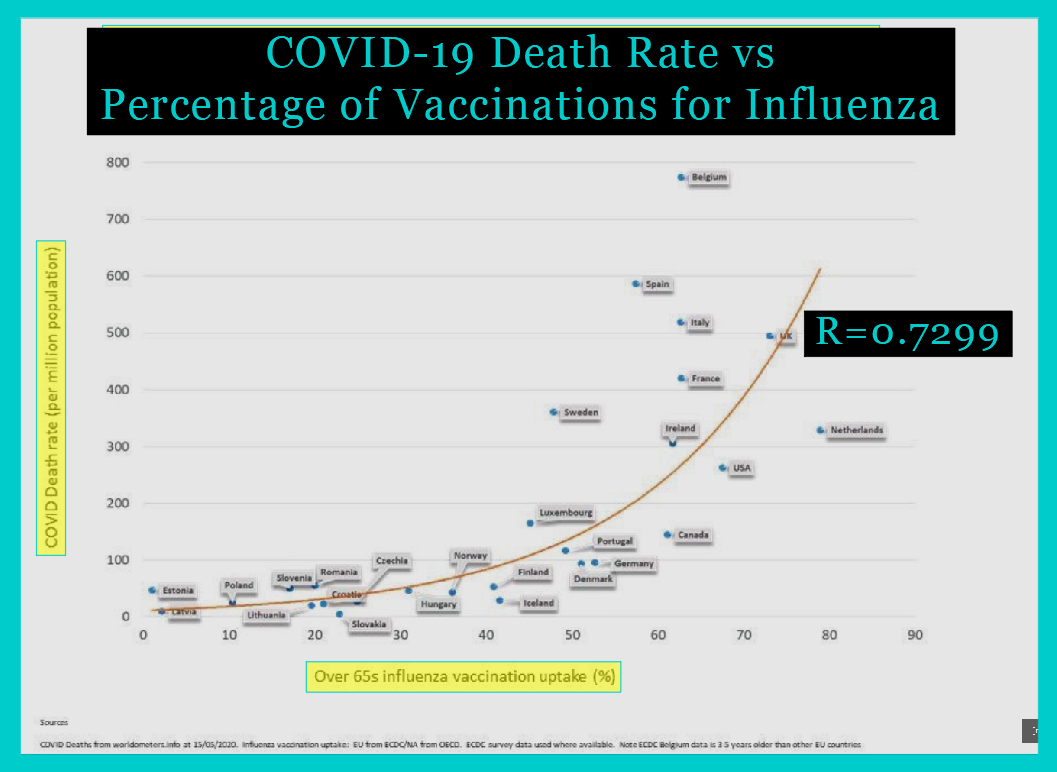
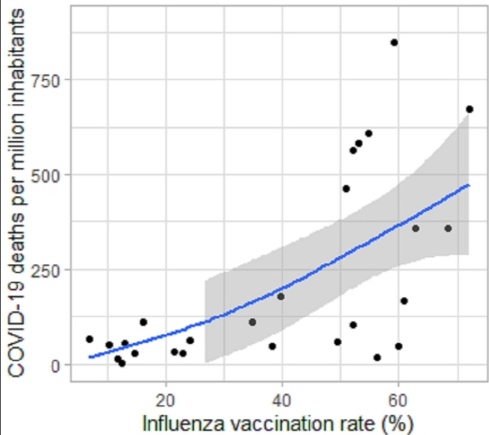
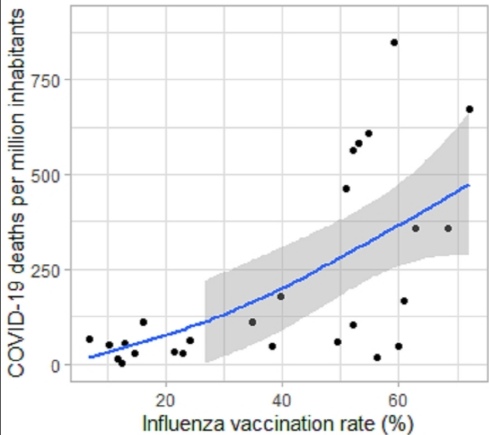
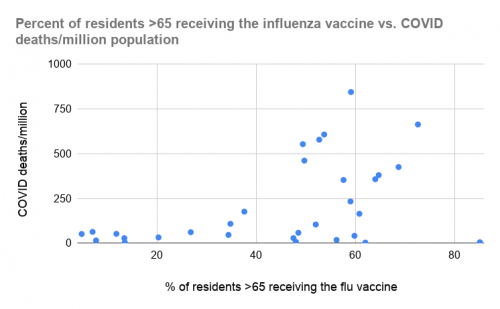
Pozitivna povezava med smrti COVID-19 in stopnjo cepljenja proti gripi pri starešjih ljudeh po vsem svetu:
Rezultati so pokazali pozitivno povezavo med smrtjo zaradi COVID-19 in stopnjo precepljenosti z cepivom za gripo pri osebah nad 65 let ( ≥ 65 let). Število smrtnih primerov zaradi COVID-19 se znatno povečuje od vzhodnih do zahodnih regij na svetu. Za razlago je potrebno nadaljnje raziskovanje te ugotovitve in dodatno delo na tem področju raziskav lahko privede do preprečevanja smrti, povezanih s COVID-19
https://www.researchgate.net/publication/344270570_Positive_association_between_COVID-19_deaths_and_influenza_vaccination_rates_in_elderly_people_worldwide
*
Nobelov nagrajenec in virolog prof.dr. Luc Montaigner: cepivo za gripo pospeši smrt zaradi COVID-19 zaradi virusne interference:
https://www.youtube.com/watch?v=o9VDarILtWc&feature=emb_logo
Dr. Luc Montagnier »Smo v norem svetu«
Prevod zadnjega vprašanja / odgovora:
Vprašanje: Ali verjamete, da bomo čez nekaj tednov ali mesecev dobili cepivo? Cepivo bo obvezno. Kaj mislite o tem?
Odgovor: Nisem nasprotnik cepljenja, niti nisem proti farmaciji, saj so naredili dosti dobrega.
Sprašujem, zakaj se osredotočajo na cepivo? Ker je tudi tukaj v ospredju, dobiček .
Problem je v tem, da so včasih cepiva slaba.
Poudariti in jasno povedati je treba, da cepljenje proti gripi pri človeku, ki je okužen s covid 19, lahko pomeni njegovo smrt v nekaj dnevih ali tednih.
Enako velja za nekoga, ki ima stabilno kemoterapijo za zdravljenja raka. Če ga cepite proti gripi, ga boste hitro ubili. To je treba povedati.
Ponovim naj, da je cepljenje lahko dobro ali slabo. Za te ugotovitve je potreben čas.
Imamo primer v Severni Italiji. Kjer so cepili ljudi proti meningitisu, je bilo največ mrtvih. To je zelo pomembno. Cepljenje v namen zdravljenja ne sme ubijati ljudi. Zdravniki ki cepijo, pozabljajo Hipokratovo prisego. Zdravniki morajo postaviti etično mejo.
*
https://www.theguardian.com/world/2020/oct/22/doctors-in-south-korea-call-for-flu-vaccinations-to-be-paused-after-25-deaths
V Južni Koreji je po prejemu cepiva za gripo umrlo že 83 ljudi
http://www.koreaherald.com/view.php?ud=20201031000051
*
Južna Koreja: Lani 1500 in letos že 48 mrtvih po cepljenju proti gripi
Manj znano je, da je v Južni Koreji lani, torej izven razmer pandemije umrlo kar 1500 oseb v tednu potem, ko so prejeli cepivo. Kakor navajajo korejski mediji: »Agencija za nadzor in preprečevanje bolezni je objavila rezultate zbiranja podatkov Državnega statističnega urada in dejala, da je približno 1500 ljudi, starih 65 let ali več, umrlo v enem tednu po tem, ko so v lanskem obdobju cepili gripo.«
Reuters pa za letos oktobra poroča o številiki 48 oseb, ki so umrle zelo kmalu po cepljenju proti gripi. Kljub temu se marsikje množična cepljenja proti gripi nadaljujejo. Čeprav so tudi v Južni Koreji nekateri zdravniki pozvali k ustavitvi množičnega cepljenja prebivalstva proti gripi, se državni program nadaljuje.
*
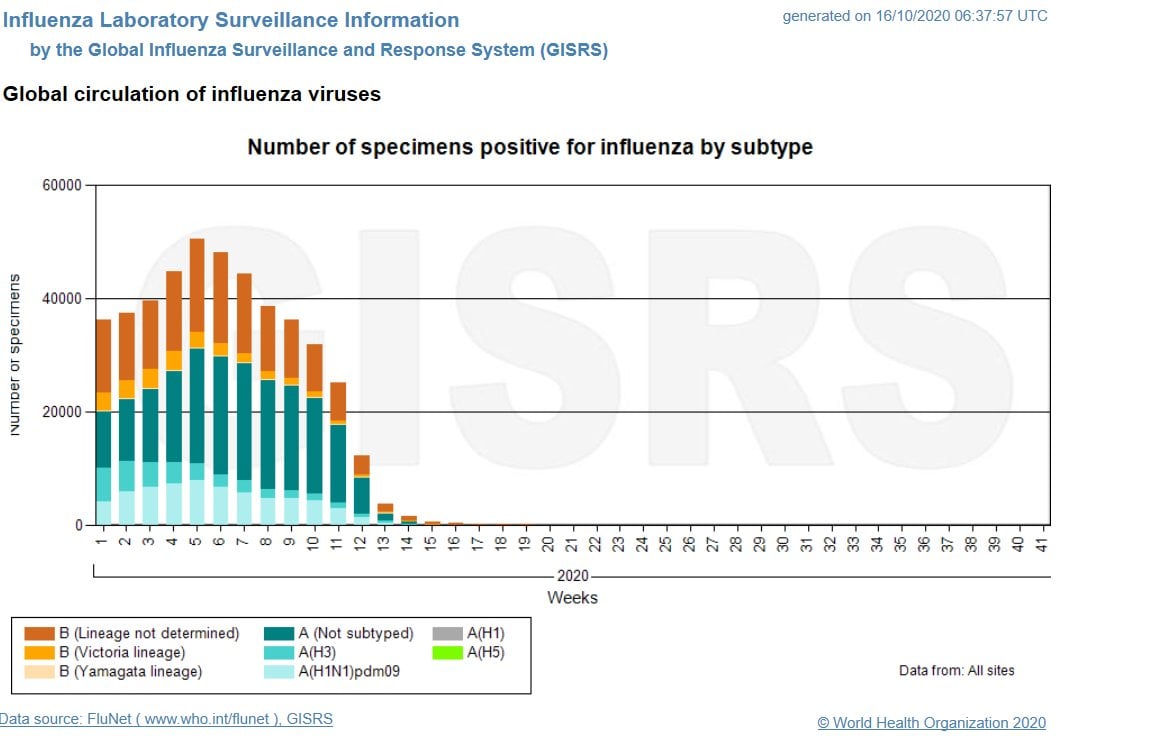
Po podatkih Svetovne zdravstvene organizacije letos po pojavu pandemije COVID-19 nihče v svetu ni zbolel zaradi gripe:
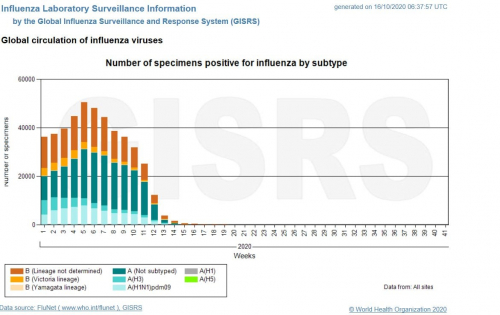
To postavlja dvoje vprašanj:
1. Ali so oboleli za gripo v letošnjem letu prišteti med COVID-19 bolnike, kar umetno napihuje število obolelih zaradi koronavirusa SARS CoV-19 in daje lažne statistične podatke?
2. Če po podatkih WHO gripe ni več, čemu je potrebno cepljenje proti gripi, ki povečuje smrtnost zaradi COVID-19?
* * *
2/3 odškodnin izplačanih v ZDA je zaradi škodljivih posledic cepiva za gripo
*
Dve ločeni, toda podobni študiji: znanstveniki so odkrili, zakaj je COVID-19 za nekatere ljudi smrtonosen
Kot ključen se je pokazal protein interferon tipa I, ki preprečuje širenje infekcije v telesu, a pri nekaterih ljudeh ne deluje pravilno.
Znanstveniki že mesece poskušajo razumeti koronavirus in bolezen COVID-19, in zakaj je okužba z virusom zelo nevarna za nekatere ljudi, za druge pa je na nivoju sezonske gripe. Tudi mladi ljudje lahko v nekaj dneh umrejo zaradi komplikacij, povezanih s koronavirusom.
Dve novi študiji sta bili objavljeni u časopisu Science in zdi se, da dajeta odgovor na to ključno vprašanje. Identificirali sta namreč ključni mehanizem v imunskem sistemu, ki lahko pojasni, zakaj je COVID-19 smrtonosen samo za nekatere ljudi in zakaj so moški bolj prizadeti.
Obe študiji poudarjata pomen interferonov tipa I (IFN), ki so ključni za to, kako se bo infekcija s koronavirusom končala za neko osebo. Interferon I so proteini, ki jih proizvajajo okužene celice, da bi zaustavile širenje infekcije. Študiji sta odkrili, da je proizvodnja teh proteinov pri nekaterih ljudeh prekinjena.
V eni študiji so odkrili, da ima več kot 10% zdravih ljudi, ki so zboleli s težko obliko COVID-19, v svojem telesu protitelesa, ki napadajo lastne interferon I proteine in jih tako onemogočajo v borbi proti koronavirusu. Druga študija je odkrila, da imajo nekateri ljudje genetsko mutacijo, ki onemogoča pravilno funkcioniranje interferona.
Ta odkritja dajejo nedvoumne dokaze, da je motenje funkcioniranja interferona tipa I ključno za razvoj bolezni COVID-19, je povedal zdravnik Jean-Laurent Casanova iz Univerze Rockefeller in dodal, da obstajajo zdravila, ki lahko rešijo ta problem.
Velika mednarodna ekipa znanstvenikov, ki so sodelovali z Casanovo, je identificirala protitelesa, ki nevtralizirajo interferon proteine pri najmanj 101 bolnikih med 987 bolniki, obolelimi za COVID-19.
Vsaj 94% bolnikov s temi nevtralizirajočimi protitelesi so moški, kar bi lahko pojasnilo, zakaj so moški bolj dovzetni za težjo obliko COVID-19, je pojasnil Stuart Tangye.
V drugi študiji so znanstveniki odkrili gene za interferonske proteine, ki delujejo proti bolniku, odkrili so 13 abnormalnosti v genetski kodi za interferone, ki so ključni za boj proti gripi.
A whimsical suggestion: correlate influenza vaccine uptake with Covid-19 frequency
Reference has been made to the possibility that influenza vaccines increase the risk of coronavirus infections (Wolff, Vaccine 2020;38:350) and that this might be relevant to Covid-19 infections (www.bmj.com/content/368/bmj.m1089/rr-10).
Furthermore, students of the subject have been perplexed about the wide geographic variation in the frequency and death rates of Covid-19.
I suggest that we look at influenza vaccine uptake in the elderly and Covid-19 death rates in European countries, using existing data. One source for vaccine data: OECD (2020), Influenza vaccination rates (indicator) doi:10.1787/e452582-e (Accessed on 21 May 2020). This lists, by country, the % of the population aged 65+ for 2018 or the latest available year. For Covid-19 death rates by country as of 21 May 2020: www.worldometers.info/coronavirus.
% INFLUENZA VACCINATIONS IN THE ELDERLY/COVID-19 DEATHRATES PER MILLION
Czech Republic 20.3/28 Lithuania 13.4/22
Denmark 52.0/97 Luxembourg 37.6/174
Estonia 4.8/48 Netherlands 64.0/337
Finland 48.4/55 Norway 34.4/43
France 49.7/431 Portugal 60.8/125
Germany 34.8/99 Slovak Republic 13.0/5
Hungary 26.8/49 Slovenia 11.8/51
Ireland 57.6/319 Spain 53.7/596
Italy 52.7/535 Sweden 49.4/384
Latvia 7.7/12 United Kingdom 72.6/531
To see if there is an association between the two factors find the correlation coefficient using a small hand calculator. Otherwise, make a scatterplot on a piece of graph paper…….Have fun!
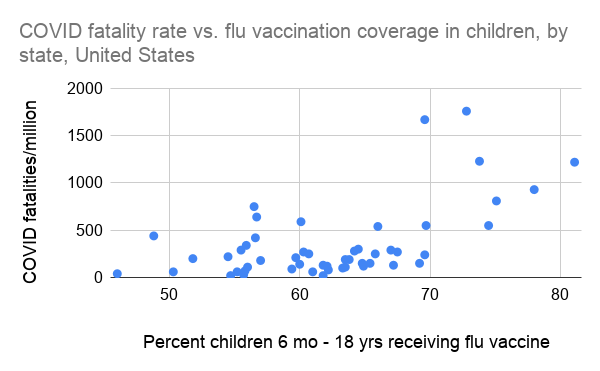
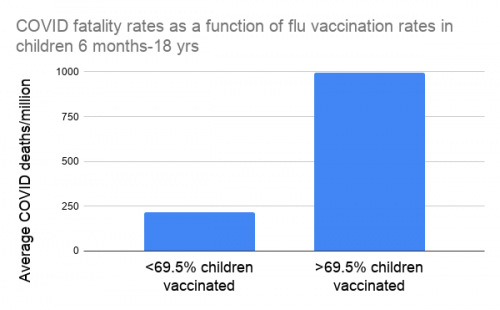
John Watkins is right; we need to think beyond containment, but he overlooks the possibility that seasonal flu shots are potential contributors to the current outbreak. (BMJ 2020;398:m810—February 28)….A randomized placebo-controlled trial in children showed that flu shots increased fivefold the risk of acute respiratory infections caused by a group of noninfluenza viruses, including coronaviruses. (Cowling et al, Clin Infect Dis 2012;54:1778) From Table 3, vaccine recipients had 20 noninfluenza virus-positive ARIs and 19 virus-negative ARIs; non-recipients had 3 noninfluenza virus-positive ARIs and 14 virus-negative ARIs. These figures yield an odds ratio of 4.91 (CI 1.04 to8.14).
Such an observation may seem counterintuitive, but it is possible that influenza vaccines alter our immune systems non-specifically to increase susceptibility to other infections; this has been observed with DTP and other vaccines. (Benn et al, Trends in Immunology, May 2013) There are other immune mechanisms that might also explain the observation.
To investigate this possibility, a case-control study is in order as we study and care for the victims of covid-19. Influenza vaccines have become sacred cows in some quarters, but they shouldn’t be.
Cepljeni proti gripi imajo 4,9 krat večje tveganje za okužbo s koronavirusi
https://www.bmj.com/content/368/bmj.m810/rr-0
Elizabeth Hart’s point about natural immunity is important, and it applies to influenza as well as coronaviruses. (BMJ rr 3/25/20) Annual flu shots have put us on a treadmill of narrow and short-term protection and subverted the broad and lasting immunity provided by wild virus infections in healthy people. Examples are accumulating of the harms done by influenza vaccines. (Cunningham, www.bmj.com/content/368/bmj.m626/rr) Now we have a study suggesting that they might increase mortality in the elderly. (Anderson, Ann Intern Med 3/3/20) The title and abstract are bland and innocuous, but Table 2 indicates that vaccines increase mortality from influenza and pneumonia by 17%. (vaccine effectiveness: minus 17.3 %, CI minus 40.7% to 6%) Furthermore, they increase the risk of illness from noninfluenza viruses, including coronaviruses. (Cowling, Clin Infect Dis 2012;54:1778. Wolff, Vaccine 2020;38:350)
Some vaccine experts worry that safe and effective coronavirus vaccines may not be possible, citing animal studies demonstrating “antibody-dependent enhancement” (ADE) of natural infection and the production of pulmonary immunopathology. (Jiang, “Don’t rush to deploy Covid-19 vaccines…” Nature 3/16/20. Takano, J Vet Med Sci 2019;8:911. Tseng, PLoS One 2012;7(4):e35421. Kam, Vaccine 2007;25:729)
The ominous forecasts about Covid-19 remind me of the “Seven-Step Recipe” for increasing demand for flu shots concocted by the CDC in 2004: “…statements of alarm by public health authorities…prediction of dire outcomes from influenza…continued reports that influenza is causing severe illness affecting lots of people…repeated urging of influenza vaccination…” (Doshi, BMJ 2005;331:1419) Sound familiar?
Purely natural immunity from measles brings with it substantial morbidity and mortality, and the imperfect herd immunity provided by the vaccine is a small price to pay to prevent them. Influenza and coronaviruses are a different matter. I am frightened and suspicious about the public decisions currently being made about Covid-19, and I am not alone.
https://www.bmj.com/content/368/bmj.m1089/rr-10
ALLAN S. CUNNINGHAM 21 May 2020Retired pediatrician
Nevarnosti cepiva proti sezosnki gripi pri COVID-19
V študiji, ki jo je napisal Greg Wolf iz US Armed Forces Surveillance (ameriškega nadzora oboroženih sil, podružnica letalskih sil) in ki je bila objavljena v reviji Journal, Vaccine, 10. januarja 2020, z naslovom "Cepljenje proti gripi in interferenca z respiratornimi virusi med osebjem ministrstva za obrambo v obdobju 2017- 2018". Za sezono gripe 2018 je bilo ugotovljeno, da je osebje ameriške vojske, ki je prejelo cepivo za zimsko gripo, imelo za 36% povečano možnost okužbe s drugimi respiratornimi virusi (op. prev.: kot je na primer koronavirus COVID-19).
https://www.ncbi.nlm.nih.gov/pubmed/31607599
https://www.disabledveterans.org/2020/03/11/flu-vaccine-increases-coronavirus-risk/
CDC Uses Flawed Science to Discredit Pentagon Flu Study
Widespread citation of the Pentagon study by health freedom advocates has prompted government and industry to discredit it — but the CDC is using a study that more resembles propaganda than sound science to make its case.
*
*Prije nego li se cijepite protiv GRIPE ne bi li se zaštitili od COVIDA-19 predlažem da barem prije pročitate sažetak slijedećeg peer reviewed znanstvenog istraživanja objavljenog 14. listopada 2020. godine.
PEER-REVIEWED
Positive association between COVID-19 deaths and influenza vaccination rates in elderly people worldwide
Pozadina
Pandemija koronavirusne bolesti 2019. (COVID-19), uzrokovana teškim akutnim respiratornim sindromom koronavirusom 2 (SARS-CoV-2), trajna je globalna zdravstvena kriza koja izravno i neizravno utječe na sve sfere ljudskog života. Predložene su neke farmakološke mjere za spriječavanje COVIDA-19 ili smanjenje njegove ozbiljnosti, poput cijepljenja. Prethodna izvješća pokazuju da se čini da je cijepljenje protiv gripe u negativnoj korelaciji sa smrtnošću povezanom s COVIDOM-19, možda kao rezultat heterolognog imuniteta ili promjena urođenog imuniteta. Razumijevanje takvih trendova u korelacijama moglo bi spriječiti smrt od COVIDA-19 u budućnosti. Cilj ovog istraživanja bio je stoga analizirati povezanost između smrtnih slučajeva povezanih s COVIDOM-19 i stope cijepljenja protiv gripe (IVR) kod starijih osoba širom svijeta.
Metoda
Kako bi se utvrdila povezanost između smrti od COVIDA-19 i cijepljenja protiv gripe, analizirani su dostupni skupovi podataka iz zemalja s više od 0,5 milijuna stanovnika (ukupno 39 zemalja). Da bi se točno procijenio utjecaj IVR na smrt od COVIDA-19 i ublažili učinci zbunjujućih varijabli, izvršeno je sofisticirano rangiranje važnosti različitih varijabli, uključujući kao prediktorske varijable IVR i neke potencijalno važne geografske i socioekonomske varijable, kao i varijable povezane s nefarmaceutska intervencija. Asocijacije su mjerene neparametarskim koeficijentima korelacije Spearmanova ranga i “Random Forest” funkcije.
Rezultati
Rezultati su pokazali pozitivnu povezanost između smrtnosti od COVIDA-19 i IVR osoba starijih od 65 godina. U svijetu postoji značajan porast smrtnosti od COVIDA-19 iz istočnih u zapadne regije. Dalje istraživanje je potrebno kako bi se objasnili ovi nalazi, a dodatni rad na ovoj liniji istraživanja može dovesti do prevencije smrti povezanih s COVIDOM-19.
Izvor:
https://peerj.com/articles/10112/
* * *
Cepljenje proti gripi povečuje število hospitalizacij in smrtnih primerov pri starejših osebah?
Opazovalna študija z dizajnom regresijke diskontinuitete
Zdravilna vrednost cepiva proti sezonski gripi ni ugotovljena. To dejstvo je ugotovila raziskava smrtnost starejših oseb v 14 letnem obdobju.
Tabela 2 kaže, da je cepivo za gripo povezano z 8,9% povečanjem smrtnosti zaradi vseh vzrokov pri starejših moških (VE-8,9%, CI -19,6% do 1,8%) in 26,5% porastom smrtnosti zaradi vnetja pljuč. (VE -26,5%, CI -56,1% do 3,0%)
The Effect of Influenza Vaccination for the Elderly on Hospitalization and Mortality
Izvorno istraživanje objavljeno 7. travnja 2020. godine
Pozadina:
Promatračke studije koje koriste tradicionalni dizajn istraživanja sugeriraju da cijepljenje protiv gripe smanjuje hospitalizacije i smrtnost starijih osoba. U skladu s tim, zdravstvene vlasti u nekim zemljama daju prednost cijepljenju ove populacije. Ipak, ostaju pitanja o učinkovitosti ove politike s obzirom na potencijal pristranosti i zbunjivanja u podacima promatranja.
Cilj:
Utvrditi učinkovitost cjepiva protiv gripe u smanjenju hospitalizacija i smrtnosti starijih osoba upotrebom promatračkog dizajna istraživanja koji smanjuje mogućnost pristranosti i zbunjivanja.
Dizajn:
Dizajn regresijskog diskontinuiteta primijenjen je na oštru promjenu stope cijepljenja u dobi od 65 godina koja je rezultat dobne politike cijepljenja u Ujedinjenom Kraljevstvu. U ovom su dizajnu usporedbe bile ograničene na osobe koje su bile blizu praga dobi od 65 godina i stoga su bile vjerovatno slične u većini vrijednosti, osim stope cijepljenja.
Provedeno:
Engleska i Wales.
Sudionici:
Odrasli u dobi od 55 do 75 godina koji borave na istraživanom području tijekom 2000. do 2014. godine.
Intervencija:
Cjepivo protiv sezonske gripe.
Mjerenja:
Stope hospitalizacije i smrtnosti prema mjesecu starosti.
Rezultati:
Podaci su obuhvaćali 170 milijuna epizoda njege i 7,6 milijuna smrtnih slučajeva. 65. godina života povezana je sa statistički i klinički značajnim porastom stope cijepljenja protiv sezonske gripe. Međutim, nijedan dokaz ne ukazuje da je cijepljenje smanjilo hospitalizacije ili smrtnost starijih osoba. Procjene su bile dovoljno precizne da isključe rezultate mnogih prethodnih studija.
Ograničenje:
Studija se oslanjala na podatke promatranja, a fokus joj je bio ograničen na osobe u dobi od 65 godina.
Zaključak:
Trenutne strategije cijepljenja koje daju prednost starijim osobama mogu biti manje učinkovite nego što se vjeruje u smanjenju ozbiljnog morbiditeta i smrtnosti u ovoj populaciji, što sugerira da bi mogle biti potrebne dodatne strategije.
Primarni izvor financiranja:
Nacionalni institut za starenje.
https://www.acpjournals.org/doi/10.7326/M19-3075
***
VPRAŠANJE ZA CORBETT: ALI OBSTAJA POVEZAVA MED CEPIVOM ZA GRIPO IN COVID-19?
https://www.corbettreport.com/is-there-a-flu-shot-covid-link-questions-for-corbett-068/
https://www.bitchute.com/video/LivqAJub4egS/ slovenski podnapisi
Pozdravljene gospe in gospodje,
dobrodošli nazaj k Corbett Report. Jaz sem vas gostitelj James Corbett iz corbettreport.com in vi poslušate vprašanje in ta teden bomo na d programu obravnavali vprašanje, ki prihaja iz komentarja na prejšnji seriji vprašanj z naslovom qfc 66: Kaj je WHO (Svetovna zdravstvena organizacija)?, ter iz oddelka za komentarje na strani corbettreport.com. Član Scott je napisal:
»Ohayo gozaimas James. Pred nekaj dnevi sem bral sem nekatere komentarje na videoposnetku Jason Bermus in našel sem komentar, ki je menil da obstaja povezava med cepljenjem v letu 2019 in COVID-19. Na žalost ni bilo povezave na dokaze o tem. Pomislil sem, da sem prejel cepivo za gripo novembra in je moj krvni test v decembru je pokazal zvišanje tumorskih markerjev, prvič po moji operaciji. Septembra 2017 sem imel rak žolčnih vodov. Tumorski markerji so še naprej naraščali, čeprav moje CT ali PET skeniranje ni pokazalo nobenega tumorja. Ženo mojega zdravnika sem vprašal, ali je to dvoje lahko povezano, a ona je menila, da to ni možno. Ali ste vi kaj slišali o tej povezavi med cepljenjem v letu 2019 in COVID-19. Kaj vi menite o tem? Jai mata. Scott.«
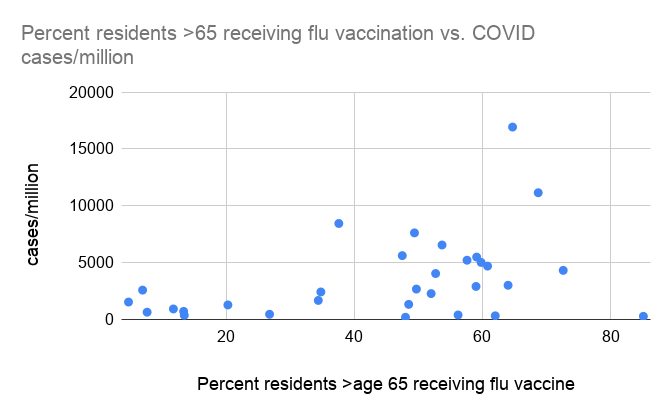
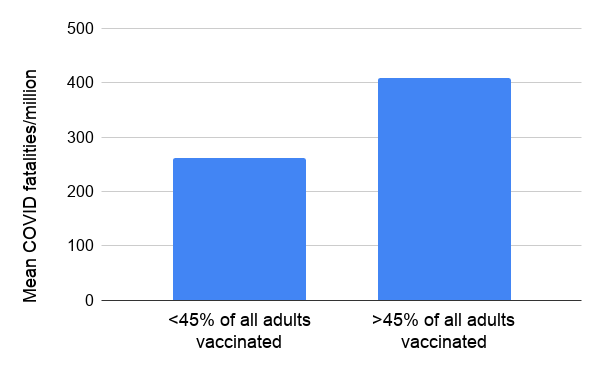
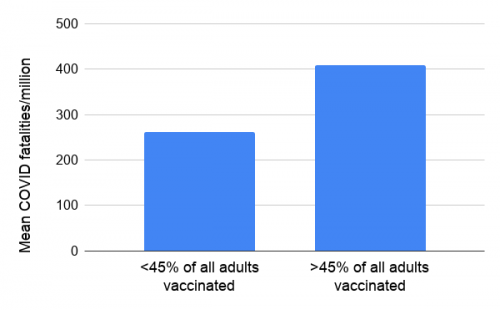
Hvala za vprašanje Scott in za dodatno japonščino. Zdi se mi, da sta dva dela tega vprašanja. Prvi je povezan z vašimi tumorskimi markerji, drugi pa je v zvezi s povezavo ali korelacijo med cepljenjem za gripo v letu 2019 in COVID-19. Za drugi del nimam le mnenja, temveč dejanske povezave, dokumente in dokaze o katerih lahko govorim. Usmeril bom vašo pozornost na članek z imenom Cepivo proti gripi in COVID-19 , za katerega mislim, da je vreden vaše pozornosti, ne le ker ima dobre raziskave, ampak še bolj pomembno, ima vse dokumentirano- dvakratno podčrtana ta beseda. Ima povezave na uradne medicinske znanstvene revije, ki dokumentirajo vse kar trdijo v tem članku. Pojdimo k povzetku na vrhu tega članka, kjer piše: Injekcija proti gripi- fatalna infekcija. Nadalje pravijo, da je deset držav z najvišjo stopnjo smrtnosti zaradi COVID-19, po podatkih Johns Hopkins Univerze: Belgija, Peru, Velika Britanija, Španija, Italija, Čile, Švedska, ZDA, Mehika in Francija in da je vsaka od teh držav injicirala več kot 49% starejše populacije s cepivom za gripo. To je v nasprotju z državami z najnižjo stopnjo smrtnosti zaradi COVID-19, kot so Ruanda, Tajska, Mozambik, Šri Lanka, Papua Nova Gvineja, Uganda, Tanzanija, Tajvan in Vietnam, ki z izjemo 49% cepljenja na Tajvanu, imajo izjemno nizko stopnjo cepljenja proti gripi. Tako je veliko različnih stvari, ki jih lahko izpostavimo kot potencialne vzroke za to in na primer nekdo lahko trdi, da te države nimajo dovolj kapacitet za testiranje, toda skrbna serološka študija več držav v Afriki je pokazala, da čeprav je bilo mnogo primerov pogrešanih, je to zato, ker prebivalstvo dejansko ni bilo zelo bolno. Zato tudi visoko število primerov najdenih protiteles, o katerih poročajo serološke študije, vzamemo kot študije z omejeno vrednostjo. Vendar tudi če upoštevamo to manipulirano statistiko, lahko pokažemo, da obstaja direktna korelacija med visoko pokritostjo s cepivi za gripo in visoko smrtnostjo zaradi COVID-19. Na veliko načinov lahko razložimo, kaj to pomeni. Najprej pa moramo pokazati korelacijo in to je namen tega članka z veliko podatki, ki prihajajo iz uradnih zdravstvenih virov. Pomembno je poudariti, da ta članek uporablja dejansko statistiko, ki jo sporočajo zdravstvene agencije in Johns Hopkins Univerza in drugi uradni viri. In z uporabo teh številk, za katere vemo, da so manipulirana statistika, lahko pokažemo korelacijo med umrlimi zaradi COVID-19 in stopnjo pokritosti s cepljenjem za gripo. To lahko ugotovimo tudi z uporabo teh manipuliranih številk.
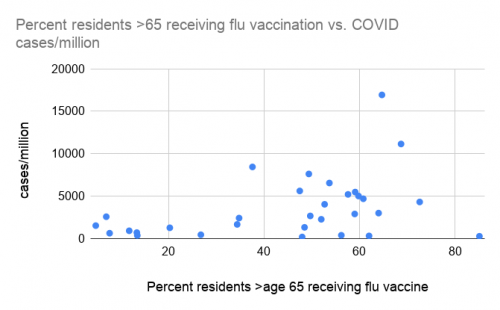
Če želite izvedeti več o manipulaciji številk, pojdite na corbettreport.com/coronastats, kjer je moja oddaja o lažeh, prekletih lažeh v koronavirusni statistiki, ko so celo pred nekaj meseci mnogi epidemiologi in drugi izpostavili očitne statistične napake, ki so bile narejene namenoma, da bi povečali t.i. COVID-19 krizo. A tudi če vzamemo te številke takšne kot so in uradne znanstvene študije, lahko pokažemo korelacijo med pokritostjo s cepivi za gripo in smrtnostjo zaradi COVID-19 in to so naredili v tem članku. Prične se z nizko stopnjo smrtnosti zaradi COVID-19 v državah z nizko stopnjo pokritosti s cepivi za gripo. Podatke so vzeli iz mnogih držav po vsem svetu in pokazali so, da je pri vsakem primeru COVID-19 smrti na milijon ali smrti, ki so pripisane COVID-19 na milijon in ki presegajo 250, vsak tak primer imel najmanj 49% pokritost s cepivi za gripo za njihovo starejšo populacijo. Na to so pogledali iz različnih zornih kotov z različnimi tabelami in znova vas bom pozval, da sami preberete ta članek, da vidite iz katerih virov prihajajo podatki in kako so predstavljeni. V tem delu so zaključili, prvič: da države, ki imajo visoko pokritost s cepivi, so do julija 2020 utrpele najmanj 20 krat več smrti zaradi COVID-19 na milijon, kot države z nizko pokritostjo. In drugič: zdi se da obstaja vrh pri 45-50% pokritosti z cepivi za gripo, kar je pomembno, saj se pri tem vrhu zdi, da obstaja jasna povezava s povečano smrtnostjo, ki je pripisana COVID-19. Nad tem vrhom pa se zdi, da korelacije ni, tako da od 45-50% dalje lahko pričakujemo višjo incidenco smrti zaradi COVID-19, toda pri tem ni razvidna neposredna povezava s cepljenjem. To je pomembna točka, h kateri sem bom vrnil malo pozneje.
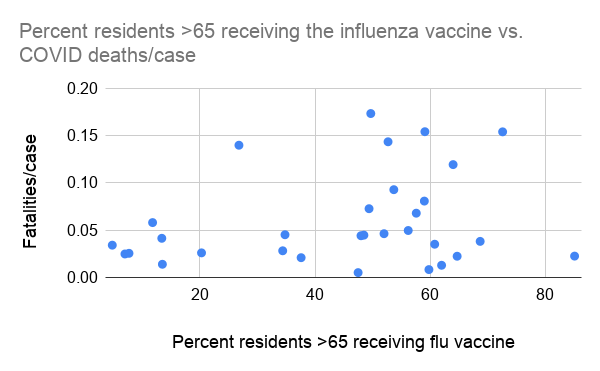
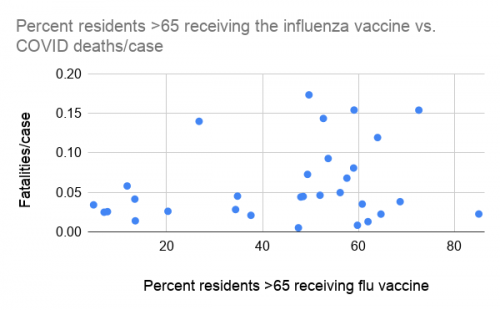
V nadaljevanju članek obravnava visoko stopnjo pokritosti s cepljenjem za gripo, ki lahko naredi individualno COVID-19 infekcijo bolj smrtonosno. Govori o tem, da se visoka smrtnost v primerjavi s številom primerov lahko izračuna ter da razen pri Madžarski (ki ima nizko pokritost, vendar edina uporablja aluminijev adjuvant v cepivu za gripo), je jasno razvidno, da je visoka smrtnost na število primerov v korelaciji z visoko pokritostjo s cepivi za gripo. To so prikazali v različnih diagramih, kjer lahko vidite jasno korelacijo in Madžarsko, ki je edina izjema. Kot razlagajo, je zadeva pri Madžarski drugačna, saj je edina država, ki uporablja aluminij kot adjuvant v svojih cepivih. Če ne veste, kaj je adjuvant, svetujem da se pozanimate, ker je take stvari izjemno pomembno vedeti v tej dobi bio-varnosti.
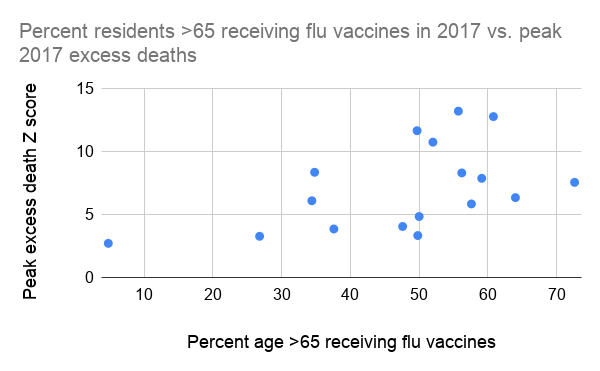
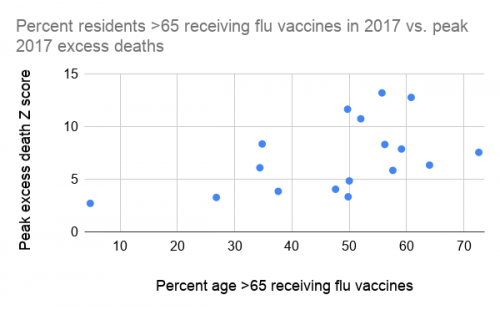
Potem govorijo o tem, da je cepivo za gripo povezano tudi s prekomernimi smrtmi v letu 2017 in pravijo, da je leta 2017 bila v Evropi nenavadno visoka presežna smrtnost v času sezonske gripe, ki jo je povzročil H3N2 virus gripe, ki ga večinoma ni bilo v cepivu. Kot je razloženo v nadaljevanju, cepivo za gripo lahko poveča dovzetnost za katerokoli okužbo in ne samo tisto, ki jo pokriva cepivo. Zato lahko pričakujemo povečano smrtnost v kateremkoli letu, posebno kadar nevaren patogen v obtoku ni specifičen sev v cepivu za gripo, kar se dogaja bolj pogosto, kot ljudje mislijo. In to se je zagotovo zgodilo leta 2017 in kot kaže diagram, je visok delež starejše populacije sprejel cepivo za gripo, kar je v direktni povezavi z visoko smrtnostjo zaradi sezonske gripe leta 2017. Torej ne gre le za nedavno cepljenje proti gripi in COVID-19, ampak morebiti za širši pojav, kajti čeprav korelacija ne pomeni vzročnosti, imamo korelacijo v različnih letih.
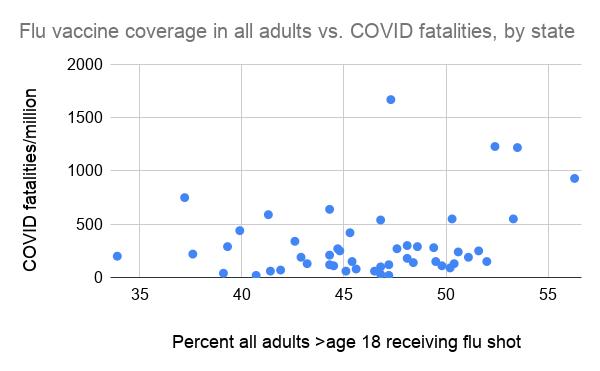
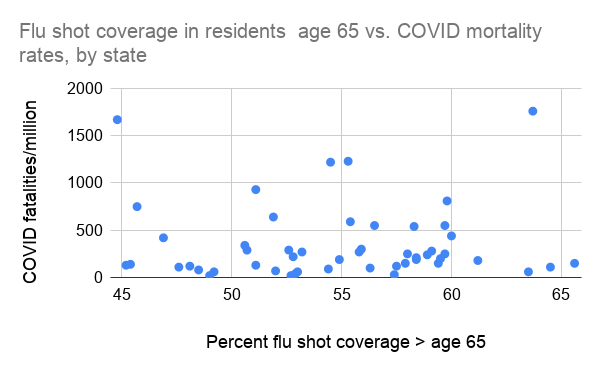
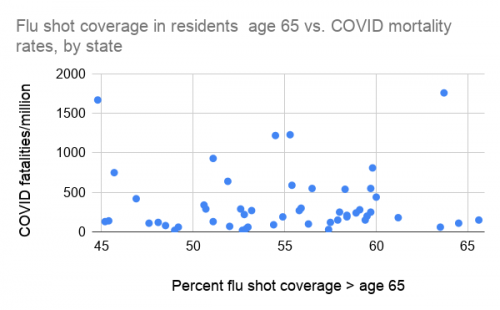
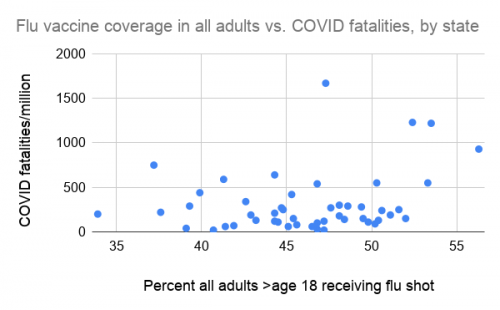
Dalje članek navaja, da je korelacija med pokritostjo s cepivi za gripo in smrtnostjo zaradi COVID-19 vidna tudi v ZDA, pri čemer je pomemben vrh, o katerem smo govorili. Vsaka zvezna država je imela najmanj 50% pokritost s cepivi za gripo v starejši populaciji in ker je to vrh, ni mogoče najti statističnega vzroca v državah, čeprav je bila 50% pokritost v primerjavi s 60% ali 70% pokritostjo. Ni statistično značilnih podatkov in ni mogoče najti korelacije, kar je povezano z idejo o vrhu iz prejšnjega diagrama. Imajo različne diagrame in grafikone, ki jih lahko pogledate, če želite več informacij o tem. To je zelo podroben članek z veliko povezavami in podatki, zato vas spet vabim, da ga preberete.
Poglejmo zdaj, kam to pelje in kaj to pomeni, kajti korelacijo lahko vidimo; obstaja statistična povezava, ki jo lahko prepoznamo kot visoko pokritost s cepivi za gripo med starejšo populacijo, povezano z visoko stopnjo smrtnosti, ki jih pripisujejo COVID-19. Kaj to pomeni? Ali obstaja vzročnost ali vsaj mehanizem, o katerem lahko ugibamo, kot o možnem vzroku. In odgovor je da. V članku to podrobno obravnavajo in zaključujejo v rumeno obarvanem delu članka, da cepivo za gripo ni bilo nikdar podprto z znanostjo, da gre za korupcijo in ne za javno zdravje, ko propagirajo cepljenje proti gripi. Potem se vprašajo, ali cepivo za gripo poslabša pandemijo gripe? To se nanaša na škandal z cepivom za svinjsko gripo leta 2009, o čemur sem govoril v moji objavi »Kdo je WHO?« V tem prejšnjem podcastu je več informacij o tem. Med sezono svinjske gripe leta 2009 je bila najdena korelacija med ljudmi, ki so prejeli cepivo za gripo v sezoni 2008-2009 in ljudmi, ki so potrebovali zdravstveno oskrbo zaradi svinjske gripe v času pandemije leta 2009. To pomeni, da ljudje, ki so imeli simptome in so potrebovali zdravstveno oskrbo v bolnišnici ali pri zdravniku zaradi te gripe, so bolj verjetno prejeli tudi cepivo za gripo v prejšnji sezoni. In tega ni ugotovila samo ena ali dve, temveč celo štiri opazovalne študije, ki so jih izvedli v Kanadi. Kot pri ostalih zadevah, ki jih obravnava ta članek, obstaja povezava na vir podatkov, ki kažejo te povezave.
Članek nadalje navaja, da so strokovnjaki za javno zdravje bili šokirani zaradi teh ugotovitev, a so molčali, ker je Big Pharma in njihove sponzorirane vladne agencije izrabile pozornost javnosti na gripo leta 2009, kot odskočno desko za še večjo promocijo programa cepljenja za gripo. Dali so povezavo na zanimiv članek, ki je vezan na zgodbo o pandemiji gripe in je v srcu tega vprašanja o varnosti cepiva za gripo in poročanju medijev o tem. Tu je pismo, ki je bilo objavljeno v britanski medicinski reviji »the bmj« in tu gre za uradno medicinsko znanost, saj to ni stran za teorije zarote ali kaj podobnega. Avtor je Alan S. Cunningham, upokojen pediater iz Cooperstown-a v New York-u, ki je napisal hiter odgovor glede poročanja v »the bmj« o znanosti na področju cepiv za gripo: Uradni dvolični govor skriva resne probleme glede varnosti in učinkovitosti cepiva za gripo. V tem članku dr. Cunningham piše: Po tednih premišljevanja o Donahue članku, ki povezuje cepivo za gripo s splavi (imamo povezavo ali vsaj referenco, ki jo bom dal na ta Donahue članek), sem čutil olajšanje, ko sem bral zgodbo Rona Wiponda o tem, kako mediji poskušajo skriti pod preprogo resna vprašanja glede varnosti cepiv. Poudaril je, da hinavščina oz. po njegovih besedah »dvojni standardi« oblasti, ki so zavrnile dokument Donahua, ker je to bila opazovalna študija. On navaja, da so leto za letom opazovalne študije oznanjale 80% učinkovitost cepiv, nato pa 60% in 40% učinkovitost, pri tem pa niso omenili, da te študije ne preučujejo škodljivih učinkov cepiv, kot so narkolepsija, epileptični napadi, vročica, okulorespiratorni sindorm. Ne omenjajo negativne učinkovitosti cepiv, povečanje tveganja za okužbe z virusi gripe in drugimi virusi, povezane ali povzročene zaradi cepiv. Ne omenjajo, da so cepiva lahko učinkovita v eni sezoni, a lahko povečajo tveganje za gripo v naslednji sezoni. Poglejte od protiteles odvisno okrepitev, da bi razumeli razlago mehanizma. Ne navajajo, da omenjene opazovalne študije verjetno pretiravajo glede učinkovitosti cepiv zaradi učinka zdravega uporabnika, ki ga epidemiologi dobro poznajo. Ta oseba je v bistvu povedala, da resna študija opozarja na resna vprašanja glede varnosti in učinkovitosti cepiv za gripo, a so jo znanstveni tolmači in znanstveni korporativni mediji, financirani od Big Pharma, zavrnili, z izgovorom, da je to zgolj opazovalna študija, ki ne dokazuje ničesar. Da v resnici ni znano in je veliko razlag za to. Našli so veliko izgovorov za zavrnitev teh študij, čeprav se tudi oni zanašajo na isto vrsto študij t.j. na opazovalne študije, ko oznanjajo na primer, da so bila cepiva bila letos 80% učinkovita in so rešila veliko življenj, zanemarijo pa druge pomembne podrobnosti.
Kot sem povedal, je v članku, ki ga lahko sami preberete, citiranih veliko referenc. Na koncu članka dr. Cunningham zaključi, da Wipond-ov članek daje nov vpogled starega zdravnika za dojenčke, ki je nekoč z vsem srcem zagovarjal cepiva, pozneje pa so ga razdražili dvolični govori avtoritet na področju cepljenja. Upa, da bo njegov članek pomagal k pošteni razpravi o varnosti in učinkovitosti cepiv za gripo. Žal je bilo to pismo objavljeno januarja 2018 v British Medical Journal, mi pa smo zdaj v septembru 2020 in obžalujem dejstvo, da odprte in iskrene razprave, ki jo je želel dr. Cunningham, še ni bilo. Tudi ne polagam upe v to, da se takšna razprava lahko zgodi v korporativnih znanstvenih medijih, ki jih financira Big Pharma. A pomemben del vsega je razlog, zaradi katerega ne samo ti Scott, ampak tudi zdravnik tvoje žene, ni nikoli slišal za to in ne pozna mehanizma, ki bi lahko pojasnil možne povezave med cepljenjem proti gripi in COVID-19 ali katero drugo boleznijo in ta razlog je, da tovrstni rezultati niso javno publicirani in na veliko razglašeni, tako kot hvalijo cepiva, da so varna in učinkovita. Te vrste študij oglašujejo in z njimi seznanjajo zdravnike. Zakaj se to dogaja?
In zaključna poanta tega članka, v katerem govorijo o povezavi med cepivom za gripo in COVID-19 je, da cepivo za gripo spodbuja tudi druge viruse. Kot smo že prej nakazali, leto 2009 ni bilo anomalija, ker cepivo za gripo rutinsko povečuje stopnjo okuženosti z drugimi patogeni, kar izniči kakršne koli koristi cepiva. Medtem so mnoge študije tega pojava bile opravljene na bolnikih, ki so se svobodno odločili, ali bodo sprejeli cepivo za gripo ali ne. Ena študija je zadostila zlatemu standardu zaslepljenega randomiziranega in s placebom nadzorovanega preizkusa. Medtem ko je bila splošno sprejeta hipoteza, da je mehanizem povečanja ne-gripoznih obolenj virusna interferenca, na podlagi opazovanja, da bolezen z eno vrsto virusa lahko prepreči druge, pa je Riken s sod. leta 2018 odkril, da se je povečanje ne-gripoznih obolenj pričelo 14 dni po prejemu cepiva za gripo, preden se je razvila imunost na gripo. To kaže, da podobno kakor cepivo za DTP in druga cepiva z neaktivnimi patogeni, tudi cepivo za gripo ustvari nespecifične spremembe imunskega sistema, ki povečajo dovzetnost za določene druge okužbe.
Večina študij o cepivu za gripo se je osredotočila na otroke ali pa je našla statistično pomembne rezultate le pri otrocih. Vendar pa je ena študija, ki je iskala učinke pri odraslih, ugotovila, da medtem ko se zdi, da je cepivo dalo navskrižno zaščito pred določenimi patogeni v tej populaciji, pa je precej povečalo dovzetnost za mnoge druge patogene, vključno s koronavirusi. Ta študija se je nanašala na prej znane koronaviruse in ne na SARS CoV-2. Potencial cepiva za gripo, da povečuje okužbo COVID-19, je bil jasno ugotovljen in kot smo prikazali, je to razvidno tudi iz podatkov o COVID-19. Upam, da zdaj razumete, zakaj vas nenehno usmerjam k temu članku, da bi sami poiskali vire podatkov. Samo v tem odstavku je navedenih veliko virov, ki je specifična strokovno pregledana in publicirana medicinska literatura, ki dokazuje vsako trditev v tem članku, vključno s študijo, ki je bila objavljena v Vaccine januarja 2020 z naslovom »Cepiva za gripo in interferenca respiratornih virusov med osebjem Ministrstva za obrambo v sezoni gripe 2017-2018«. Navaja, da sprejem cepiva za gripo lahko poveča tveganje zaradi drugih respiratornih virusov zaradi t.i. virusne interference, vendar zaključuje, da sprejem cepiva za gripo ni povezan z virusno interferenco med populacijo. Takoj nato pa trdijo nasprotno; da je bila virusna intereferenca zaradi cepiva za gripo znatno povezana s koronavirusi in človeškim metanemovirusom.
Opozorilo za trapaste teoretike zarot: ta študija je bila objavljena januarja 2020, izvedena pa je bila leto poprej. Ne nanaša se na COVID-19 SARS CoV-2, ki ga teoretično takrat še ni bilo. Ne govori o SARS CoV-2, ki je nov koronavirus, temveč o drugih vrstah koronavirusov; o prejšnjih, ki smo jih poznali. Vendar ja, cepivo za gripo je bilo znatno povezano z virusno interferneco, ki je dejansko povzročila okužbo s koronavirusi. Zato se zdi, da to zasluži nadaljnje raziskave, ne pa da to zanemarimo, ker naj bi bilo razkrito, da ni bilo govora o COVID-19 ali SARS CoV-2. Morda bi nekdo moral to raziskati, ali ne? Tudi to kaže na globoko nepoštenost v razpravi, o kateri je govoril dr. Cunningham v pismu reviji »the bmj«.
Flu Injection -- Fatal Infection : https://homevaccineeducationnetwork.com/flu-vaccine-and-covid-19
What connects the countries of Belgium, Peru, the UK, Spain, Italy, Chile, Sweden, the US, Mexico, and France? These countries, the top ten in COVID-19 mortality (as of August 24, 2020, according to Johns Hopkins), all injected more than 49% of their elderly populations with the flu vaccine. This stands in stark contrast to the countries on the low end, with fatality rates/popuation up to four orders of magnitude smaller: Rwanda, Thailand, Mozambique, Sri Lanka, Papau New Guinea, Uganda, Tanzania, Taiwan, and Vietnam - with the exception of a 49% vaccination rate in Taiwan, the flu vaccination rates in these countries is extremely low. While one might object that these countries may lack in testing ability, careful serological study of multiple countries in Africa has shown that while in fact many cases were missed, this is because the residents were in fact not very ill - while the number of individuals with COVID antibodies in Kenya, for example, was similar to Spain, the hospitals were never overwhelmed and excess deaths were not reported. However we look at the data - either between or within continents - higher rates of flu vaccination clearly appears to transform large numbers of COVID cases from mild to severe disease. As flu vaccines are being pushed aggressively and even mandated in fall 2020, it is critical for citizens and medical professionals to review the issue. Please read on for data, references, and sources.
Low COVID-19 fatality rates seen in countries with low influenza vaccine coverage
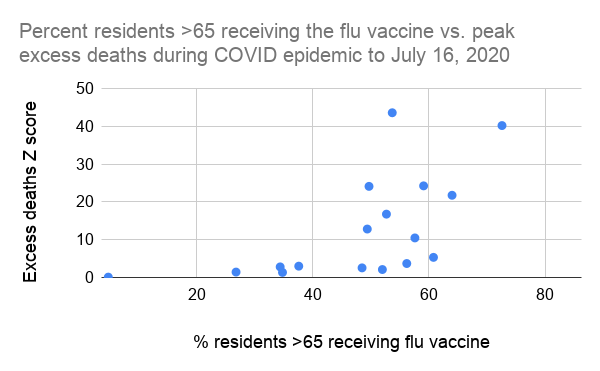
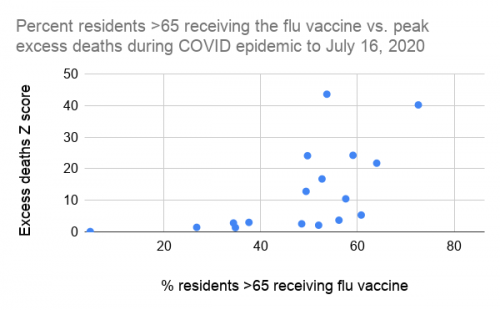
Cunningham( 2020)published a list of flu shot coverage rates in European countries vs. their COVID-19 fatality rates. His data is graphed below, updated through July 16 and supplemented with every other country for which we could find influenza vaccine data. This includes the United States, Canada, New Zealand, Japan, Iceland, Israel, and South Korea. Because COVID-19 testing and reporting may be inconsistent between countries, we also provide the peak total excess death rate since January of 2020, in the form of a statistical Z score for countries for which this was available. Full data and sources are given at the bottom of this article. All flu vaccine coverage data comes from 2019, if available, or 2018.
The Flu Shot: Never Supported by Science
In 1972, Dr. John Anthony Morris reported his research findings on the influenza vaccine to his superiors at the FDA. A distinguished doctor and government researcher, Dr. Morris had been comissioned 13 years earlier to scientifically justify the FDA's plans to widely expand the flu vaccination program. To his expectant audience, however, his results were thoroughly disappointing. Dr. Morris reported that the flu shot provided no measurable net benefit, in part because the injected product failed to stimulate antibody production in the lungs, thus allowing for viral replication in this sensitive area. It was later realized that the lack of benefit also derives from the flu shot's ability to increase vulnerability to viruses not covered in the shot, including unmatched strains of flu and different respiratory viruses dangerous in their own right. Dr. Morris' finding of no net benefit of the influenza vaccine has been repeatedly verified with contemporary data, including a study by Simonsen et al. (2005) that found that the large increase in flu vaccination of the elderly between 1980 and 2001 failed to decrease flu season mortality, and a study in Britain which found that the vast increase in flu shot uptake by those who had just turned 65 (vs. those who were just a bit younger) provided no decline in hospitalizations or deaths.
Given the powerful results of Dr. Morris' research, the flu vaccine's only perk could be to line the pockets of Big Pharma, and should have been regulated out of existence. Unfortunately, the cozy relationship between the FDA, CDC, and the pharmaceutical industry, well documented today, is not a new phenomena. Instead of reconsidering the vaccination program Dr. Morris' supervisors swiftly closed his laboratory and blocked publication of his results. Breathing a sigh of relief that good science would not be placed in the way of good profits, Big Pharma continued pushing for expansion of the flu shot market. Even if there wasn't a huge benefit in ordinary years, they argued, it was important to have manufacturing in place in order to churn out large quantities of vaccine quickly to save the world during the next serious pandemic (History of Vaccines, by Arthur Allen).
Enter 2009, the first major flu pandemic to occur after mass influenza vaccination had become a reality. Big pharma did indeed heroically turn out millions of doses of pandemic influenza vaccine. Unfortunately, most of the doses did not become available to the general public until after the pandemic was nearly over. In addition there was the inconvenient finding that individuals who had obediently taken the seasonal flu vaccine the year before were more likely to develop pandemic influenza illness that was medically attended. Public health experts were shocked by these findings but kept their lips sealed as Big Pharma and their sponsored government agencies used the public spotlight on the flu in 2009 as a springboard to push for an even larger flu vaccination program. For the first time the flu vaccine was recommended for every American citizen, especially children, who by 2020 were the largest consumers of the shot despite lack of evidence of benefit and the mercury that was allowed to remain in the vaccine.
The Flu Shot Makes A Flu Pandemic - Worse?
The Flu Shot Promotes Other Viruses
As alluded to above, 2009 was not an anomaly; the flu shot routinely increases the rate of infection with other pathogens, negating any benefits of the shot. While many of the studies of this phenomena worked with patients who had freely chosen whether or not to take the flu shot, (Dierig et al., 2014), one study met the gold standard of a blinded, randomized, placebo controlled trial (Cowling et al., 2012). While it has been generally hypothesized that the mechanism of the increase in non-flu illnesses is viral interference - the observation that illness with one virus may block others - it was found by Riken et al. (2018) that the increase in non-flu infections starts in the first 14 days after receipt of the flu vaccine, before any immunity to the flu has developed. This indicates that like the DTP vaccine and other innactivated pathogen vaccines, the vaccine engenders non-specific immune system changes which increase vulnerability to certain other infections. Most of the studies on the flu vaccine have focused on children, or found statistically significant results only in children, however one study to find an affect in adults found that while the flu shot appeared to offer cross protection against certain pathogens for this population, the vulnerability to several other pathogens, including coronavirus, was specifically increased. This study was with regards to "old" coronaviruses, not COVID-19. The potential of the flu shot to fuel COVID-19, however, was firmly established, and, as we demonstrated above, can now clearly be seen in the COVID data
https://www.bmj.com/content/360/bmj.k15/rr
Rapid Response:
Official doubletalk hides serious problems with flu shot safety and effectiveness
OFFICIAL DOUBLETALK HIDES SERIOUS PROBLEMS WITH FLU SHOT SAFETY AND EFFECTIVENESS
After weeks of brooding about the Donahue article linking flu shots to miscarriages (Vaccine 2017;35:5314) it was with a sense of relief that I read Rob Wipond’s narrative of media attempts to sweep a serious vaccine safety issue under the rug….He points out the hypocrisy (his words were “double standard”) of authorities who dismissed the Donahue paper because it was an “observational study.” Year after year they have quoted observational studies to announce, “…80% vaccine effectiveness…60% effectiveness…40% effectiveness…” They do not mention that these studies make no effort to look for adverse vaccine effects (e.g. narcolepsy, seizures, high fever, oculorespiratory syndrome). They do not mention “negative vaccine effectiveness”, the increase in risk of illness from influenza and non-influenza viruses associated with (or caused by) the vaccines. (Cowling, Clin Inf Dis 2012;54:1778) They do not mention that a vaccine “effective” in one season may increase influenza risk in a subsequent season. (Read about “antibody-dependent enhancement” to understand one explanatory mechanism). They do not mention that the observational studies they refer to are likely to exaggerate vaccine effectiveness in the first place because of the “healthy user effect” well known to epidemiologists.
Some history: 1960 Nobel Laureate and a primary developer of today’s influenza vaccine, Macfarlane Burnet, didn’t think it was worth much. (Br J Path 1936:17:282. Natural History of Infectious Disease 1972, page212)….In 2000 Kenneth McIntosh warned that we should not routinely give influenza vaccine to healthy children until multicenter randomized trials were done over several seasons to be sure that it was safe and effective. (Editorial, NEJM 2000;342:225) His advice was ignored….In 2004 a “Seven-Step Recipe” for using the media to boost demand for the vaccine was presented to the National Influenza Vaccine Summit, sponsored by the CDC and the AMA. The recipe included, “…statements of alarm by public health authorities…prediction of dire outcomes from influenza…continued reports that influenza is causing severe illness affecting lots of people…repeated urging of influenza vaccination…” (Doshi, BMJ 2005;331:1419) Sound familiar?
Peter Collignon and his colleagues have said this: “We need much larger, independent, and better-reported prospective studies that clearly demonstrate that the benefits of influenza vaccines in children far outweigh harms…If, overall, the increased number of cases of ARI plus vaccine side effects are much larger (in vaccine recipients) than those on placebo, given the low efficacy of the vaccine, then this is a strong argument against current policies advocating routine influenza vaccination of children.” (Collignon, Clin Inf Dis 2015:60:489)
In any discussion of influenza epidemiology we should acknowledge the careful and steady (one could even say fearless) work of Danuta Skowronski and her Canadian public health colleagues. It was they who found that the 2008-9 flu shot doubled the risk of illness from the 2009 H1N1 pandemic flu. Their observations were considered important enough to alter Canadian vaccine recommendations for the 2009-10 season. However, for some reason, they had a good deal of difficulty getting their study finally published. (Skowronski, PLoS Med 2010;7(4):e1000258) This observational study was a revelation, even a shock, to many public health experts. US officials never publicly acknowledged the findings…..This is just one of a number of important papers published over the years by Skowronski and her colleagues, who have a reputation for high scientific and ethical standards.
Wipond does not mention another technique used to dismiss legitimate vaccine safety concerns, having to do with “statistical significance.” Recently, a large cohort study found that flu shots given during the first trimester of pregnancy were associated with a 20% increase in autism spectrum disorder in the offspring. P for the association was 0.01, and the authors acknowledged that, if it was causal, would mean four(4) additional autism cases for every 1000 mothers vaccinated. However, they incorrectly used a statistical manipulation to adjust the finding into “non-significance.” (Hooker, Donzelli, Zerbo. JAMA Pediatr 2017;171:600) One typical media headline about the study was, “Flu vaccine during pregnancy not linked to autism.” (Shute, NPR, 11/28/16)….This kind of thing goes on all the time with news releases for vaccine research.
The flu season in North America officially began 5 weeks ago, and the vaccine publicity juggernaut is still picking up steam. Manufacturers are hoping to sell 166 million doses in the US this season. One business group predicts an $8 billion US influenza vaccine market by 2025. (Coherent Market Insights, 1/5/18) The 2016-17 vaccine increased the risk of H3N2 illness among UK elderly by 68%, and officials are calling for better vaccines. (Osterholm, NY Times, 1/8/18) Meanwhile, in the absence of any evidence that it would help, officials and ordinary citizens in the US and UK wrangle about flu shot mandates for healthcare workers.
Wipond’s article provided new insight for an old baby doctor who, at one time, was a wholehearted vaccine advocate, but lately has been exasperated by bullying and doubletalk from vaccine authorities. Let us hope that his article helps to sustain an honest discussion about the safety and effectiveness of influenza vaccines.
Allan S. Cunningham 1/9/18
Povezava splava s cepivom za gripo: https://pubmed.ncbi.nlm.nih.gov/28917295/
Influenza vaccination and respiratory virus interference among Department of Defense personnel during the 2017-2018 influenza season https://pubmed.ncbi.nlm.nih.gov/31607599/
Statistika o precepljenosti za gripo in incidenco COVID-19 https://drive.google.com/file/d/1IKt-PUVP06UXxfiTuNRQir64qCPJjG0l/edit
https://papers.ssrn.com/sol3/papers.cfm?abstract_id=3621446 COVID-19 Severity in Europe and the USA: Could the Seasonal Influenza Vaccination Play a Role? 16 Jun 2020 Our analysis indicates that receiving seasonal influenza vaccination(s) in the past might be an additional risk factor for the elderly in terms of enhanced susceptibility to infection with SARS-CoV-2 and higher likelihood of a lethal outcome in case of infection. More research about this possible risk factor is urgently needed.
Vir: https://qplusnews.com/correlation-coefficient-covid-deaths-qivc-flu-shots
• (2020.07.09) Flu Vaccination and COVID 19 risk – Dr. John Campbell
“Influenza vaccines may alter our immune systems non-specifically to increase susceptibility to other infections” https://youtu.be/utMREADbtAc
• (2020.08) Could Increases in Influenza Vaccination Rates Give Rise to Exponentially-Related Corresponding Increases in Mortality Rates From Covid-19? https://grahameb.com/diy_stats
• (2020.08.09) Hypothesis: Possible immune interference between Polysorbate 80 of the adjuvanted influenza vaccine and SARS-CoV-2 as a cause of coronavirus pandemic https://doi.org/10.5281/zenodo.4009604
• (2020.08.24) Proteins that contaminate influenza vaccines have high homology to SARS-CoV-2 proteins thus increasing risk of severe COVID-19 disease and mortality https://doi.org/10.5281/zenodo.3997694
* * *
What connects the countries of Belgium, Peru, the UK, Spain, Italy, Chile, Sweden, the US, Mexico, and France? These countries, the top ten in COVID-19 mortality (as of August 24, 2020, according to Johns Hopkins), all injected more than 49% of their elderly populations with the flu vaccine. This stands in stark contrast to the countries on the low end, with fatality rates/popuation up to four orders of magnitude smaller: Rwanda, Thailand, Mozambique, Sri Lanka, Papau New Guinea, Uganda, Tanzania, Taiwan, and Vietnam – with the exception of a 49% vaccination rate in Taiwan, the flu vaccination rates in these countries is extremely low. While one might object that these countries may lack in testing ability, careful serological study of multiple countries in Africa has shown that while in fact many cases were missed, this is because the residents were in fact not very ill – while the number of individuals with COVID antibodies in Kenya, for example, was similar to Spain, the hospitals were never overwhelmed and excess deaths were not reported. However we look at the data – either between or within continents – higher rates of flu vaccination clearly appears to transform large numbers of COVID cases from mild to severe disease. As flu vaccines are being pushed aggressively and even mandated in fall 2020, it is critical for citizens and medical professionals to review the issue.
https://www.homevaccineeducationnetwork.com/flu-vaccine-and-covid-19?fbclid=IwAR0_J-Tk-Y0ICTKLUNAnuEGLri4C5nYnk2xdSQa-1CWTAe57E1FIwaS7fTI
Cepiva za gripo že zmanjkalo, naslednja pošiljka prihaja sredi novembra
Ljubljana, 27.10.2020
Na Nacionalnem inštitutu za javno zdravje (NIJZ) so potrdili informacijo, da je dober teden po začetku cepljenja zmanjkalo cepiva za gripo. "Razdelili smo 250.000 odmerkov, naslednjo pošiljko pričakujemo v sredini novembra (20.000 odmerkov)," so zapisali.
S sprejemanjem naročil za letošnjo sezono so prekinili in o tem tudi obvestili izvajalce cepljenja. Prav tako so izvajalce cepljenja obvestili, da naslednjo pošiljko cepiva prejmejo šele v novembru in da njihova naročila tudi tedaj ne bodo v celoti realizirana.
"Vsi proizvajalci cepiv, ki imajo dovoljenje za promet, so nam sporočili, da v letošnji sezoni ni več možna dodatna dobava cepiva. Povpraševanja sicer redno ponavljamo, so pa možnosti, da dobimo dodatne odmerke, izredno majhne," še priznavajo na NIJZ.
Napovedali so tudi, da bodo prevzeli cepivo od drugih držav, če ga bo katera odstopila. So pa tudi na NIJZ od drugih držav že prejeli prošnje za odstop cepiva. Po preliminarnih podatkih se je v prejšnji sezoni (2019) v Sloveniji proti gripi cepilo 142.842 ljudi, od tega 51.030 kroničnih bolnikov, 716 nosečnic in 7595 zdravstvenih delavcev.
*
Lani se je cepilo proti gripi 142.000 , letos pa 250.000. ker cepivo za gripo poveča smrtnost zaradi COVID-19, imamo v novembru presežno smrtnost
Umrli 5.10-7.12. 2020
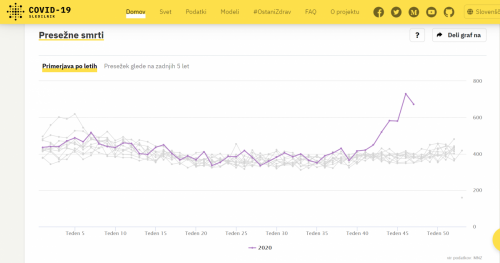
Presežne smrti nov 2020
Doktorat iz Avstralije o škodljivosti cepljenja- 400 strani : https://ro.uow.edu.au/cgi/viewcontent.cgi?article=5550&context=theses.
*
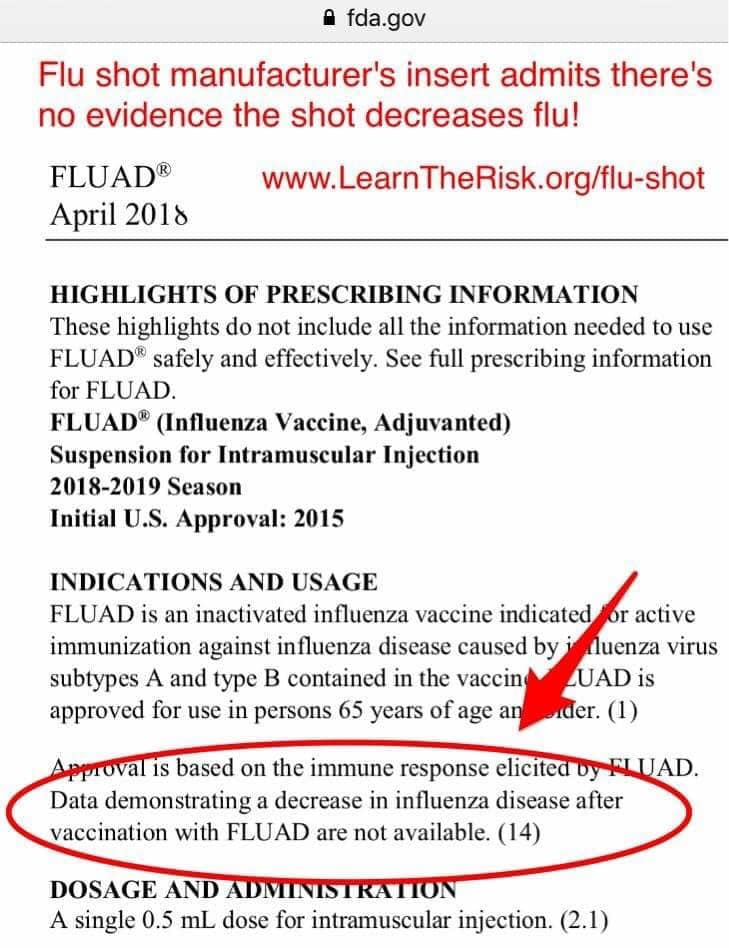
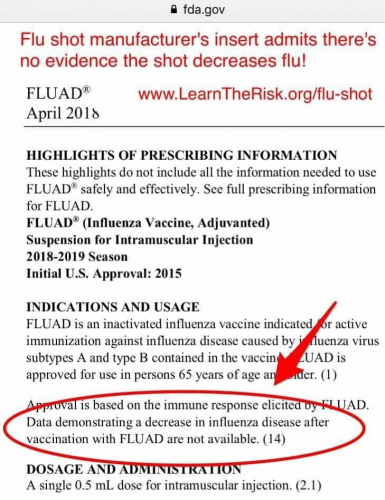
FLU SHOT LABEL ADMITS: NO DATA THAT THE SHOT DECREASES FLU
At least one flu shot maker admits that there is no evidence that getting a flu shot decreases your risk of getting the flu.
But the list of side effects from the toxic fu shot is long.
In fact, at the US Vaccine Court, the flu shot is considered the most DANGEROUS shot in terms of serious side effects and medical expenses payout.

Is Europe’s flu vaccine campaign linked to ‘second wave’ of COVID attributed deaths?
Analysis
January 4, 2021 (LifeSiteNews) – Is there a link between the flu shot and excess mortality in Europe in the second half of November? A simple comparison of vaccination statistics and the number of deaths attributed to COVID-19 reveals what looks like a correlation between the two, according to a contributor to the French daily FranceSoir. His lengthy and carefully documented op-ed is unsigned, but he claims to have a scientific background and his statistical quotes come from verified scientific papers and studies. And he believes that the correlation he observed is significant enough for the authorities to act upon his hypothesis and to take precautions because of the risk that the effects of the SARS-COV-2 virus are being potentiated by the influenza vaccine.
Here below is a shortened presentation of his reasoning. Links to quoted studies are available in his op-ed.
When the flu shot arrived in France on October 13, 2020, with health authorities encouraging the population to take it in the context of the COVID-19 crisis, in particular so as to prevent hospital congestion, there was an unprecedented rush that led to the vaccination of 34.2 percent of elderly or fragile subjects by the end of the month, compared with just 19.0 percent by October 31, 2019. This despite the fact that at the time there was no official sign of the presence of a flu epidemic. To date, only a handful of flu infections have been identified in France, several of which were related to patients who had just returned from abroad.
5.3 million doses of the vaccine were sold within eight days, and there was a historic shortage of stock: ordinarily, some 10 million doses are sold each year, and administered over a period of two months.
There was a subsequent peak in deaths attributed to the Wuhan virus between November 15 and November 30, in what the government called a “second wave” (according Professor Didier Raoult, the world-famous French microbiologist specializing in infectious diseases, it would be more precise to call it a “new epidemic” because of significant mutations of the virus). At the beginning of October, recalled the op-ed’s author, the reproduction rate of the epidemic was equal to 1, which should have prevented a new “epidemic surge.” However, a sudden rise of hospital admissions and later, deaths took place starting on October 20, one week exactly after the start of the flu vaccination campaign.
The preliminary reason why the author of the op-ed believed a correlation may exist between the flu shot and COVID-19 is that contracting different respiratory infections at the same time is not very likely. Preventing flu (and other rhinoviruses) would therefore facilitate a SARS-COV-2 infection.
In Italy, the Northern regions where flu and meningitis vaccines had been widely distributed during the fall and winter of 2019-2020 were those that saw the highest number of COVID-19 deaths in March and April of last year, as lung specialist Alberto Rossi observed in an interview with LifeSiteNews: almost all of the COVID-19 patients he personally treated in Piacenza had received the flu shot.
Back to France and the autumn statistics: by November 11, 9 million Frenchmen had been vaccinated against the flu. Nine days later, a second shortage of the flu shot occurred. Daily COVID-19 deaths started rising on October 20, and spiked starting on November 10, with daily highs beyond 1,000, while average deaths significantly declined as of December 1st.
Interestingly, a similar scenario played out in the Czech Republic, Poland, Slovenia, Hungary and Romania, that registered few COVID-19 deaths last spring. These Eastern European countries consistently had a very low influenza vaccine coverage until this fall, when aggressive campaigns led to an unprecedented number of flu shots.
In all these countries, there was a massive demand for the flu shot, leading to stock shortages similar to those in France, and in each of them slowly rising numbers of COVID-19 deaths suddenly spiked shortly after the campaign started, and are now descending once more.
Is this a mere coincidence? In Romania, where few COVID-19 deaths were registered last spring and where flu vaccination was rare, the exceptional flu shot campaign started mid-September and COVID-19 deaths started rising significantly as of October 7.
Most of these deaths are those of elderly or fragile patients.
The hypothesis is therefore: “The higher the vaccination rate for people over 65 years of age, the greater the mortality due to Covid-19.”
To answer this question fully, it would be necessary to evaluate the interaction between flu shots and SARS-COV-2 infections. In a context where side-effects of vaccines receive relatively little attention, notably because vaccine producers are not held responsible for them, these studies are few and far between and have not been made as a prerequisite for massive vaccination in the context of the coronavirus pandemic. There have been several warnings, however, on the grounds of several former whistle-blowing studies by medical specialists such as Michel Georget and Michel de Lorgeril, the latter having shown that people who had received the flu shot in 2008-2009 had a higher risk (40 to 250 percent higher) of contracting the pandemic A/ H1N1 than non-vaccinated patients.
The few existing studies in 2020 tend to go in the same direction.
“The first one is Spanish13 and was published on June 18 by Dr. Juan F. Gastón Añaños of the Pharmacy Service of the Spanish Hospital of Barbastro, in his own name. It concerns a town of 115,000 inhabitants, of which about 25,000 are over 65 years old. 20 people died. Of these 20 people, 90 percent were vaccinated against the flu during the winter, while only 63 percent of those over 65 were vaccinated. The small number of people who died can make interpretation hazardous. However, the study is continuing on a home for dependent elderly people: of 94 people, 25 there died from Covid-19. In this home, 80 residents were vaccinated against influenza and 14 were not. Of the 25 deaths, 24 were vaccinated; only 1 was not,” observes the author of the France-Soirop-ed.
Another statistical study, dated May 8, 2020, by two teachers of psychology and chemistry showed a correlation between flu-shot coverage and COVID-19 mortality last spring.
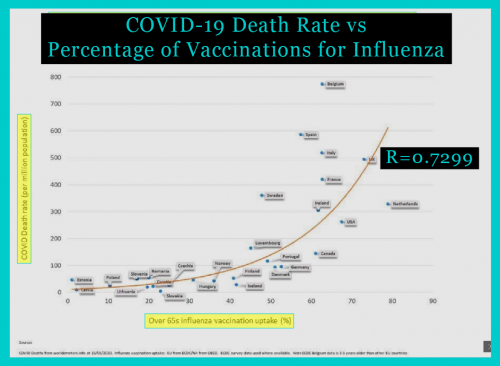
PEER journal published a wide-ranging study on October 1st analyzing data from 39 countries: “The results showed a strong correlation between Covid-19 deaths and the rate of influenza vaccination in people 65 years and older (R=0.687; P-value = 0.00015).”
The author of the op-ed added personal evaluation of statistics from European countries, excluding those that had closed down their borders early such as Iceland, or that made extensive use of the “Raoult protocol” as it is known in France: hydroxychloroquine, azithromycin and zinc. He also found that the higher the vaccination coverage in one of the 21 European countries he retained for his calculations, the higher the mortality in relation to the total population or to the number of people falling ill with COVID-19.
Counter-studies contradicting these studies do exist, and the author quoted them, but showed that they had little statistical significance for various reasons; he also rejected studies favorable to his hypothesis for the same type of reason.
He quoted a further study that was presented as proving that there is no relation between flu vaccination and COVID-19 hospitalizations or deaths, while in fact the study shows that 17 percent of non-vaccinated infected patients needed hospital care, against 41 percent of patients who had received the flu shot. The authors of this study used “corrections” without giving details. In a general way, according to the France-Soirop-ed, studies that contradict the flu shot link suffer “weaknesses” and are indeed “cautious” as to their results.
The op-ed added that there can be other factors explaining the sudden surge in COVID-19, such as the fact that countries that have not been affected by a respiratory virus often observe a surge in infections later on (but usually, the virus is weaker by then).
“What is troubling is that all European countries that have been spared so far are being impacted by an outbreak at the same time. An epidemic does not spread uniformly in time and space. Unless there is a common trigger in time and space. The European Union conducted a campaign in early October to encourage all European countries to implement influenza vaccination campaigns. It seems legitimate to ask the question of the impact of influenza vaccination on mortality in case of infections with other respiratory viruses,” it said.
There is also the “climate factor,” linked to less sun, colder weather and lower immunity of the population. But on the other hand, it recalled that last spring, Europe had exceptionally warm and sunny weather. Also, temperatures fall earlier in Eastern Europe than in the west, but its COVID-19 mortality did not rise earlier in consequence.
As to how the vaccine can favor COVID-19, the op-ed quoted several studies published in 2020 in The Lancet, Science Direct and the Journal of Medical Virology suggesting that viral infections such as the rhinovirus and coronaviruses can stop flu epidemics by activating the immune system against future flu viruses.
This “viral interference” can affect a current epidemic, these studies suggested. Other pathogens, including common rhinoviruses, could in this way “suppress” the replication of SARS-COV-2 whose growth factor is lower than theirs.
Quoting Georget and de Lorgeril, the author wrote: “We are wrong to believe that vaccines ‘magically’ stimulate our immune system with an attenuated or dead virus without any collateral effects. Why shouldn't the exact opposite happen? The presence of the dead or attenuated virus can be interpreted as benign by our immune system and thus facilitate a future infection. This is called an immune response that facilitates the infection. This phenomenon has been observed for several viruses such as measles, respiratory viruses (RSV), dengue fever, but also HIV. It is also known that vaccination in some cases leads to a drop in immune defenses contrary to what one might expect, and this drop can last several weeks.”
He also observed that “social distancing” and frequent hand-washing possibly blocked benign infections that actually activate our immune systems in winter, thus giving wider scope to more dangerous and contagious infections when contracted.
So the immune response to COVID-19 might block the flu, and at the same time the flu shot might “deprive people of a strong immune activation that could have protected them against SARS-COV-2.”
Virological surveillance in France showed how a rise in SARS-COV-2 infections corresponded to a decrease in common benign rhinoviruses, together with the absence of flu infections. In the same way benign rhinoviruses tend to disappear at the height of a flu epidemic and return after it ends.
Finally, side-effects of the flu shot may also make patients more vulnerable with regard to COVID-19, according to the author. These include bronchial damage, asthma and diabetes, and all these conditions are related to increased morbidity and mortality among COVID-19 patients.
*
Sep 30, 2020

