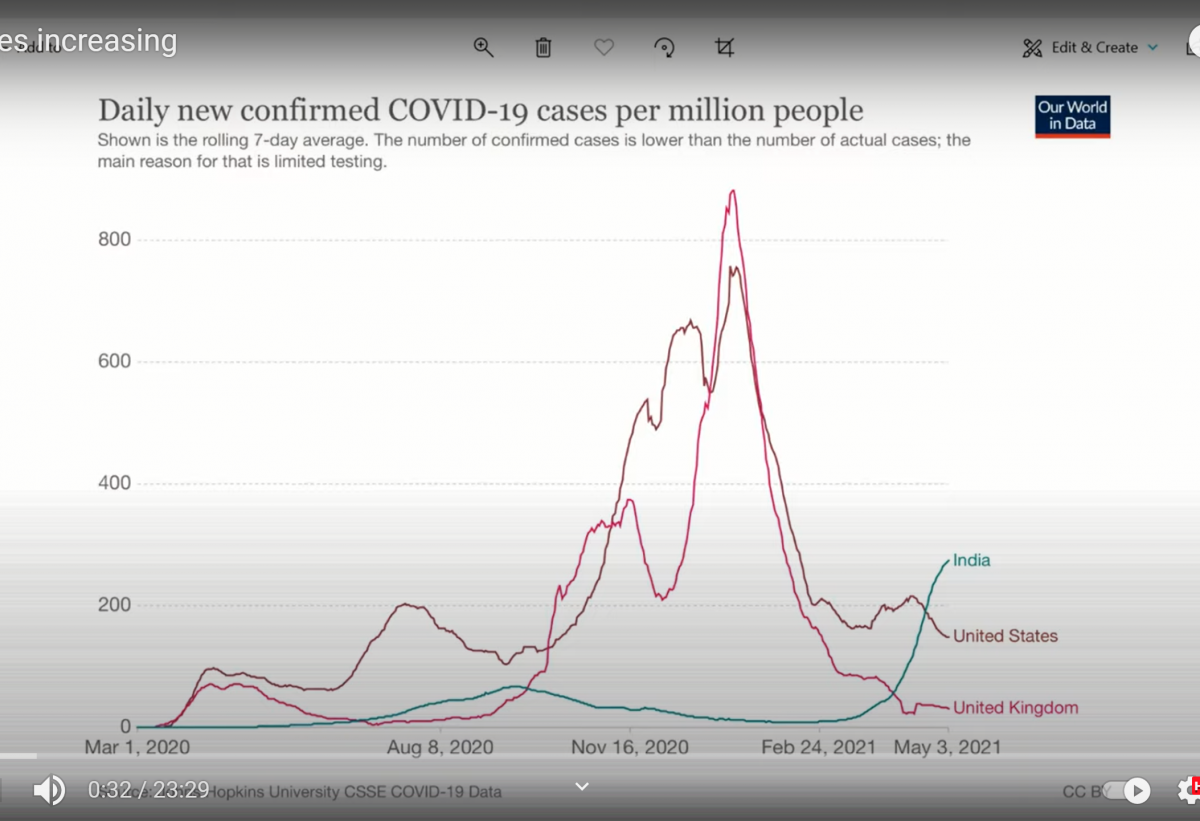
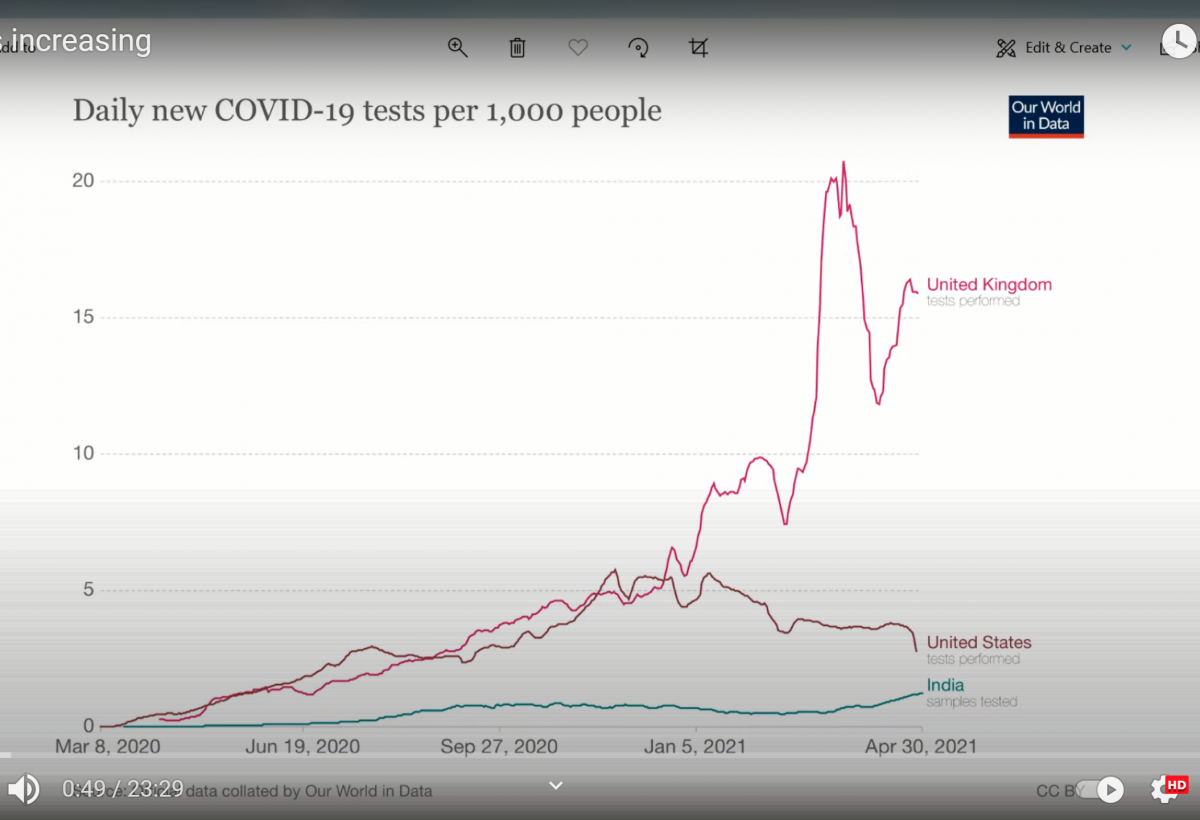



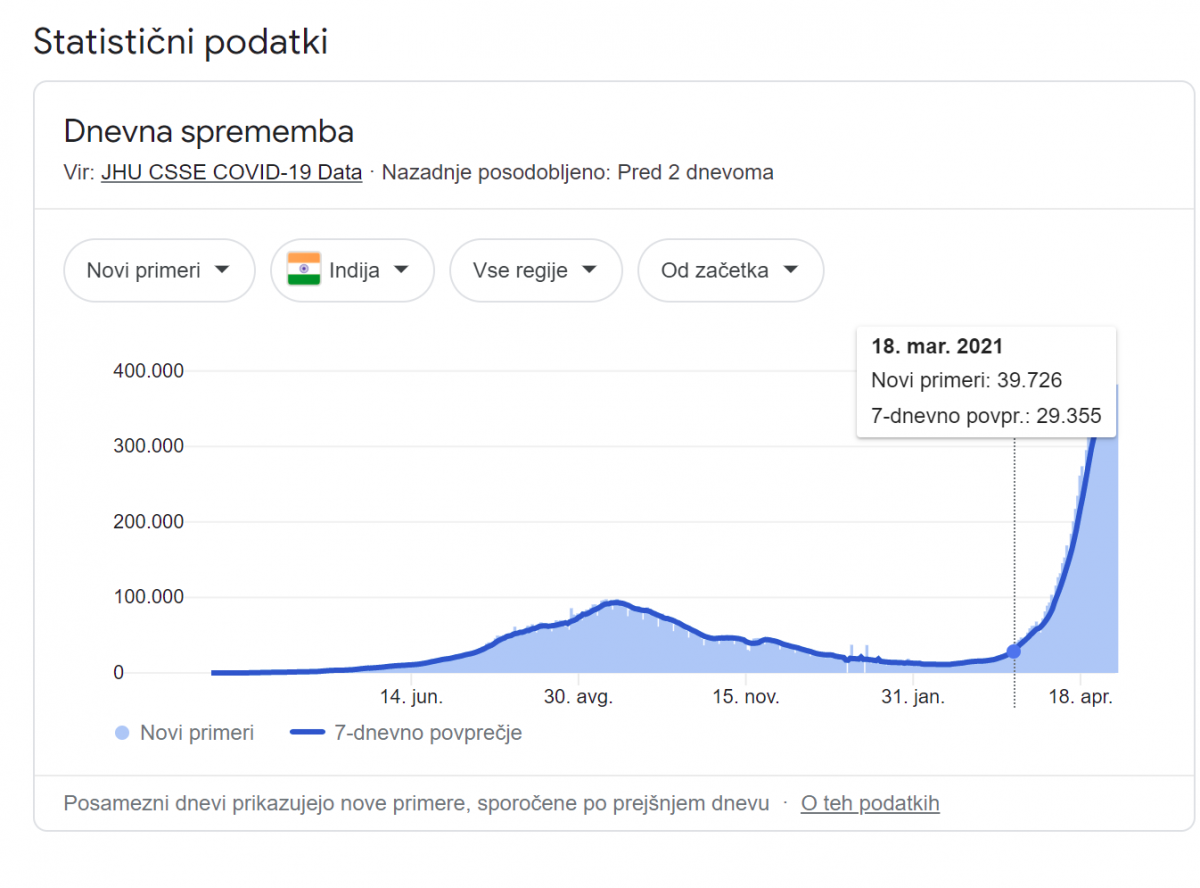

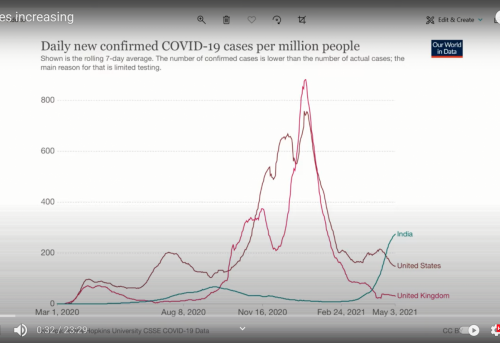
Število dnevnih primerov s pozitivnim PCR testom ( za katerega je znano, da ni diagnostično orodje in ne pokaže okužbe z aktivnim koronavirusom SARS CoV-2) v Indiji močno narašča od aprila 2021, a kljub temu je še veliko nižje od števila pozitivnih primerov v ZDA ali UK od novembra 2020 do februarja 2021.
*
*
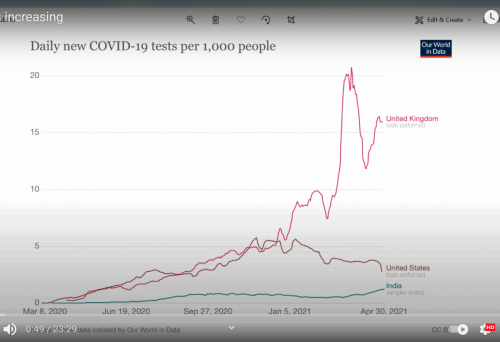
V Indiji se je aprila povečalo tudi število opravljenih PCR testov na 1000 ljudi, kar je vplivalo na večje število primerov pozitivnih PCR testov
*
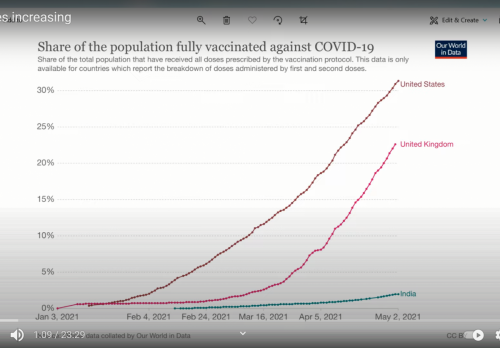
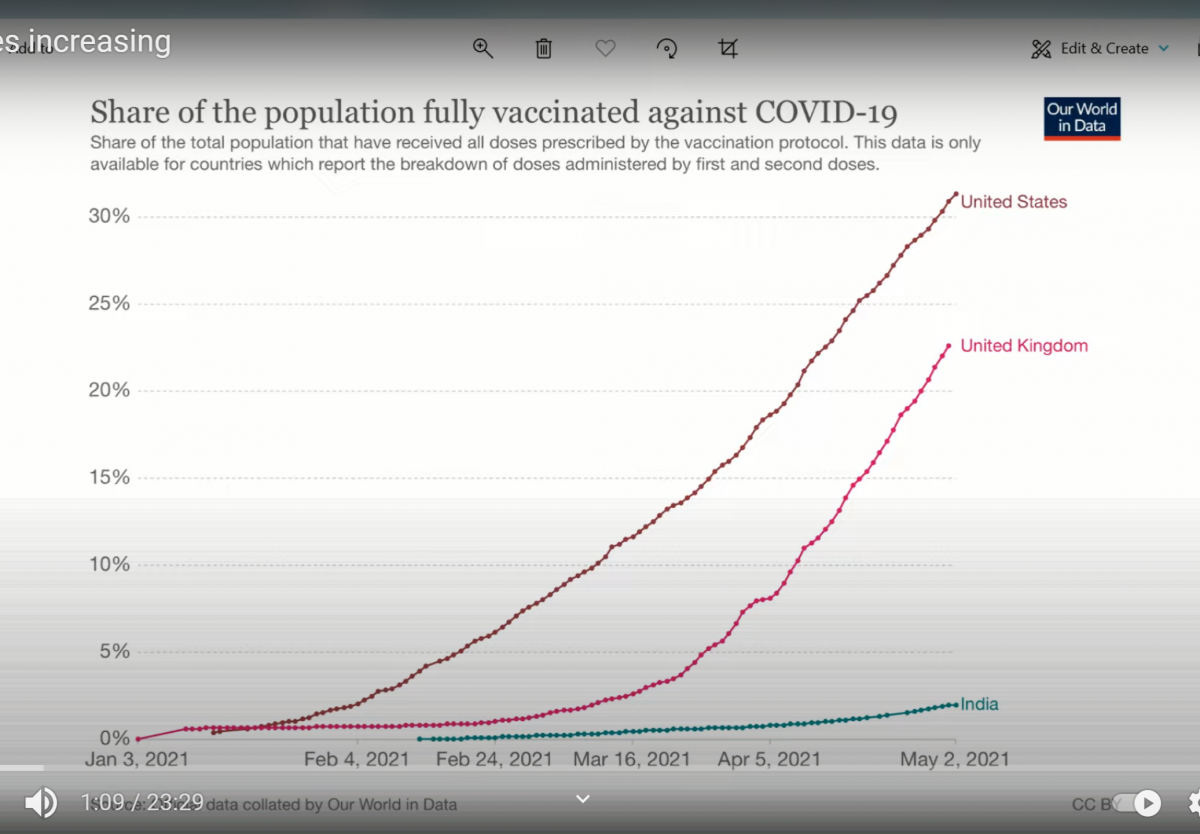
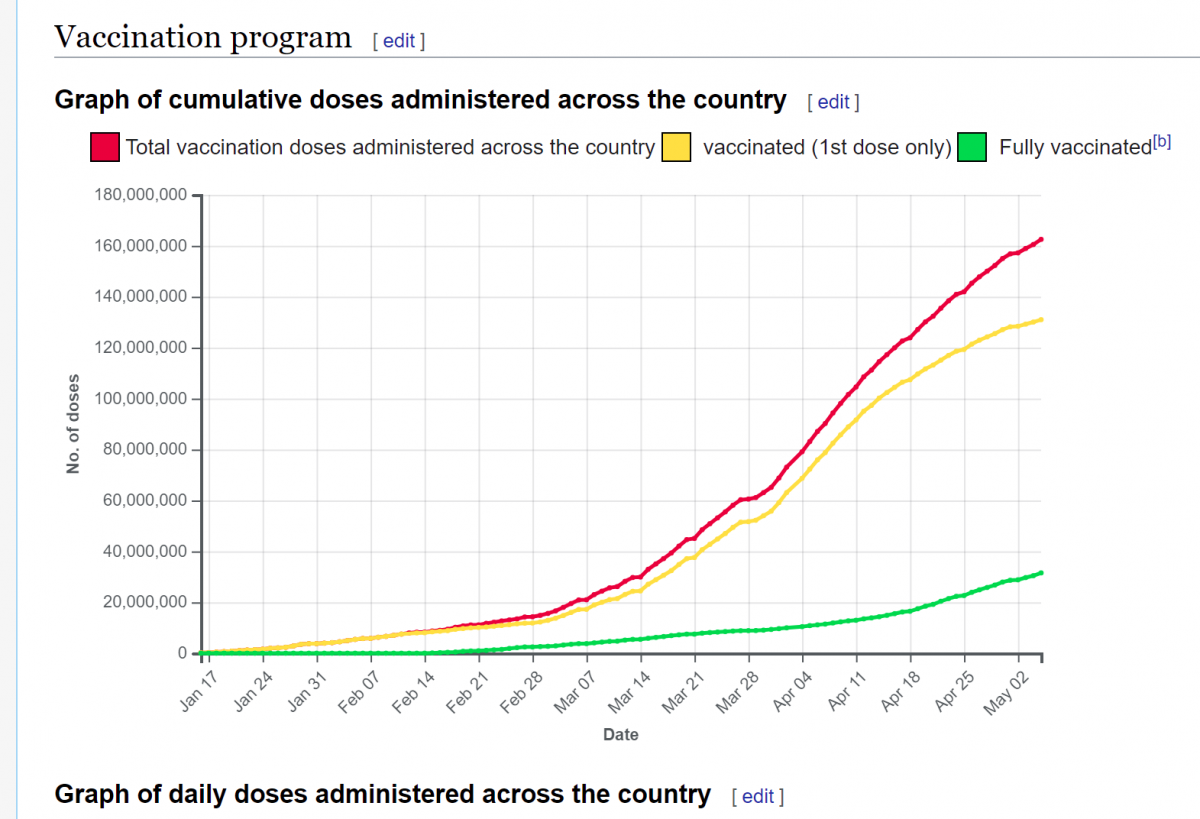
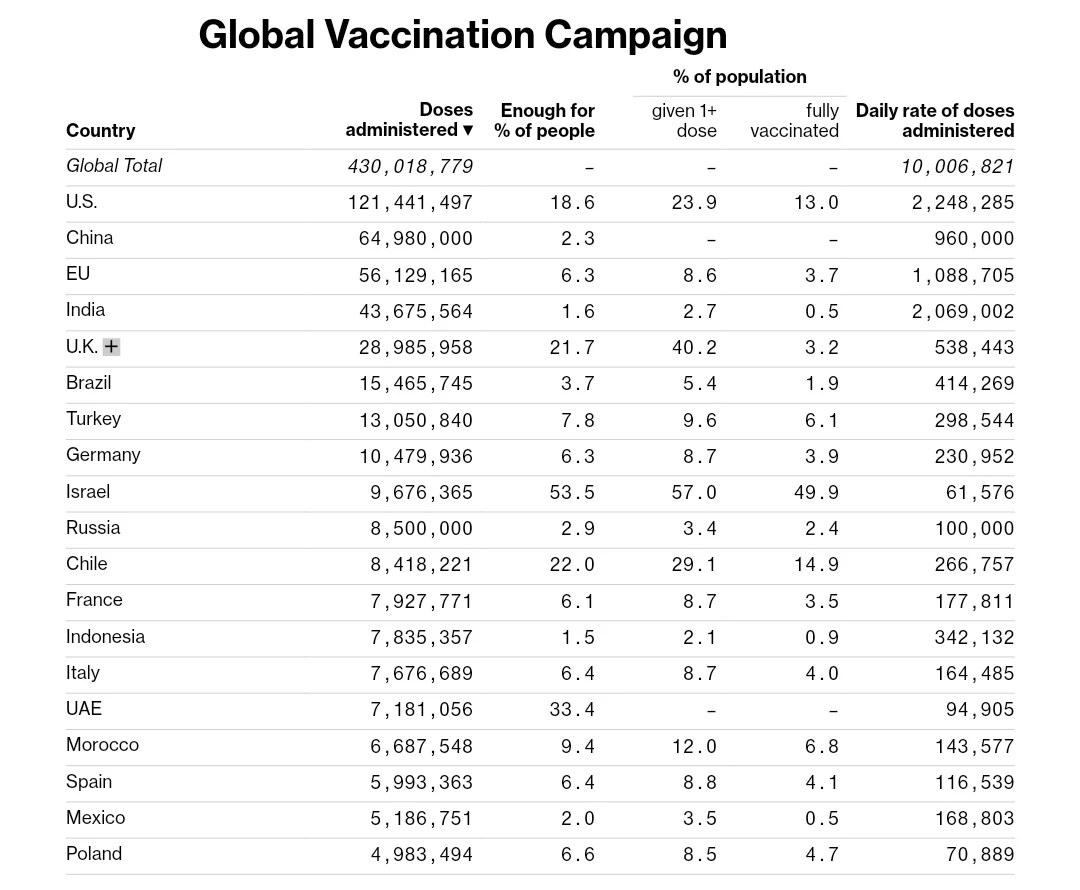
Delež v celoti cepljenega prebivalstva se je v Indiji povečal marca in aprila 2021
*
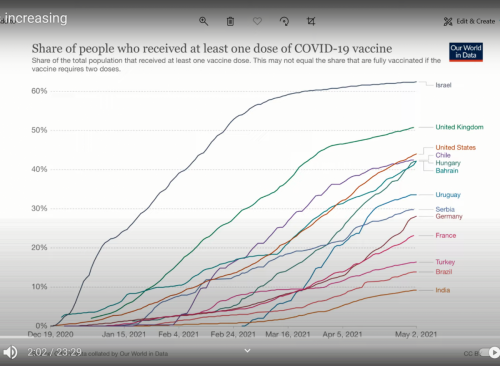
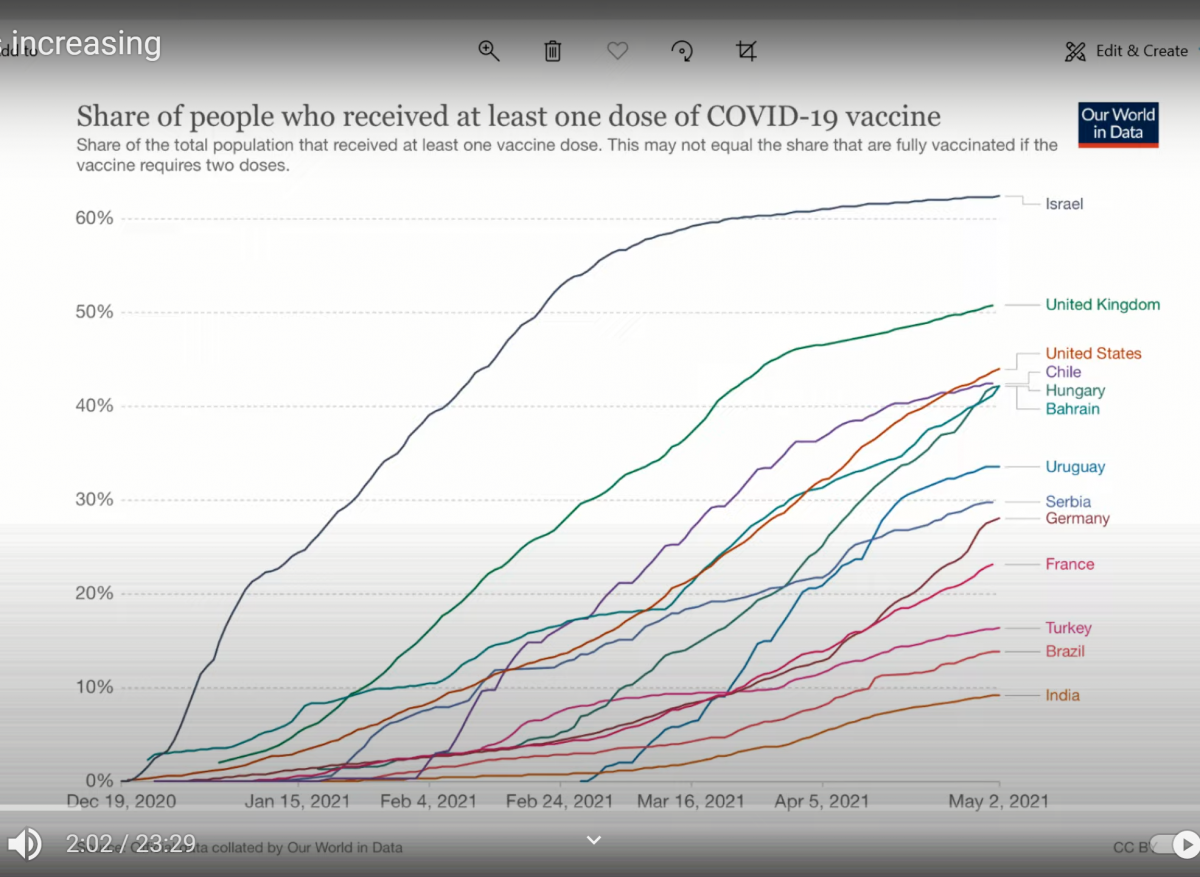
Delež cepeljnih z vsaj enim odmerkom se je v Indiji zelo povečal aprila 2021
Madžarska, Urugvaj in Čile uporabljajo rusko cepivo Sputnik
*
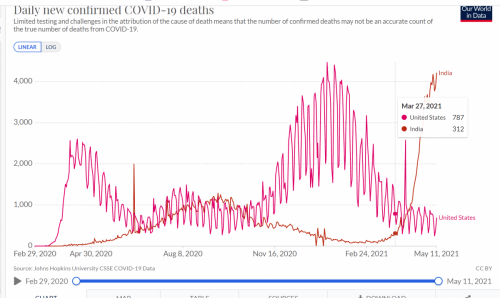
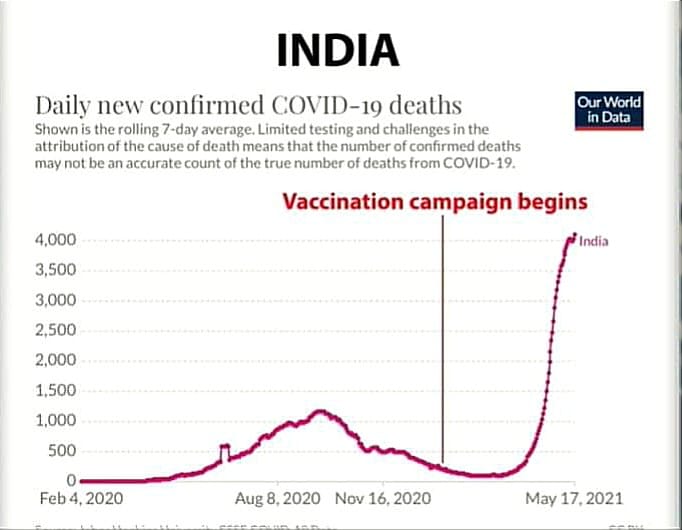
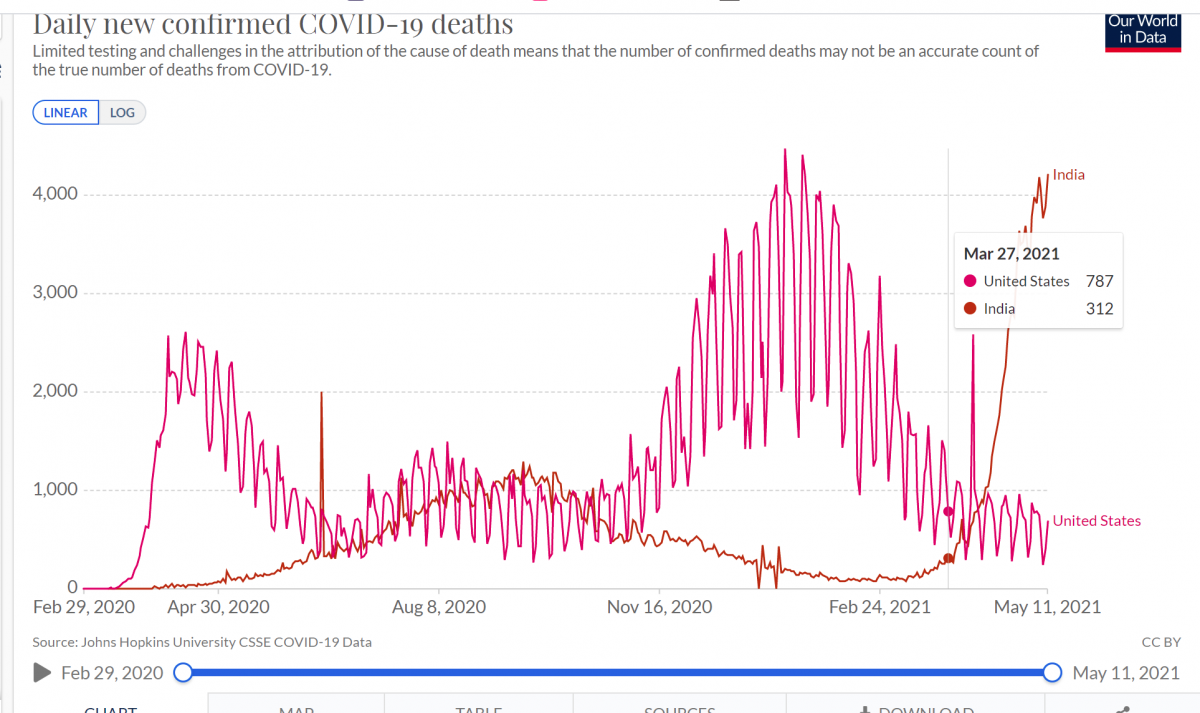
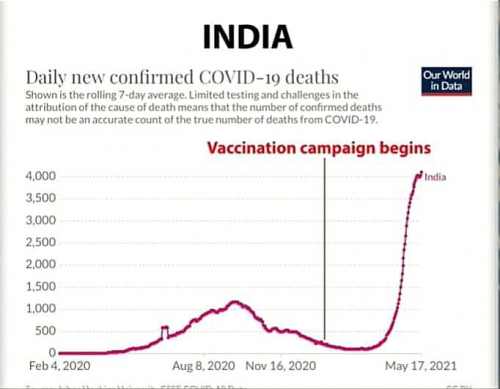
Indija je v začetku maja 2021 dosegla nivo dnevnih smrti, kot ga je imela ZDA v sredini januarja 2021- vendar je potrebno vedeti, da ima Indija 1,2 milijarde prebivalcev, ZDA pa skoraj 4 krat manj, to je 331 milijonov
*

*
*
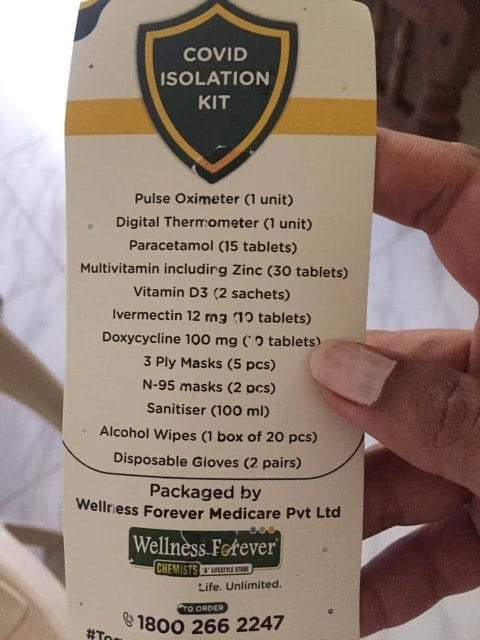
V Indiji je do konca aprila 2021 bilo uporabljenih 150 milijonov odmerkov cepiva, v celoti cepljenih je okoli 2% populacije, ki šteje približno 1.2 milijarde ljudi. Avstralija je prepovedala prihod svojih državljanov iz Indije, da bi prebivalstvo obvarovala pred "indijskim sevom" koronavirusa. V indijskih bolnišnicah ni prostora, kisika in zdravil, v mnogih vaških področjih ni bolnišnic. Zasebne bolnišnice zahtevajo depozit v višini približno 2.700 USD preden sprejmejo bolnika na zdravljenje. Zato veliko ljudi nima dostopa do zdravstvene nege. Veliko ljudi ima simptome, kot so kašelj, bolečina v križu, zasoplost, izguba okusa in vonja, vročina in šibkost.
Vir: https://www.youtube.com/watch?v=Jw6zqt-s2Ck
Po podatkih iz Indije, zboli od 0,02 do 0,04% cepljenjih ljudi (v ZDA 0,008%)
*
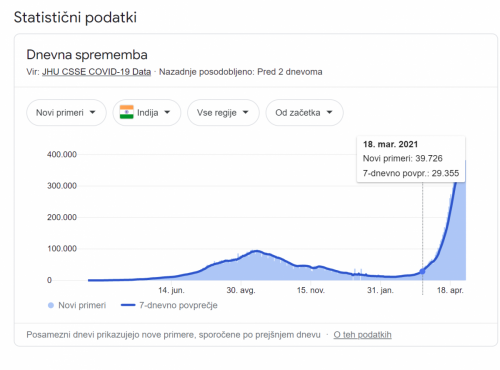
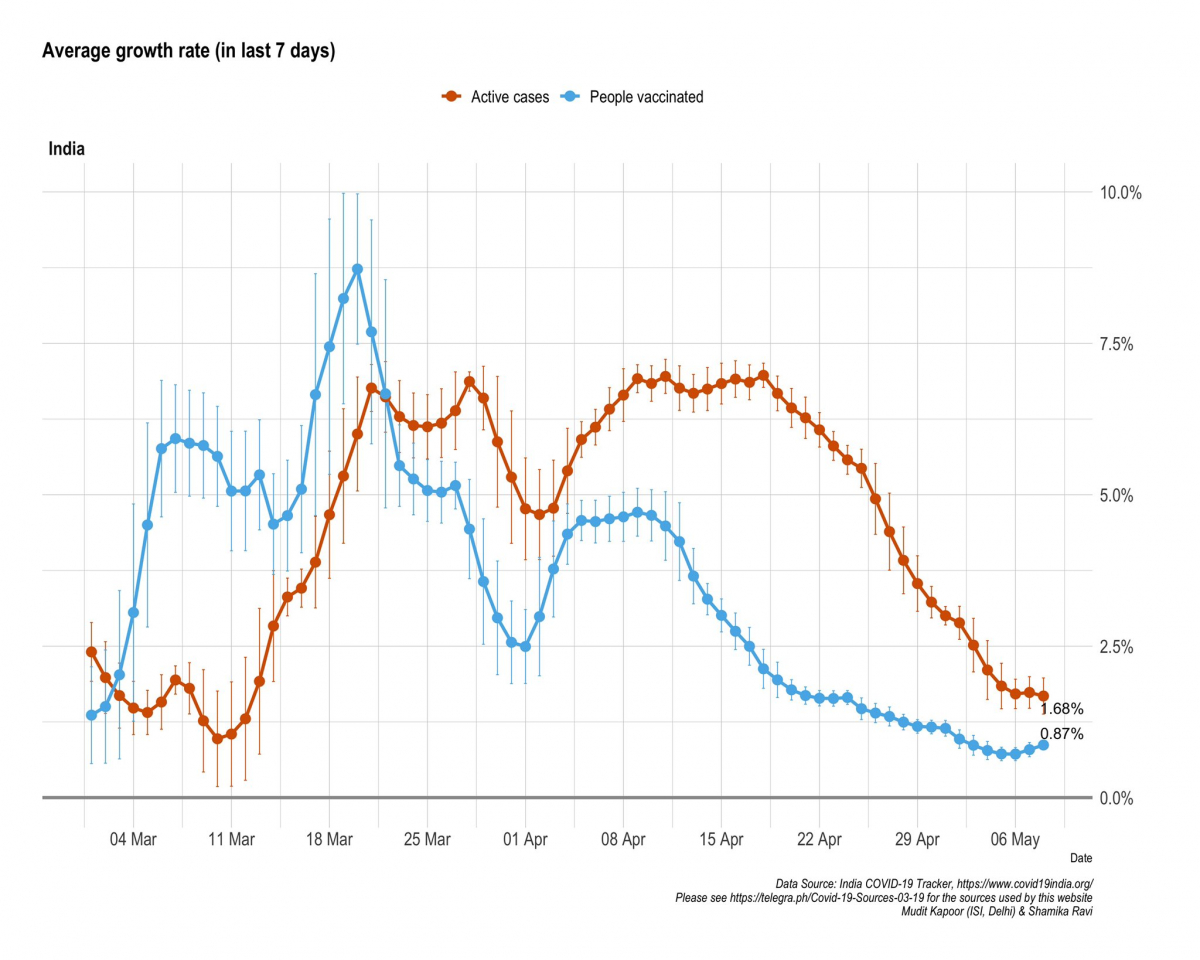
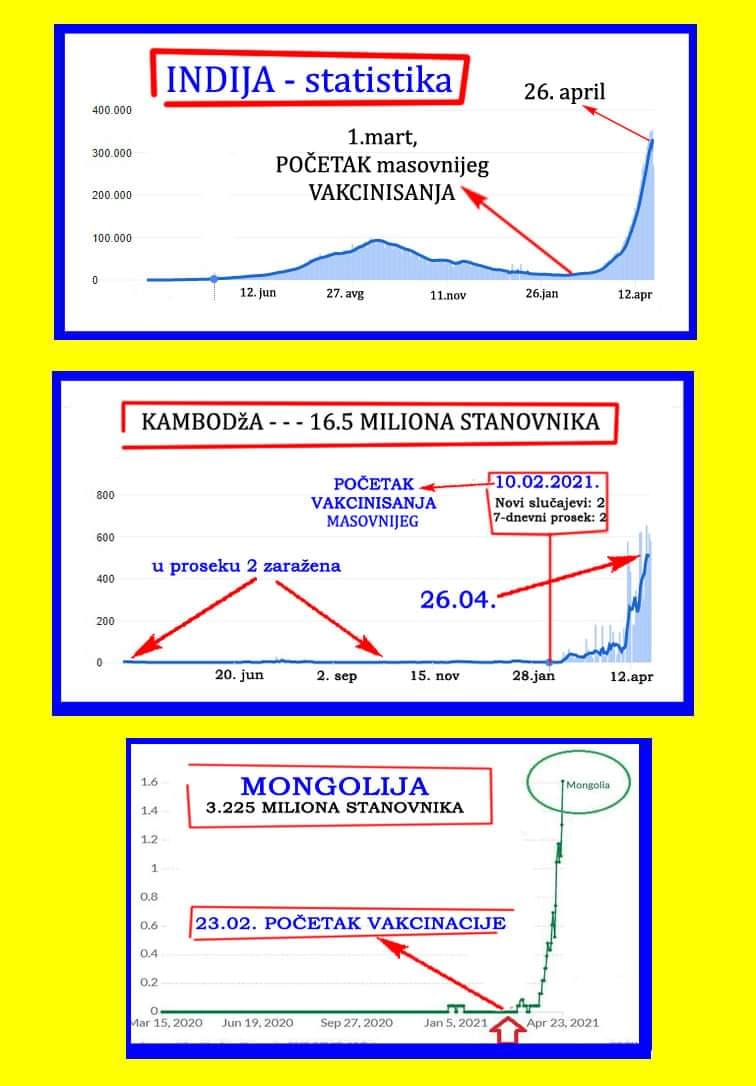
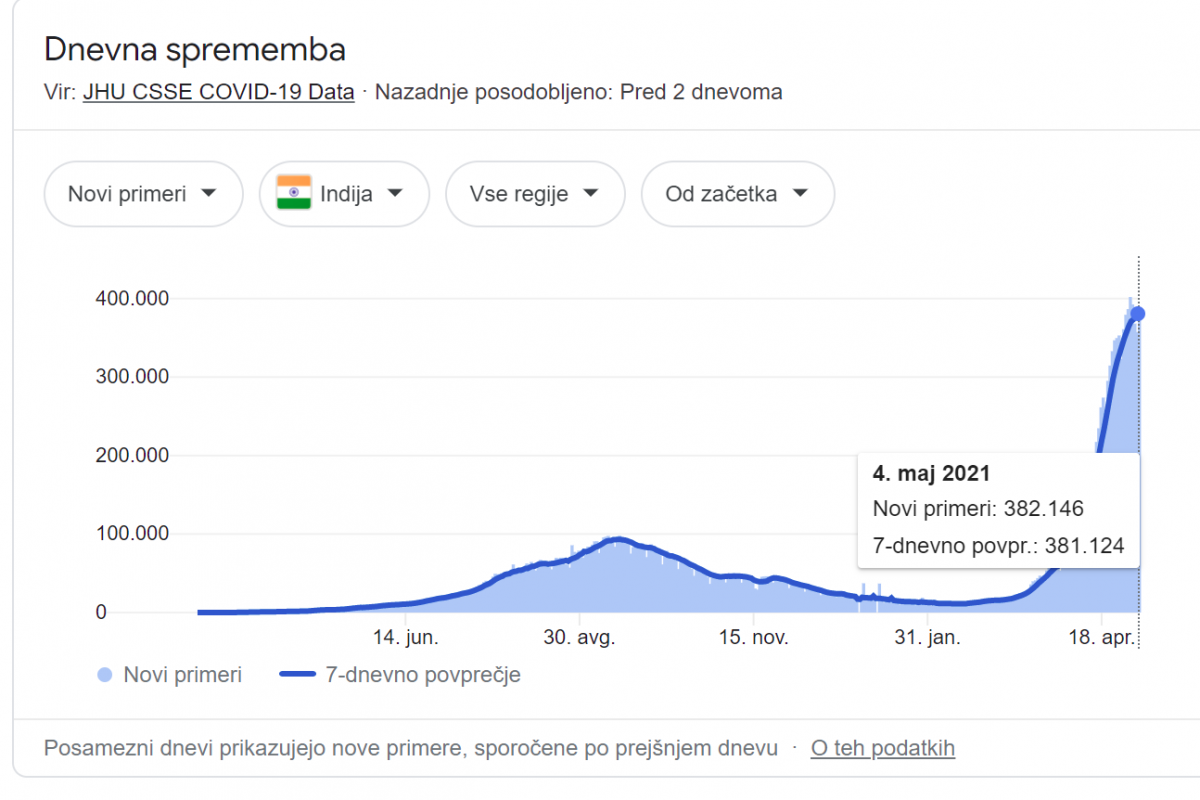
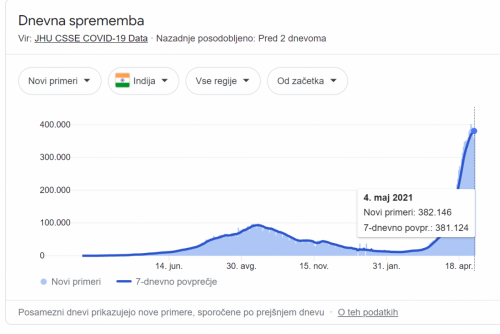
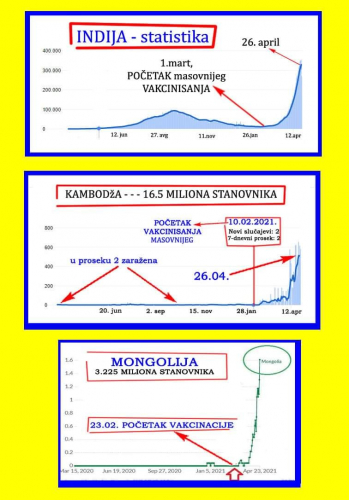
Število novih primerov pozitivnih PCR testov je pričelo strmo naraščati 18. marca 2021, kmalu po povečanju števila cepljenih. Tega dne je bilo 39.726 novih primerov, 4. maja 2021 pa je bilo skoraj desetkrat več novih primerov, to je 382.146
*
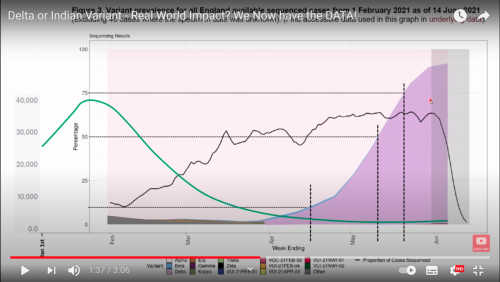
Povečanje okužb v Indiji pripisujejo dvojni mutaciji koronavirusa SARS CoV-2, ki naj bi bila bolj prenosljiva in bolj odporna na cepivo. Vlada pravi, da so analize iz države Maharashtra pokazale povečanje vzorcev dvojih mutacij E484Q in L452R, ki kažejo na imunski pobeg in povečano infektivnost. Najdene so bile v 20% primerov v tej državi. Dr. Jeremy Kamil, ameriški virilog iz Louisiana University Health Sciences Center Shreveport je povedal, da je mutacija E484Q podobna mutaciji E484K, ki se je pojavila v Južni Afriki (B.1.351) in v Braziliji (P.1). Mutacija L452R pa se je pojavila v liniji koronavirusa v ZDA, v t.i. Kalifornijskem sevu (B.1.427/B.1.429 linija).
V začetnem obdobju pandemije, so geni beljakovinske bodice imeli samo eno mutacijo, ki je zdaj dominantna vsepovsod. GISAID ima javno dostopno bazo podatkov, kjer je 43 sevov koronavirusa, ki imajo dve mutaciji, najdeni v Indiji. Angleški sev iz marca 2021 pa ima kar devet mutacij genov beljakovinske bodice.
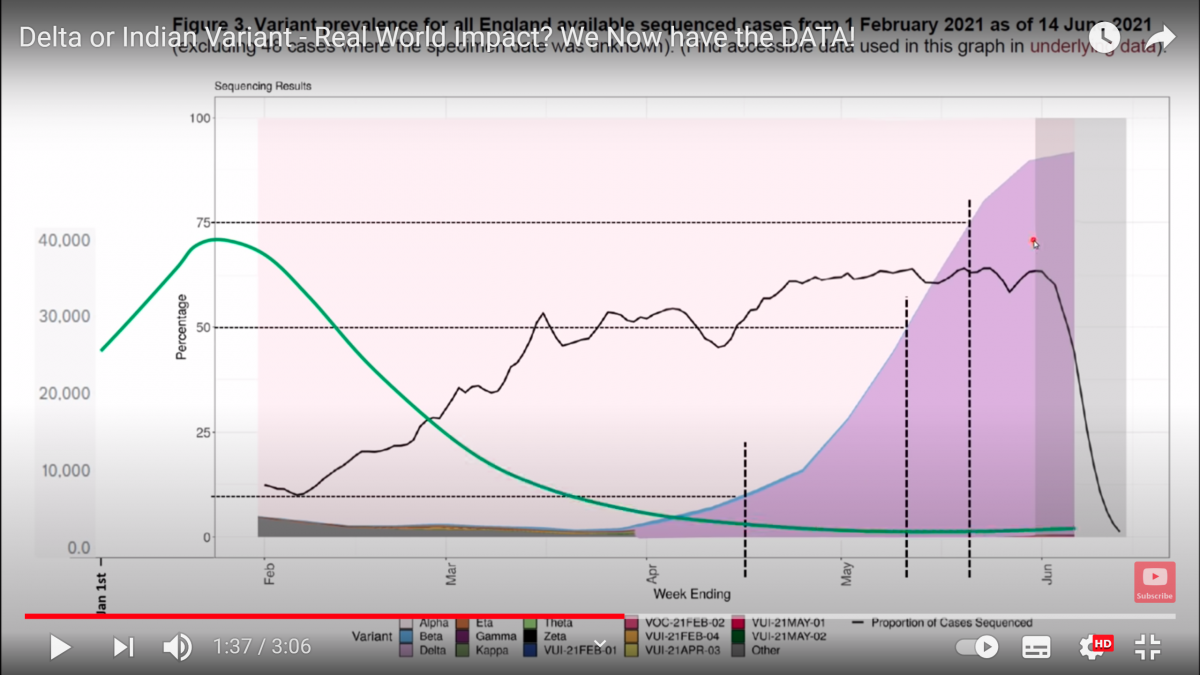
Indijski sev z dvema mutacijama pa ni bolj smrtonosen, kljub večji prenosljivosti. Indijski sev ni vzrok drugega vala okužb v Indiji, saj 80% sekvencioniranih vzorcev koronavirusa nima teh dveh mutacij, ki sta najdeni v samo 230 primerih v Maharashtra med tisoči sekvencioniranih vzorcih koronavirusa.
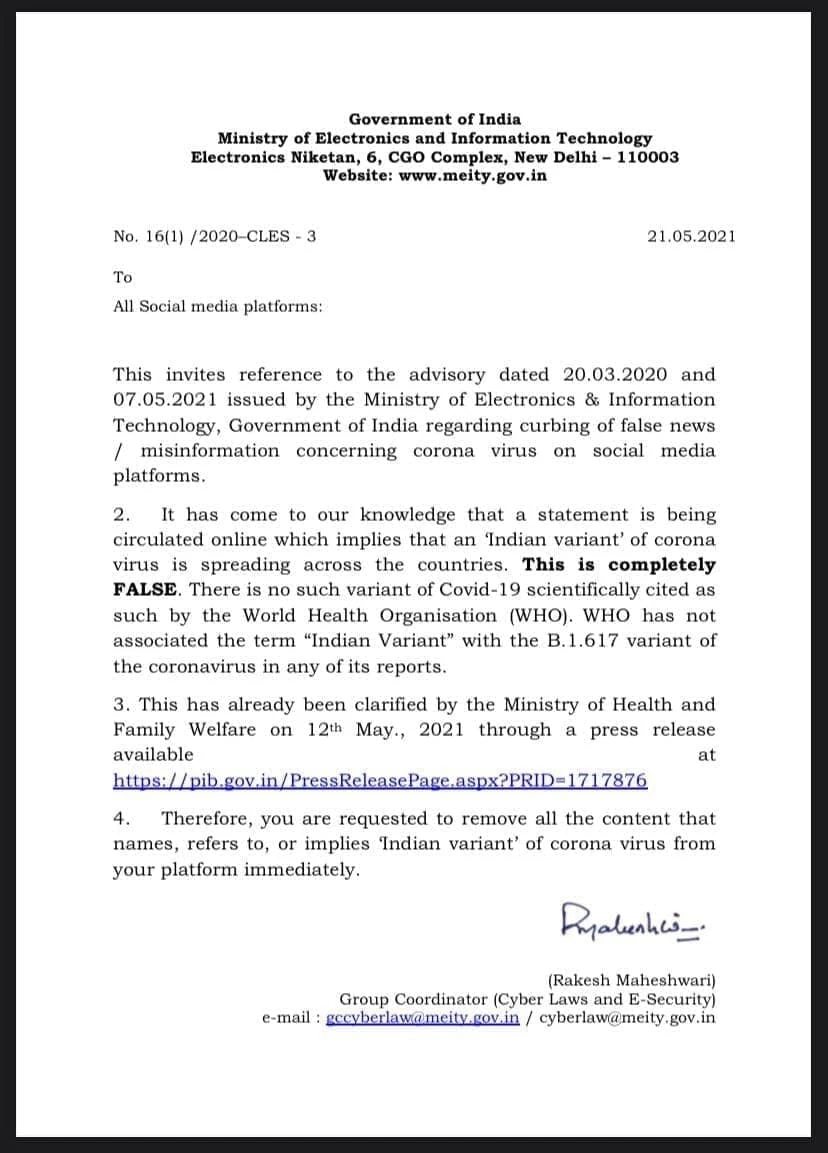
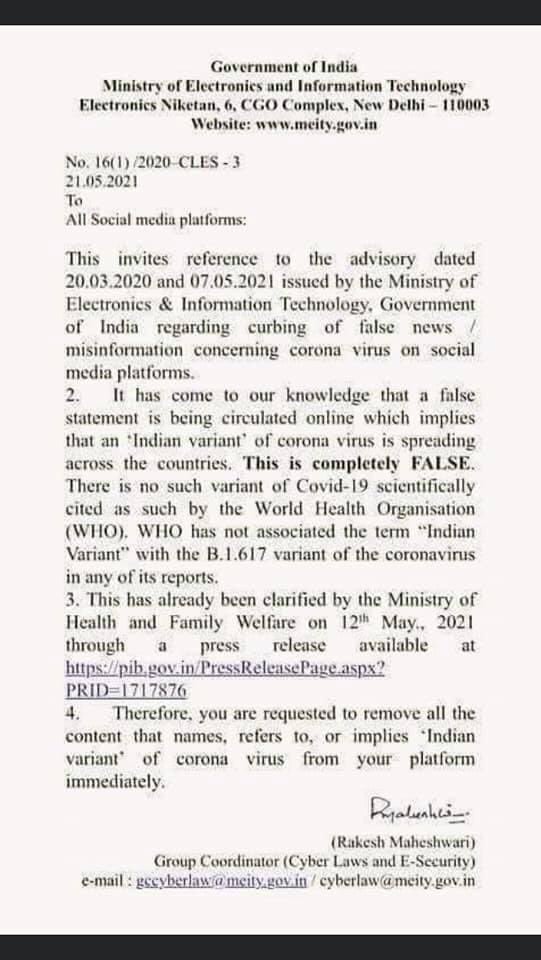
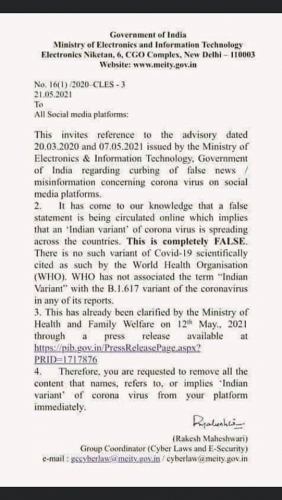
https://pib.gov.in/pressreleasepage.aspx?PRID=1717876&fbclid=IwAR16Ug59QuzyzoRh7-YG69Di-00BsYvEY1IP0sCqhOuXXFvc_O9eS8WWIm4 -WHO has not associated the term “Indian Variant” with B.1.617, now classified as Variant of Concern
Če indijski sev ni vzrok eksponentnega porasta pozitivnih primerov, kaj je potem vzrok?
*

*
Možen vzrok je cepivo za COVID-19, s katerim so v Indiji pričeli cepiti 16. januarja 2021, 18. marca pa se je pričela eksponentna rast primerov. Med 16. in 29. marcem 2021 je bilo po uradnih podatkih AEFI 91 smrtnih primerov zaradi COVID-19 cepiva. Cepivi, ki sta dobili odobritev za uporabo v sili sta Covishield od Oxford/Astra Zeneca capivo, ki ga proizvaja Serum Institute of India in Covaxin, ki ga je razvil Bharat Biotech. Kot tretje cepivo je odobren Sputnik V, s katerim naj bi začeli cepiti proti koncu maja 2021.
Kot možen vzrok eksponentne rasti primerov pozitivnih PCR testov sicer navajajo angleški sev (B.1.1.7), saj so ga našli v 736 vzorcih od skupno 10.787 vzorcev. Vendar pa je profesor Vincent Racaniello demantiral trditev, da je bil angleški sev bolj prenosljiv in smrtonosen. Več o tem je v članku:
Vir: https://www.bbc.com/news/world-asia-india-56517495
Da je bolj verjetno, da so COVID-19 cepiva vzrok drugega vala okužb v Indiji in ne indijski ali angleški sev, kažejo tudi podatki o posledicah cepljenja:
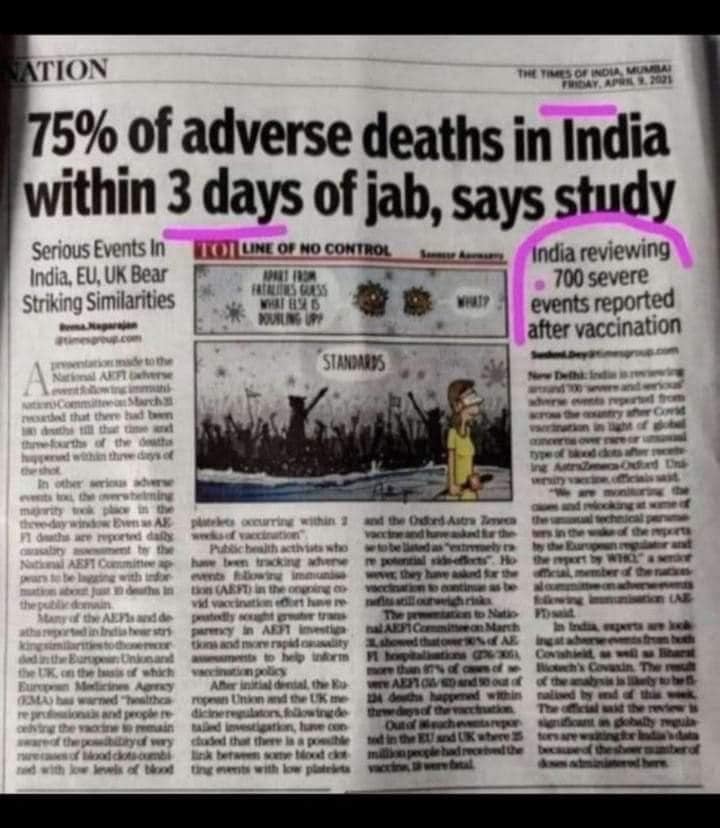
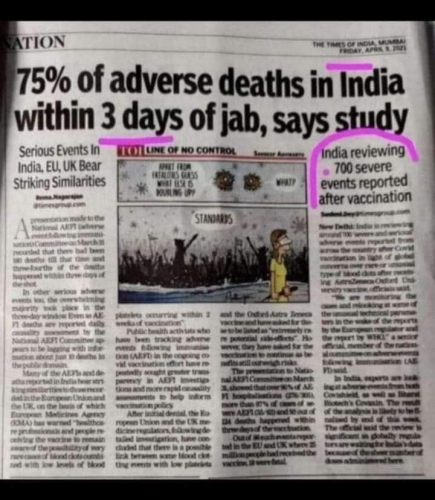
Do 31. marca 2021 je bilo 180 smrti in 305 hospitalizacij zaradi COVID-19 cepiv in 75% smrti in 90% hospitalizacij se je zgodilo v treh dneh po prejemu cepiva, poroča indijski komite za spremljanje posledic cepljenja AEFI. Večina smrti je posledica krvnih strdkov ali znižanja nivoja trombocitov 14 dni po prejemu zlasti cepiva Covishield proizvajalca Oxford/Astra Zeneca ozrioma licenčnega indijskega proizvajalca Serum Institute. To cepivo uporablja oslabljen adenovirus šimpanza, v katerega je vstavljena sekvenca koronavirusa za kodiranje beljakovinske bodice SARS CoV-2. Do 4. maja 2021 so razdelili okoli 140 milijonov odmerkov Covishield/Astra Zeneca cepiva in okoli 20 milijonov odmerkov Covaxina/Bharat Biotech
Zdaj pa so ugotovili, da krvne strdke in poškodbe ožilja povzročajo beljakovinske bodice, bodisi iz divjega koronavirusa SARS CoV-2 bodisi tiste, ki nastanejo zaradi COVID-19 cepiv. To pomeni, da imajo cepljeni povečano tveganje za krvožilne bolezni in smrt. Več o tem je v članku:
Več o posledicah cepiva Oxford/Astra Zeneca je v objavi:
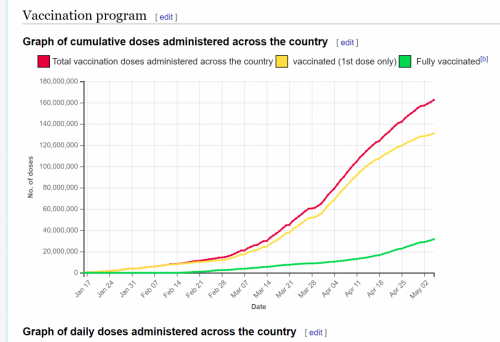
rumena =število prejemnikov 1. odmerka, zelena=število prejemnikov 2 odmerkov rdeča=število apliciranih odmerkov cepiva.
vir: https://en.wikipedia.org/wiki/COVID-19_vaccination_in_India
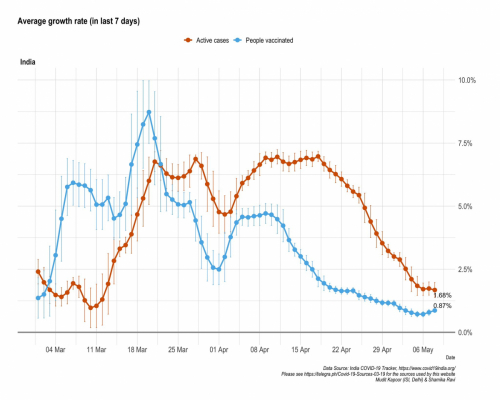
Eksponentna rast primerov pozitivnih PCR testov se je pričela po 11. marcu, kar je v korelaciji s povečanjem aplikacije odmerkov cepiva, ki se je začela eksponentno večati v začetku marca 2021.

Vir: https://www.google.com/search?q=covid+in+india&rlz=1C1GCEA_enSI871SI871&oq=covid+in+india&aqs=chrome..69i57j0j0i22i30l7.3415j0j15&sourceid=chrome&ie=UTF-8
*
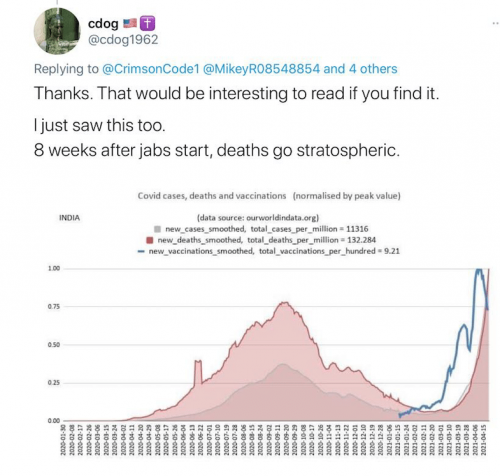
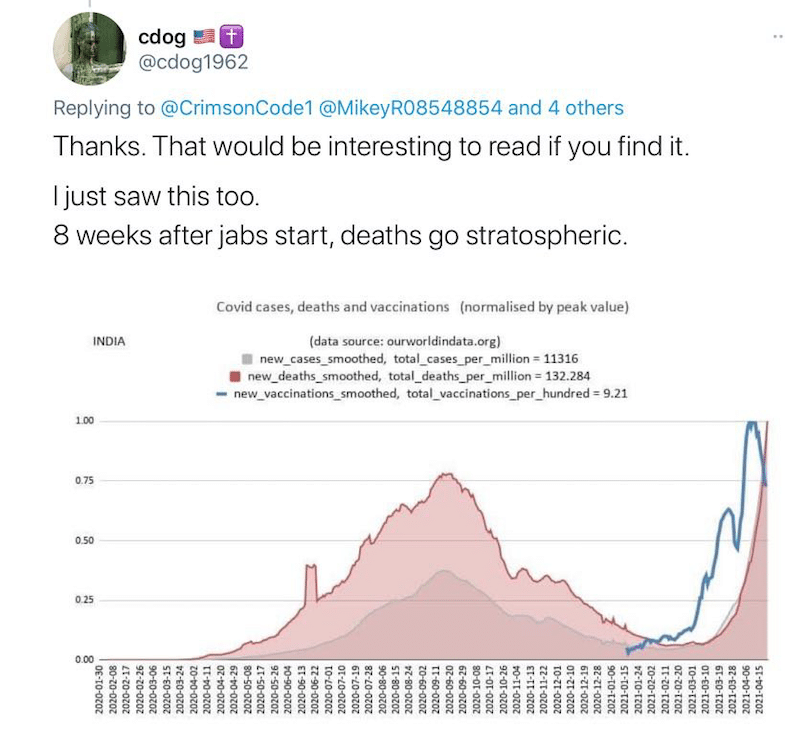
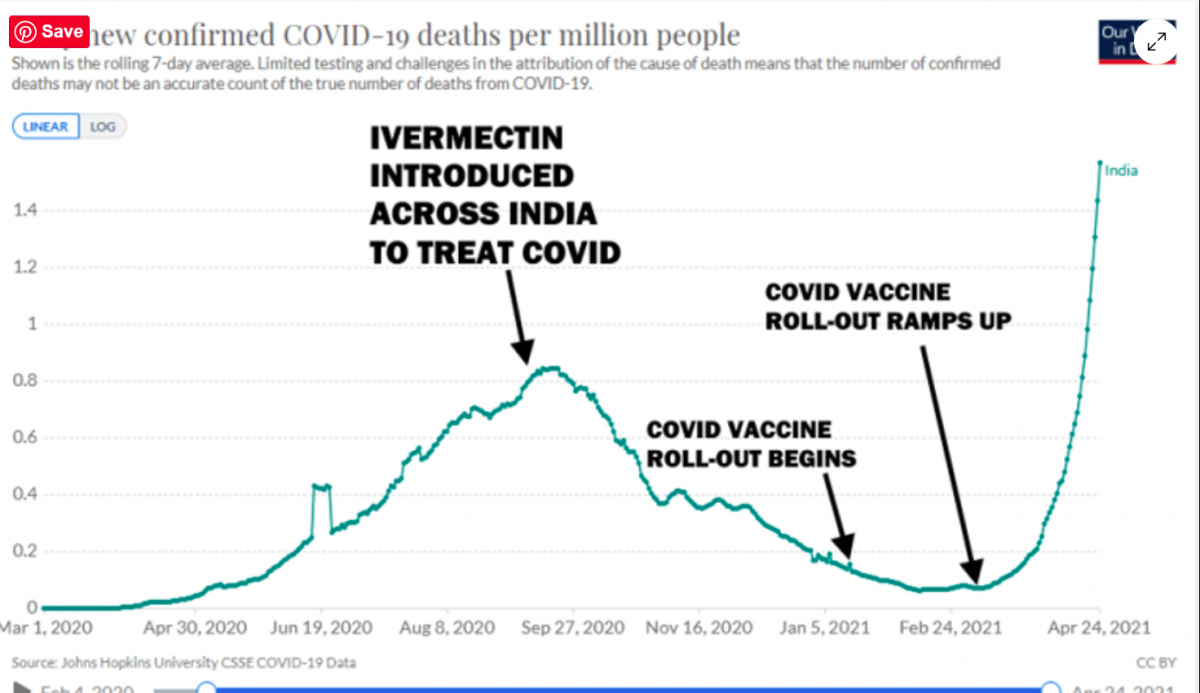
Na tej sliki vidimo korelacijo med povečanjem števila cepljenih ljudi (modro) in povečanim številom smrti (rdeča krivulja) in povečanjem primerov pozitivnih PCR testov (siva)
*
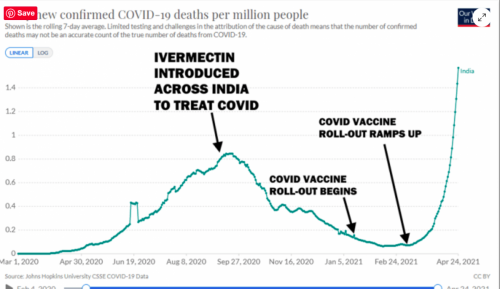
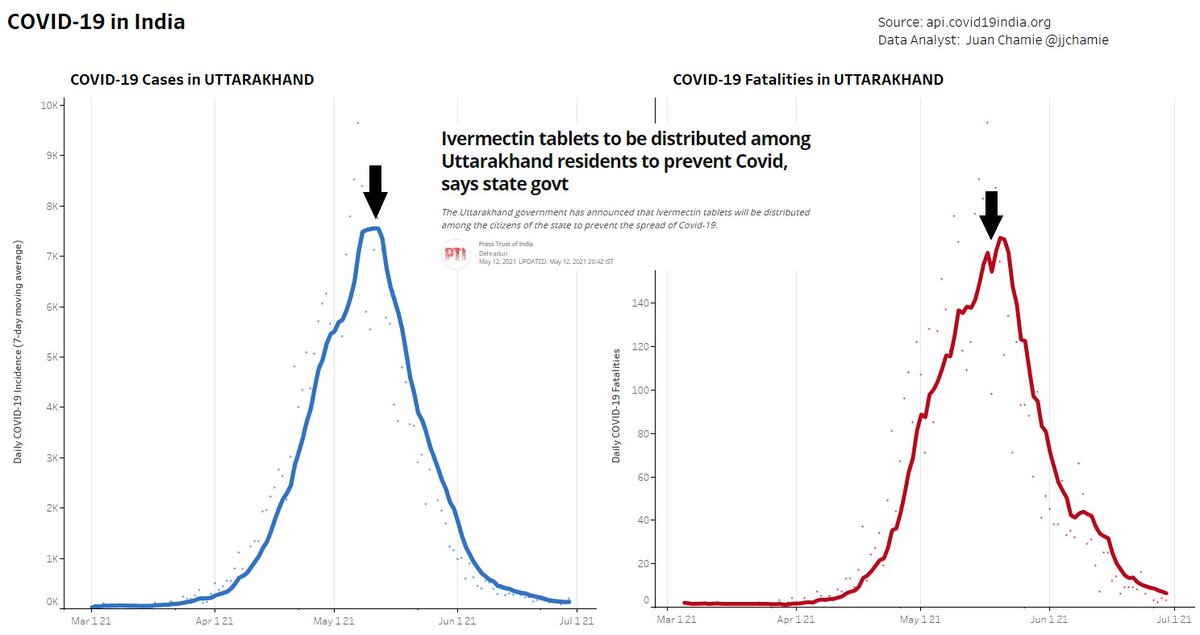
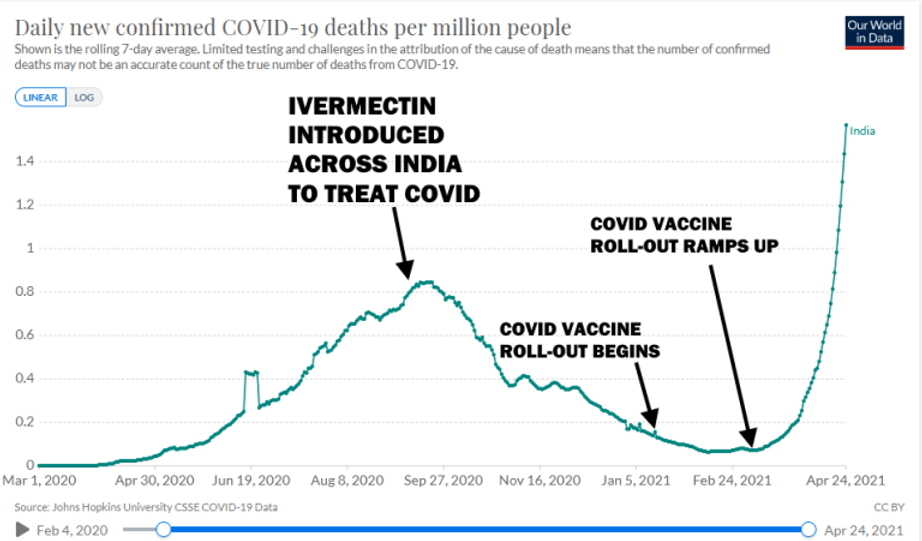
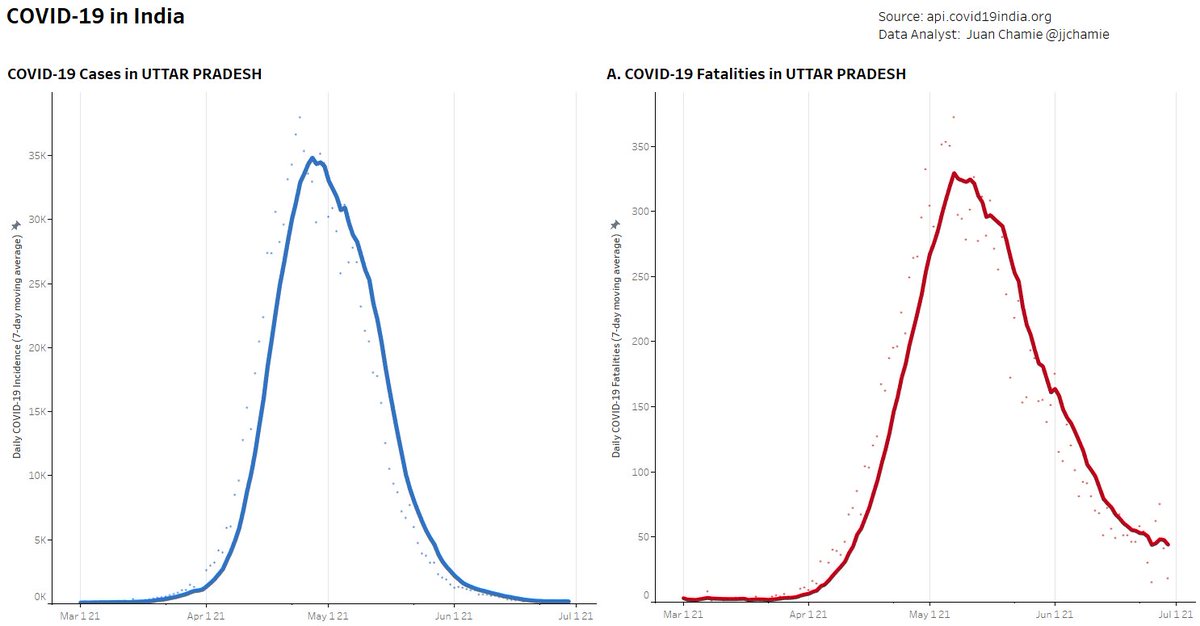
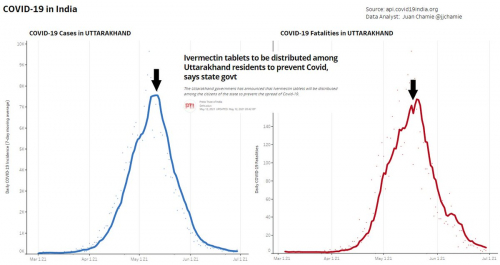
število smrti v Indiji se je znižalo po začetku uporabe zdravila Ivermectina septembra 2020 in se povečalo v korelaciji s povečanjem števila cepljenih ljudi po 11. marcu 2021
*
*
*
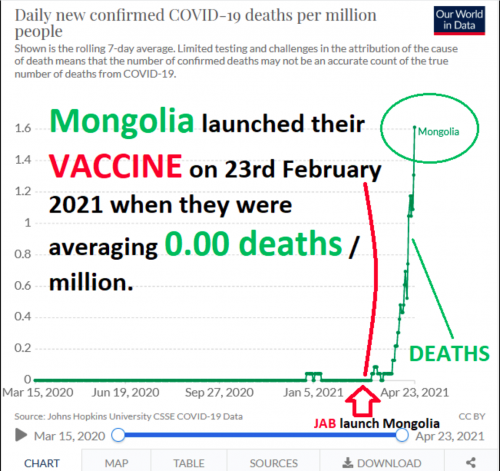
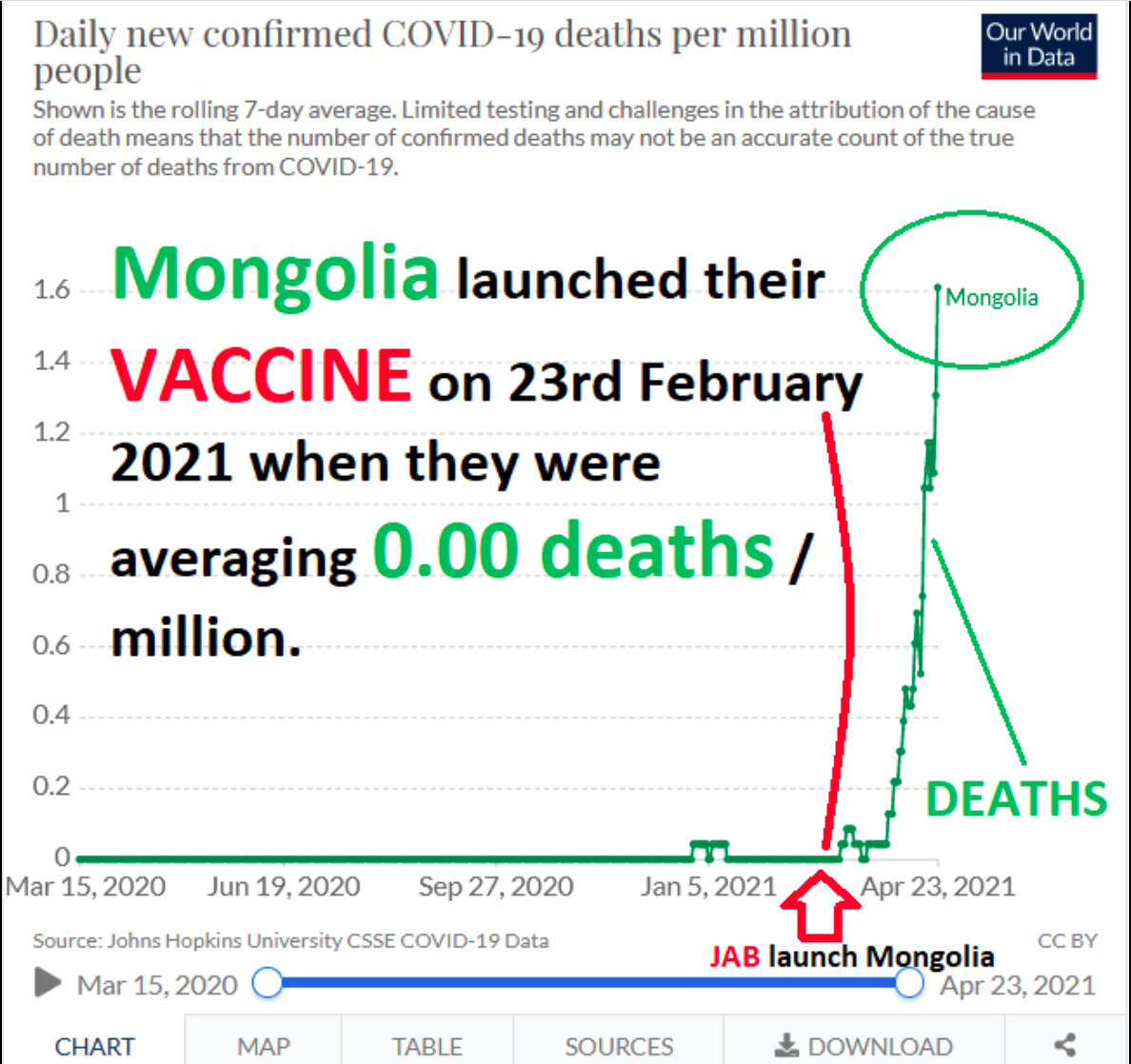
Podobno je v Mongoliji, kjer so se smrti pojavile po začetku cepljenja 23.februarja 2021
*
Indija, ki ima okoli 1,2 milijardi prebivalcev, je imela do aprila 2021 16,96 milijonov primerov pozitivnih PCR testov in 192.311 smrti, domnevno zaradi COVID-19, čeprav je ta statistika vprašljiva, saj vemo, da PCR test ni diagnostično orodje in da se obdukcije, ki bi pokazale pravi vzork smrti, ne izvajajo. V zadnjem mesecu se je število smrtnih primerov v Inidiji povečalo za 8-10 krat, kar je v korelaciji s povečanjem števila cepljenih ljudi.
Vir: https://www.reuters.com/world/asia-pacific/india-coronavirus-cases-set-new-global-record-us-readies-help-2021-04-25/
*
*
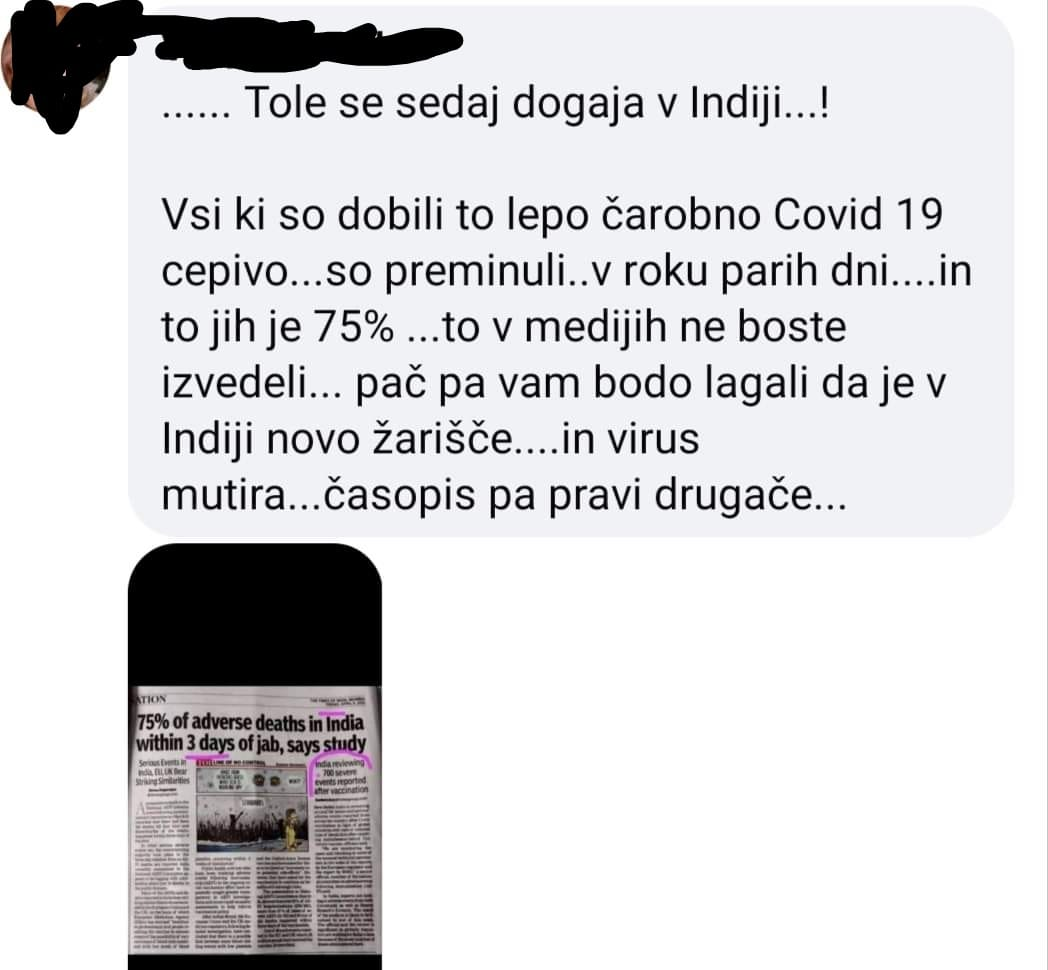
Iz Indije prihajajo tudi poročila o genocidu, lakoti in korupciji, pomanjkanju zdravstvene oskrbe pod krinko COVID-19 pandemije in novih sevov koronaviursa. Ne umirajo zaradi okužb, ampak zaradi lakote, ki je posledica ukrepov zaklepanja, ki uničuje gospodarstva tudi drugih držav po svetu. Vlada in mediji pa lažejo, da gre za nove seve koronavirusa. Osebe, ki nimajo PCR testa, nimajo dostopa do zdravnika. Ker so ukrepi uničili delovna mesta, ni dohodka in ni hrane. Posledica tega je, da zdaj milijoni umirajo zaradi stradanja in ne zaradi koronavirusa.
Vir: https://awakeningnation.com/genocide-and-starvation-in-india-pandemic-corruption/
*
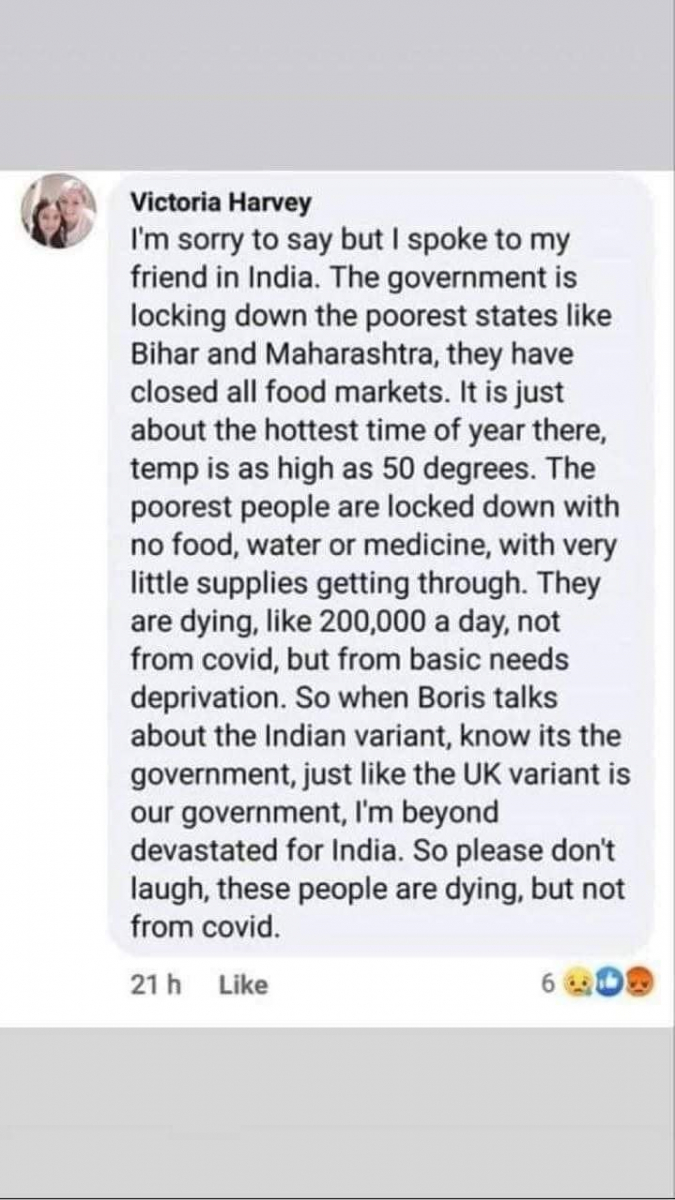
Ta zapis pravi, da je vlada zaklenila najbolj revne države, kot sta Bihar in Maharashtra, kjer so zaprli vse tržnice. Revni ljudje so zaprti brez hrane, vode ali zdravil. Umirajo, tudi po 200.000 na dan, a ne zaradi COVID-19, temveč ker nimajo sredstev za življenje zaradi COVID ukrepov vlade
*
Mediji medtem objavljajo lažne novice o umiranju ljudi na cestah zaradi COVID-19, kar pa so v resnici več let stare slike umiranja ljudi, tudi zaradi spročanja plina v neki indijski državi.


*
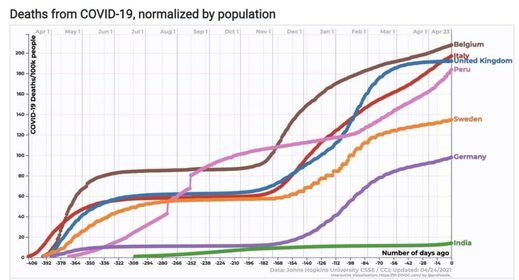
Mediji napihujejo število mrtvih v Indiji zaradi COVID-19, medtem, ko je resnica popolnoma drugačna, kot prikazuje spodnji graf:
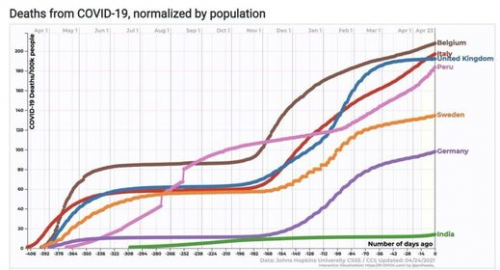
Vidimo lahko, da je relativno število smrti zaradi COVID-19 v Indiji veliko manjše kot v Belgiji, Italiji, Veliki Britaniji ali Nemčiji
Poleg tega smrti, ki se beležijo kot smrti zaradi COVID-19, so v resnici smrti zaradi drugih vzrokov, kot je diareja zaradi pomanjkanja čiste vode in higiene. Med največjimi vzroki smrti v Indiji sta diareja in pljučnica. V Indiji umre vsaki dve minuti en otrok zaradi diareje ali pljučnice. Poleg tega je v mnogih mestih zrak zastrupljen najbolj na svetu, kar vodi v kronične bolezni dihal in slabšo odpornost. Mnogi tuberkulozni bolniki nimajo dostopa do zdravstvene oskrbe in te smrti se potem napačno pripišejo COVID-19. Zaradi tuberkuloze v Indiji svako leto umre več kot 1,4 milijona ljudi, kar je večja epidemija kot COVID-19.
Lažne novice o umiranju zaradi COVID-19 v Indiji so namenjene propagandi za uvajanje obveznega cepljenja.
India je ustavila COVID-19 z Ivermectionom in zdaj so začeli cepiti z VACC1N35, in imajo ekplozijo COVID-19. Tudi zrak je zelo onesnažen, Ivermectin pa ni več na voljo, kot prej. Ivermectiin je učinkovit proti mutacijam koronavirusa. Zakaj nihče letos ni imel gripe?
Kot vzrok smrtonosne katastrofe v Indiji navajajo tudi opustitev uspešnih terapij proti COVID-19 (29), najprej hidroksiklorokina nato pa še ivermectina. V letu 2020 pandemija v Indiji ni bila huda, saj sta bili prebivalcem na voljo uspešni generični zdravili. V kampanji promocije cepljenja so mediji vodili vojno proti zgodnjemu zdravljenju COVID-19 na domu, ki je uspešno potekalo na osnovi varnih zdravil hidroksikolrokina in ivermectina. Preusmeritev vlade iz tega načina zdravljenja na cepiva, je povzročila sedanjo zdravstveno katastrofo.
Zdravnik dr. Suryiu Kantu Tripathiu, voditelj Oddelka za respiratorno medicino na Medicinski univerzi King George v Lucknowu je za India Times povedal, da bi ivermektin lahko zaustavil drugi val okužb. Navedel je, da se ivermektin uporablja več kot devet mesecev brez stranskih učinkov. Je poceni zdravilo, ki stane 2,65 USD na osebo. Prispeval je do 83% zmanjšanju stopnje smrtnosti v bolnišnicah, v katerih so ga uporabljali. Ko so v Indiji prenehali uporabljati ivermectin, je smrtnost začela naraščati, zlasti odkar so pričeli s cepljenjem.*
V mnogih delih Indije so uporabljali tudi hidroksiklorokin, saj so nacionalne smernice potrdile njegovo uporabo v zgodnji fazi COVID-19 bolezni. Po odkritju ivermectina, so nekatere indijske države hidroksiklorokin zamenjale z ivermectinom. Jeseni 2020 je država Uttar Pradesh prebivalcem brezplačno delila ivermektin za uporabo na domu in imela je najnižjo stropnjo smrtnosti, poleg države Bihar, ki je prav tako priporočala ivermektin.
Ob zgodnjem zdravljenju z hidroksiklorokinom in ivermectinom je imela Indija (ki ima 4 krat več prebivalcev kot ZDA) manj kot polovico smrtnih primerov zaradi COVID-19 kot ZDA. Ta uspeh pa ni prepričal indijske vlade in svet za medicinske raziskave je novembra 2020 odsvetoval uporabo ivermektina, z enakim izgovorom kot druge regulatorne agencije, da je potrebno več podatkov.
Ali je farmacevtska industrija, ki ima profitne cilje, spodbujala uporabo cepiv in prepoved uporabe poceni generičnih zdravil?
Če je tako, je takšna prepoved zločin proti človeštvu.
Celoten članek:
Odustajanje od uspješnih terapija zbog pritiska ’Big Pharme’ vjerojatni je uzrok smrtonosne katastrofe zbog COVIDA-19 u Indiji
Trebalo bi biti jasno da je pokušaj brzog procijepljivanja većine svjetske populacije ludost, pogotovo u usporedbi s mogućnošću brzog promicanja i olakšavanja široke upotrebe protokola liječenja na bazi hidroksiklorokina i ivermektina.
4. svibnja 2021. (LifeSiteNews) – Gotovo svaka vijest vrištala je o nevjerojatno visokom broju žrtava od COVIDA-19 u Indiji, hospitalizacija i smrtnih slučajeva. U tim nebrojenim pričama nedostaje činjenica da bi se uzrok porasta slučajeva COVIDA-19 mogao povezati sa smanjenom uporabom dva dokazana generička lijeka za liječenje i prevenciju COVIDA-19: najprije hidroksiklorokin, a kasnije ivermektin.
Kao zagovornik uporabe ova dva lijeka, pregledao sam čvrste podatke iz stvarnog svijeta koji potvrđuju njihovu učinkovitost u liječenju i prevenciji COVID-a u ‘Pandemic Blunder’. Svatko tko iskreno slijedi znanost morao bi zaključiti da oba ova lijeka doista djeluju.
Tijekom 2020. i prvih mjeseci ove godine pandemija COVIDA-19 u Indiji prema svemu sudeći nije bila nimalo poražavajuća. Pažljivo praćenje dobrih vijesti bilo je da su ta dva generička lijeka uvelike osigurana stanovništvu. Tada se u svijetu dogodio pokret za cijepljenje protiv COVIDA-19 i strašan val slučajeva COVIDA-19 pogodio je Indiju.
Glavni mediji su ratovali protiv ranog kućnog/vanbolničkog liječenja COVIDA-19 koje se uspješno globalno provodilo s ta dva generička lijeka, oba s vrlo dugom poviješću sigurnosti. Sad isti mediji smatraju prikladnim usmjeriti pozornost na sve loše vijesti u Indiji. No zašto su mediji zanemarili dokaze da se nagli porast u Indiji može povezati s odlukom vlade da se tijekom nekoliko posljednjih mjeseci stane sa širokom upotrebom ivermektina?
Zašto bi se to dogodilo? Sva negativna medijska kampanja protiv ivermektina svakako je mogla navesti indijsku vladu da svoj prioritet usmjeri na cjepiva. Ako je tako, pokazalo se da je to greška epskih razmjera sa stotinama tisuća Indijanaca koji pate i umiru.
Nažalost, teško je pronaći stvarno zanimanje za preispitivanje mogućeg razloga smanjene upotrebe ivermektina u ovim mračnim danima pandemije COVIDA-19 u Indiji.
Evo nekoliko ključnih članaka. Prvo je članak od 14. travnja “Liječnik vjeruje da lijek ivermektin može pomoći Indiji zaustaviti drugi val COVIDA-19” za časopis India Times govori o dr. Suryiu Kantu Tripathiu, voditelju Odjela za respiratornu medicinu na Medicinskom sveučilištu King George u Lucknowu. On smatra da bi ivermektin “mogao pomoći u preuzimanju kontrole nad novim koronavirusom.” Također je primijećeno da se ivermektin “sada često koristi u raznim državama u Indiji”.
This senior physician also noted this about ivermectin use: “This drug is now being commonly used in various states in India.” This too was noted: “Indian medical institutions have started giving COVID-19 patients Ivermectin off-label. [AT1] Medical institutions across the nation are also giving the drug as a prophylaxis against the novel coronavirus. This is being seen in several states of the nation including Uttar Pradesh and Maharashtra. Dr. Tripathi, in a conversation with Financial Express revealed that the drug has been in use for over nine months now without major side effects being reported.”
Ovaj stariji liječnik također je naveo sljedeće u vezi s upotrebom ivermektina: “Ovaj se lijek danas često koristi u raznim državama u Indiji.” Također je zabilježeno: „Indijske medicinske ustanove počele su pacijentima s COVIDOM-19 davati ivermektin . Medicinske ustanove u cijeloj zemlji također daju lijek kao profilaksu protiv novog koronavirusa. Primjer tome je nekoliko država, uključujući Uttar Pradesh i Maharashtru. Dr. Tripathi, u razgovoru za Financial Express otkrio je da se lijek koristi već više od devet mjeseci i da nisu prijavljene njegove značajnije nuspojave.”
26. travnja pojavila se solidna analiza u blogu pod naslovom “Kad je Indija prestala propisivati ivermektin i započela cijepljenje, smrtnost je skočila.” Ovo su njegova ključna zapažanja: „Još u siječnju govorilo se o ivermektinu, jeftinom i učinkovitom lijeku koji se koristi u Indiji. Međutim, pažnja je usmjerena na cjepivo i od tada je smrtnost porasla te postoje naznake da bi se to moglo ponoviti i drugdje.
U ovoj se priči citira članak iz siječnja 2021. u kojem se naglašava: “Indija je razvila “čudesno” učinkovit i siguran protokol za liječenje COVIDA-19 koji košta samo 2,65 dolara po osobi i pomogao je da stope slučajeva i smrtnosti u zemlji “naglo padnu”. Također je primijećeno da je protokol koji uključuje ivermektin “u prosjeku doveo do 83% niže stope smrtnosti od COVIDA-19 u bolnicama koje su ga primijenile.”
U mnogim dijelovima Indije rano su počeli liječiti bolesnike od koronavirusa, uključujući upotrebu hidroksiklorokina (HCQ). Doktor Makarand Paranjpe i njegova supruga, oboje 77-godišnji indijski liječnici, potpuno su se oporavili od bolesti COVID-19 ranim liječenjem prošlog studenog, izvještava Trial Site News. Ona je koristila hidroksiklorokin, a on je uzimao ivermektin.
“Ukoliko nema nikakvog liječenja, poznato je da virus ulazi u stanice gdje se replicira”, rekao je Paranjpe. “Virus tada stvara bolest koja postaje puno teža.” Zaustavljanje takve replikacije što je ranije moguće jednostavan je učinak ovih jeftinih i sigurnih terapija.
Prošlog ožujka, dok su u SAD-u trajale rasprave o koristi hidroksiklorokina, nakon što je predsjednik Trump odobrio lijek, Indija ga je već preporučila u svojim nacionalnim smjernicama potvrđujući da ga “treba primijeniti što ranije u tijeku bolesti … te ga treba izbjegavati kod bolesnika s teškim oblikom bolesti. “
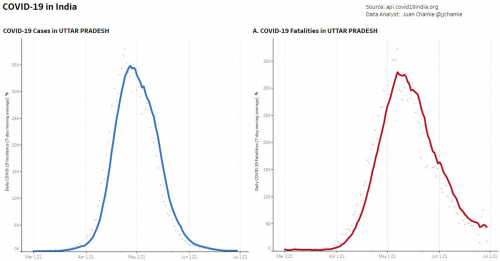
Nakon otkrića učinkovitosti ivermektina u liječenju virusa u lipnju 2020., usporedno sa značajnim naknadnim testiranjima, najveća država u Indiji, Uttar Pradesh (UP) (st. 230 milijuna) objavila je u kolovozu 2020. da za prevenciju i liječenje COVIDA-19 zamjenjuje njihov protokol hidroksiklorokinom primjenom ivermektina.
„Do kraja 2020. godine država Uttar Pradesh – koja je raspodijelila besplatni ivermektin za kućnu njegu – imala je drugu najnižu stopu smrtnosti u Indiji u prosincu s 0,26 na 100 000 stanovnika. Samo je država Bihar sa 128 milijuna stanovnika imala nižu stopu, a također je i ona preporučivala ivermektin ”, navodi Trial Site News.
Daljnjom usporedbom, koristeći rano liječenje hidroksiklorokinom i ivermektinom, gusto naseljena Indija koja ima četiri puta više stanovnika od SAD-a, ima manje od polovice smrtnih slučajeva povezanih s koronavirusom u odnosu na SAD.
Doktor Anil K. Chaurasia, liječnik iz UP-a, potvrdio je da je počevši od sredine rujna 2020. godine “primjetan očiti pad broja slučajeva COVIDA-19 i smrtnih slučajeva u Indiji … [a] nagli pad slučajeva i smrtnost još se uvijek nastavlja.”
Evo najnovijih velikih vijesti iz Indije. Nacionalna vlada suočila se sa stvarnošću. Jerri Lynn izvijestio je u nedjelju 2. svibnja da „ogromni nekontrolirani val zaraza koji pogađa Indiju ima svakakve posljedice za Modijevu vladu. Da povrati kontrolu nad virusom, indijska je vlada prošlog tjedna tiho promijenila smjernice liječenja. Nove smjernice uključuju mogućnost propisivanja dva prenamijenjena lijeka za bolesnike s blagim oblikom COVIDA-19: budezonida i ivermektina. Prvi je inhalacijski steroid za koji je dokazano da smanjuje vrijeme oporavka i potrebu za hitnom medicinskom pomoći.”
Isto tako, zabilježeno je da je „Uttar Pradesh (UP) tijekom 2020. godine liječio više od 300 000 blažih slučajeva COVID-19 bolesnika kod kuće; također se odlučio za upotrebu ivermektina za sprječavanje infekcije. Timovi za odgovor na COVID-19 počeli su uzimati lijek i nisu se zarazili. U.P. je tada naložio da ga uzimaju kontakti zaraženih te su također imali sličan uspjeh.”
No slijedi ružna stvarnost: „Ipak, izuzetan uspjeh UP-a u kontroli virusa nije informirao politiku na nacionalnoj razini – barem ne do sada. Indijsko vijeće za medicinska istraživanja odbilo je u listopadu preporučiti ivermektin u cijeloj zemlji navodeći, poput mnogih zdravstvenih regulatora, potrebu za većom količinom podataka. No sve se to promijenilo prošli tjedan kad je Indija postala najveća zemlja na planetu koja je usvojila upotrebu ivermektina u liječenju COVIDA-19 u cijeloj zemlji.”
Što se to dogodilo da je zaustavljeno široko korištenje ivermektina ne samo u Indiji, već i u SAD-u i mnogim drugim zemljama?
Indijsko vijeće za medicinska istraživanja odbilo je u listopadu preporučiti ivermektin u cijeloj zemlji navodeći, poput mnogih zdravstvenih regulatora, potrebu za većom količinom podataka. U međuvremenu se nastavljaju pozivi mnogih organizacija, uključujući Nacionalni institut za zdravstvo, FDA i Svjetske zdravstvene organizacije, za još više studija o uporabi ivermektina za liječenje i prevenciju COVIDA-19. To su puke gluposti.
Je li industrija lijekova kojoj je jedini cilj profit u Indiji i drugdje potaknula upotrebu cjepiva i izbacila široku upotrebu jeftinih generičkih lijekova?
Ako je tako, trebalo bi biti jasno da je pokušaj brzog procjepljivanja većine svjetske populacije ludost, pogotovo u usporedbi s mogućnošću brzog promicanja i olakšavanja široke upotrebe protokola liječenja na bazi hidroksiklorokina i ivermektina.
Sve svjetske vlade trebala bi učiti iz ispravnog, ali zakašnjelog postupka indijske vlade. Previše ljudi je patilo i umrlo bez potrebe. S preko 570 000 smrtnih slučajeva povezanih s bolesti COVID-19, i još više iz dana u dan, zabrane korištenja ivermektina i hidroksiklorokina trebaju se ukloniti. Smjesta. A one koje to i dalje zabranjuju proglasiti zločincima protiv čovječnosti.
Doktor Joel S. Hirschhorn, kao redoviti profesor na Sveučilištu Wisconsin u Madisonu, vodio je program medicinskih istraživanja između inženjerskih i medicinskih fakulteta. U Kongresnom uredu za Procjenu tehnologije i Nacionalnom udruženju guvernera vodio je velike studije povezane sa zdravljem. Svjedočio je na više od 50 saslušanja u američkom Senatu i Domu te je objavio stotine članaka u časopisima i na web stranicama, također i članke u glavnim novinama. Više od 10 godina izvršni je volonter u velikoj bolnici. Njegova najnovija knjiga je PandemicBlunder.
O cepivih v Indiji: https://www.bbc.com/news/world-asia-india-55748124
Statistika cepljenih: https://www.moderngroup.in/post/here-s-everything-you-need-to-know-about-covid-19-vaccination-latest-statistics
O lakoti v Indiji, ki je posledica ukrepov:
https://scroll.in/article/972732/hunger-and-malnutrition-loom-large-over-india-as-anganwadis-stay-shut-amid-coronavirus-pandemic
https://www.dw.com/en/coronavirus-exacerbates-indias-hunger-problem/a-55299109
https://www.globalsistersreport.org/news/coronavirus/column/india-hunger-may-kill-migrant-laborers-covid-19
https://www.hindustantimes.com/world-news/covid-19-could-kill-more-through-hunger-122-million-more-may-be-pushed-to-starvation-oxfam/story-67nncIVucQYuOEgrAPW6aK_amp.html
https://www.telegraph.co.uk/global-health/science-and-disease/first-coronavirus-now-starvation-hunger-stalks-millions-indians/
https://theconversation.com/how-covid-19-worsens-hunger-in-india-the-worlds-largest-food-basket-142300
https://www.channelnewsasia.com/news/cnainsider/hunger-death-exploitation-plight-poor-poverty-india-covid-19-13618958
https://banthis.tv/watch?id=60872b949a697a0c4361ac80 – Banned.Video
https://www.trtworld.com/asia/massacre-of-data-experts-say-india-is-undercounting-its-covid-deaths-46256?fbclid=IwAR3Y3Cb6SAf7Uc-7QeQ87dl-9lVk-IYlAWrOhGGjdRXF7uc5j-b8b-BDp8Y
*
Despite white, western prop, India (& Pakistan) better than us. Why? According to my family in India/Pakistan, for months , hand-out of medicine kits with HCQ, Ivermectin, Vit D, and zinc. Outbreaks happened in areas where corrupt leaders stopped handing them out. Rocco Gallati, odvetnik Twitter 29.4. 2021
Second, despite this surge, as of now India’s Covid mortality rate is 140 dead/million. This compares to 401 for the world average, 1,762 for the US, and 1,869 for the UK. It puts India 119th in the world on this, the single most important statistic for comparison purposes.
*
https://www.24ur.com/novice/tujina/mukormikoza-crna-gliva-ki-napada-covidne-bolnike-v-indiji.html
*
*
Študija: COVID-19 cepivo poslabša klinično bolezen: https://pubmed.ncbi.nlm.nih.gov/33113270/
*
Nobel Prize winner: Mass COVID vaccination an ‘unacceptable mistake’ that is ‘creating the variants’
May 19, 2021 (LifeSiteNews) – French virologist and Nobel Prize winner Luc Montagnier called mass vaccination against the coronavirus during the pandemic “unthinkable” and a historical blunder that is “creating the variants” and leading to deaths from the disease.
“It’s an enormous mistake, isn’t it? A scientific error as well as a medical error. It is an unacceptable mistake,” Montagnier said in an interview translated and published by the RAIR Foundation USA yesterday. “The history books will show that, because it is the vaccination that is creating the variants.”
Many epidemiologists know it and are “silent” about the problem known as “antibody-dependent enhancement,” Montagnier said.
“It is the antibodies produced by the virus that enable an infection to become stronger,” he said in an interview with Pierre Barnérias of Hold-Up Media earlier this month.
Vaccination leading to variants
While variants of viruses can occur naturally, Montagnier said that vaccination is driving the process. “What does the virus do? Does it die or find another solution?”
“It is clear that the new variants are created by antibody-mediated selection due to the vaccination.”
Vaccinating during a pandemic is “unthinkable” and is causing deaths, the winner of the 2008 Nobel Prize in Medicine for discovery
‘Deaths follow vaccination’
“The new variants are a production and result from the vaccination. You see it in each country, it’s the same: in every country deaths follow vaccination,” he said.
A video published last week on YouTube uses data from the Institute for Health Metrics and Evaluation at the University of Washington to illustrate the spikes in deaths in numerous countries across the globe after the introduction of COVID vaccination, confirming Montagnier’s observation.
https://www.youtube.com/watch?v=KrIoPIQZmUE
The French interviewer pointed to data from the World Health Organization (WHO) showing that since the vaccines were introduced in January, new infections contamination have “exploded,” along with deaths, “notably among young people.”
“Yes,” agreed Montagnier who is a professor at Shanghai Jiao Tong University. “With thrombosis, etc.”
Thrombosis – or blood clots — have been an unexpected problem linked to the new coronavirus vaccines and the cause of AstraZeneca’s vaccine being pulled in several countries. The head of Canada’s public health agency, Theresa Tam, told a press conference Tuesday that there are now 21 confirmed cases of vaccine-induced thrombotic thrombocytopenia, or VITT, including among three women who died from the blood-clotting disorder potentially linked to AstraZeneca’s vaccine and another 13 cases are under investigation.
Breakthrough cases
Montagnier said that he is currently conducting research with those who have become infected with the coronavirus after getting the vaccine. The Centers for Disease Control and Prevention reported in April that it had received 5,800 reports of people who had “breakthrough” COVID after being vaccinated, including 396 people who required hospitalization and 74 patients who died.
“I will show you that they are creating the variants that are resistant to the vaccine,” Montagnier said.
Coronavirus made in a lab
The famous French virologist created waves in April 2020 when he told a French television station that he believed SARS-CoV2, the new pandemic coronavirus, was man-made in a laboratory. The “presence of elements of HIV and germ of malaria in the genome of coronavirus is highly suspect and the characteristics of the virus could not have arisen naturally,” he said.
Though he was ridiculed by French experts for having “a conspiracy vision that does not relate to the real science,” Montagnier published a paper in July 2020 supporting his claims that the novel coronavirus must have originated from human experimentation in a lab – a theory that has recently resurfaced and is currently considered the most likely origin of the virus.
*
The death rate is spiraling out of control in India, but only after the spike protein-spreading, inflammation-causing covid-19 vaccines were unleashed by the millions.
Infectious disease is ravaging India, from tuberculosis to malaria, as covid vaccines cause severe inflammation, weakening the population
Thousands of people are dying from infections every day in India, and many of the deaths are not recorded in any official register. Tuberculosis, typhus, malaria, cholera, influenza, and covid-19 are just a few infectious diseases that are ravaging the nation.
A once rare fungal infection called mucormycosis has become opportunistic in recovered and recovering covid-19 patients. Mucorymycosis is caused by exposure to mucor mold, commonly found in soil, plants, manure and decaying fruits and vegetables. Another infection that is taking advantage of weak immune systems is scrub typhus. Nearly a million cases are reported every year in Asia. Scrub typhus can affect the central nervous system, cardiovascular system, renal, respiratory and gastrointestinal systems, leading to pneumonia or death. The most concerning infectious disease is tuberculosis (TB) and a host of drug-resistant variants. India has the highest incidence of TB, with 2.8 million cases and 435,000 deaths each year.
Covid-19 has only made the situation worse. People with respiratory symptoms similar to pneumonia and tuberculosis are dying with covid-19, and the number of deaths is climbing like never before as medical systems collapse. India is currently reporting more covid-19 fatalities in a single day than any other country did at any time during the past year and a half. More than 186 million vaccinations have been used throughout the country since January of 2021. Why are people suddenly becoming more susceptible to coronavirus and other infections in India after the mass vaccination push? Is it because the science of the innate immune system is being ignored and suppressed in the push to poison people with more vaccines that cause severe issues such as Antibody Dependent Enhancement (pathogenic priming) and virus interference (increased susceptibility to infection)?
How might vaccination be causing the sudden death spiral in India?
A private testing company found that two out of every three people in India already have measurable levels of antibodies in their system. A majority of the population currently has immunity to covid-19, so why are fatalities spiking at this time?
More than 186 million vaccinations have been used throughout the country since January of 2021. Before the mass vaccination campaign, India was doing a great job managing infections and preventing excess deaths. After the vaccines, the death rate climbed out of control. Today, there are now 3,532 circulating covid-19 “variants” in India, and they all flourished almost immediately after people started getting mass injected with the “vaccines.”
The average number of coronavirus deaths per day in India was well below 100 people for the first three months of the worldwide lockdowns. The country saw that number go up to 1,000 deaths per day in August and September, right after masks mandates were imposed with police state power. The infections subsided by January of 2021. At that time, the deaths per day was well below 100 again. However, as the vaccines were rolled out, the death rate shot up like never before, eclipsing 1,500 per day by April and surpassing 4,500 deaths per day in May!
Why would thousands more people die every day if a majority of people were recovering with antibodies? Why would thousands of more people be dying per day, if millions of vaccines were guaranteeing immunity? Could vaccine-induced Antibody Dependent Enhancement be at play? Could the vaccines be spreading spike proteins from the vaccinated, putting the unvaccinated at risk?
The vaccines are not only poisoning people’s bodies and making them more susceptible to infection complications (virus interference), but they are also priming immune systems to fail when re-exposed to coronavirus strains in the wild (Antibody Dependent Enhancement). According to the clinical studies, the covid vaccines elicit neutralizing antibodies that sensitize vaccine recipients to more severe disease. Furthermore, the fatigue, fever, eye disorders, soreness, numbness, facial paralysis and blood clots that result from the vaccines are signs that the vaccines are causing severe inflammation, making people more susceptible to a variety of infections. Even more, a mass vaccination campaign can force coronaviruses to evolve more rapidly, leading to the accelerated adaptation of spike proteins and the emergence of new variants. Scientists in Britain believe the B.1.617.2 variant circulating in India is 50 percent more infectious.
Moreover, the vaccines function like autoimmune disease bioweapons, forcing people’s bodies to churn out spike proteins that can lead to environmental exposure and rapid evolution of infectious virus particles. The unvaccinated are being exposed to countless spike proteins from vaccinated people. These reasons may help explain why the death toll is suddenly out of control in India and why bodies are washing up in droves along the shorelines of the Ganges.
*
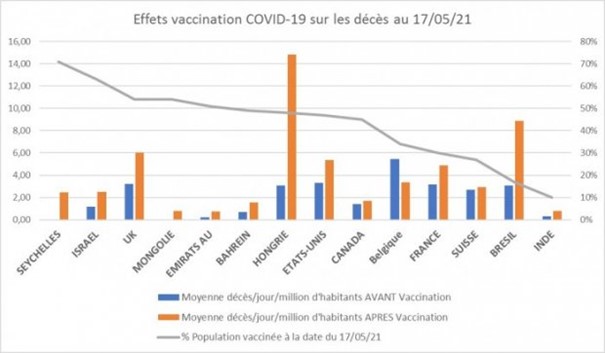
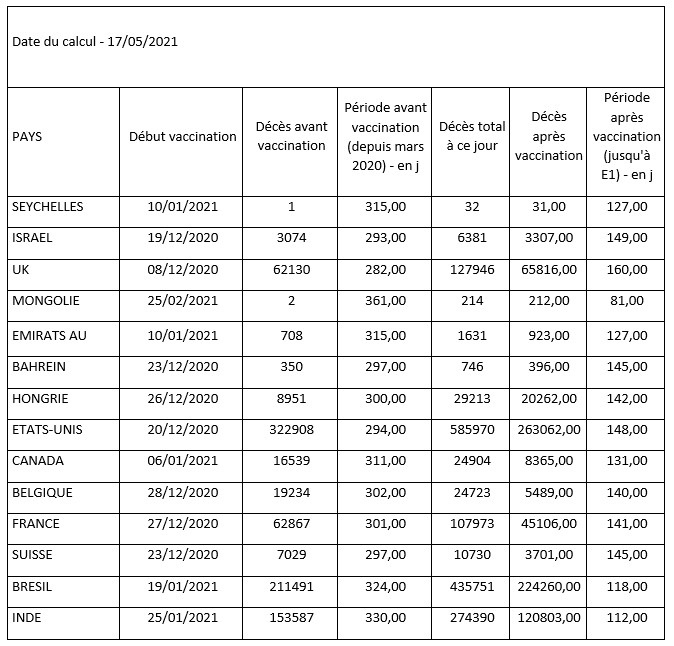
V vseh naslednjih državah: SEJHELI, IZRAEL, UK, MONGOLIJA, ZAE, BAHRAIN, MADŽARSKA, ZDA, KANADA, Francija, ŠVICA, BRAZILIJA, INDIJA, od začetka cepljenja vsak dan umre več ljudi .
Tako se 17. 5. 21 v Braziliji (17% prebivalstva, ki je prejelo vsaj en odmerek) povprečna dnevna smrtnost pomnoži s TRI; na Madžarskem s PET (48% prebivalstva je prejelo vsaj en odmerek); v Franciji je povečanje za več kot 1,5 (30% prebivalstva, ki je prejelo vsaj en odmerek) ...
Avtorja: Gabriel Faugloire in Frédéric Gobert
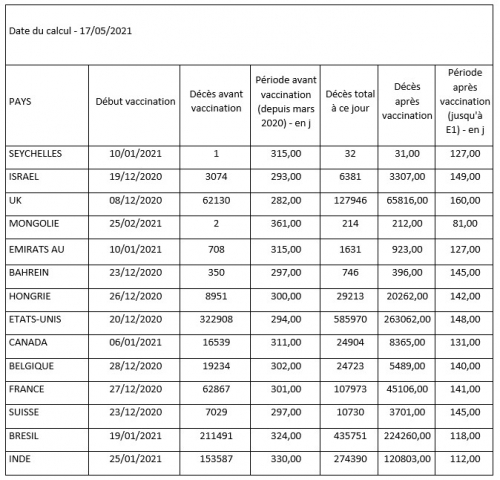
Kako so bile izračunane zgornje številke?
Vsi podatki prihajajo s spletnega mesta " ourworldindata " in se ustavijo na dan 17. 5. 21; 14 držav je bilo izbranih tako, da je kar največ heterogenosti, tako glede notranjih značilnosti kot tudi glede stopnje cepljenja posamezne države. Prvotna ideja je bila potrditi informacije, ki jih je Jean-Jacques Crèvecœur posredoval v manjšem obsegu. Iz njih je razvidno, da se je povprečna dnevna umrljivost zaradi COVID-19 povečala v skoraj vseh proučevanih državah od začetka kampanj cepljenja ; le Belgija je izjema.
Tudi če se zdi neposredna povezava s cepljenjem hitra bližnjica, se lahko iskreno vprašamo, kaj bi to lahko pojasnilo drugače ... Treba bi bilo vedeti, da bi to potrdili ali zanikali, število umrlih COVID ljudi, ki so bili cepljeni. V tem času vidimo, da je primer Sejšelov in Mongolije ogromen (1 in 2 smrtni primeri prej, 31 oziroma 212 pozneje!), Brazilija je impresivna, Madžarska pa preprosto osupljiva. Prav tako vidimo, da je v Indiji, katere mediji so zadnjo epidemijo spremenili v katastrofo, stopnja smrtnosti precej nižja od naše (treba je povedati, da številne države že dolgo uporabljajo ivermektin!).
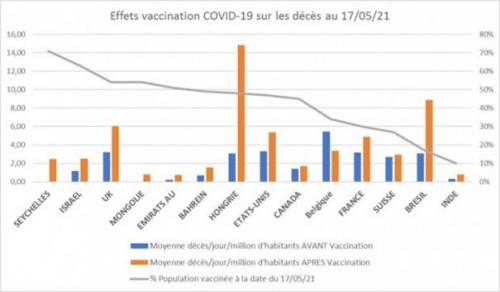
Nad ustreznim grafom bolj vizualno: predstavlja povprečno število umrlih / dan / milijon prebivalcev pred (modra črta) in po cepljenju (oranžna črta), razvrščeno od leve proti desni države, v kateri je največ % cepljenega prebivalstva (Sejšeli ) manj % (Indija). Odstotek cepljenega prebivalstva (siva krivulja) .
V vlogo "velikih" medijev in večine strani Factchecker za "preverjanje dejstev" je treba znova in vedno podvomiti; njihova odgovornost za laži in neumnosti, ki krožijo in jih javnost upošteva, je ogromna: večja teža smrtnosti zaradi covida v Indiji v primerjavi s Francijo je laž; izjemna resnost covid epidemije je laž; varnost "cepiv" ali najboljše razmerje "korist / tveganje" je laž; življenjski interes nošenja maske na prostem je laž; demokratičnost in spoštovanje svoboščin sanitarne izkaznice je laž; trditev, da za zdravilo covid ni zdravila je laganje; trditev, da je "cepivo" edina rešitev je laž; sistematično neizpraševanje nesmisla vladne "zdravstvene" politike: nihamo med slepoto zaradi strahu, kolektivne psihoze, kompromisa in strahopetnosti; itd. A vseeno se od marca 2020 v človeških življenjih plačuje cena bankrota glavnih medijev.
Vir: https://reseauinternational.net/depuis-quon-vaccine-anticovid-la-mortalite-moyenne-quotidienne-a-augmente-dans-13-pays-sur-14/
*
Povečanje smrtnosti po cepivu za COVID-19
https://www.youtube.com/watch?v=xSrc_s2Gqfw&t=9s
*
Explosion of 3,500 new covid “variants” follows mass vaccination campaign in India
Thursday, May 20, 2021 by: Ethan Huff
There are now 3,532 circulating Wuhan coronavirus (Covid-19) “variants” in India, new reports indicate, and they all came about almost immediately after people started getting mass injected with the “vaccines.”
According to a May 6 report from The Hindu, 27 states throughout India are confirmed to be afflicted with these variants, which were identified from 13,000 samples that were sequenced for variants. Among the 3,532 variants identified, 1,527 were found to be B.1.6.1.7, or “double mutant,” variants.
This news prompted the Indian government to announce a “third wave” of the Chinese Virus, which it says is “inevitable looking at the current surge in infections.”
The B.1.1.7 variant said to be circulating throughout the United Kingdom is supposedly on the decline in India, while another double mutant strain known as B.1.617 is said to be on the rise.
The Indian government says that B.1.617 could be linked to the “second wave” that reportedly caused a number of deaths in past weeks.
“The current surge in cases seen over the last and a half month in some states shows a correlation with the risk of the Indian mutant variant,” announced S.K. Singh, director of India’s National Center for Disease Control (NDCC).
“The U.K. variant is declining in proportion across the country in the last one and half months.”
The “vaccines” are spreading the variants, and communist China is laughing about it
Right around the time that the mainstream media began reporting these numbers and talking about scary new variants of the Wuhan Flu, Kamala Harris issued a travel ban against India.
Since the first, second and however many Chinese Virus “waves” there have been at this point have all fizzled out, the establishment is now working overtime to try to reignite fear about even more waves in order to keep people scared and muzzled inside their homes for the rest of their lives.
In talking about its record-breaking daily death toll, India’s health ministry blamed the “variants” rather than discussing the elephant in the room. Everything was fine in India until the mass vaccination campaigns began, and now more people are dying daily than ever before.
Could it be that the injections are responsible? The obvious answer is yes. But as long as the mainstream media refuses to connect the dots, many will believe that the variants are spreading through the air, necessitating the creation of even more deadly vaccines.
This vaccine addiction will be the downfall of the planet, which has been brainwashed into believing that every sniffle requires another injection as a “cure.” And with each new injection comes more disease, creating an endless cycle of diseases and vaccines.
Meanwhile, India is trying to save face by putting out messaging claiming that the situation is under control and that other countries should not worry. Communist China, in response, has been mocking India and the mass death that is occurring there.
The Chinese Communist Party (CCP) certainly knows that the injections are spreading the disease, seeing as how both were made in China – thanks to Anthony Fauci.
How quickly many have forgotten that we would not even be in this mess were it not for the machinations hatched in Wuhan a year-and-a-half ago. Both the East and the West were involved in the unleashing of all this, and there is no end in sight to the madness.
“Truth can never be buried forever; it will come out,” says GNews “With the help of the Whistleblower movement, people and countries around the world will find out the truth about the origin of the CCP virus soon.”
More related news about the Wuhan coronavirus (Covid-19) death jabs can be found at ChemicalViolence.com.
https://www.naturalnews.com/2021-05-20-3500-covid-variants-mass-vaccination-campaign-india.html
*
The World Health Organization (WHO) Monday elevated India’s COVID variant B.1.617 from a “variant of interest” to a “variant of global concern.” The variant, which was first isolated in India, is believed to be driving the country’s brutal second wave.
In a follow-up statement today, the WHO said the B.1.6.1.7 variant has since spread throughout India and at least “44 countries in all six WHO regions.”
Maria Van Kerkhove, the WHO’s technical lead for COVID, said during Monday’s press conference new data under peer review shows B.1.617 is more transmissible than earlier strains of the virus.
Van Kerkhove said the variant may be able to evade some of the protections provided by vaccines, as a surprising number of patients who have already been fully vaccinated have been found to be infected with the strain.
“Even though there is increased transmissibility demonstrated by some preliminary studies, we need much more information about this virus variant in this lineage in all of the sub lineages, so we need more sequencing, targeted sequencing to be done,” Van Kerkhove said.
One version of the variant, which first emerged in the state of Maharashtra in late 2020 or early 2021, was elevated to a “variant of concern” in the UK last week.
Variants are classified as “variants of concern” when there is evidence they spread more rapidly, cause more severe disease, evade previously acquired immunity better than circulating versions of the virus, or reduce the effectiveness of public health measures, vaccines or medications.
Van Kerkhove said there was nothing to suggest diagnostics, therapeutics and vaccines don’t work.
“With millions of people around the world infected with this virus, new mutations arise every day,” Gregg Gonsalves, associate professor of epidemiology at Yale University, said in March. “Unless we vaccinate the world, we leave the playing field open to more and more mutations, which could churn out variants that could evade our current vaccines and require booster shots to deal with them.”
Quarraisha Abdool Karim, associate scientific director of the Centre for the Aids Programme of Research in South Africa and professor in clinical epidemiology at Columbia University, said scientists, advocates and decision-maker must ensure that as many people are vaccinated all over the world and as soon as possible so that everyone will be safe from COVID and prepared for the next pandemic.
New variant evades Pfizer vaccine
After the WHO’s press conference, the Financial Times reported on a new study that showed the B.1.617 variant has “modest ability” to avoid antibodies elicited by Pfizer’s COVID vaccine, though an extensive vaccination campaign is likely to reduce transmissions.
Research by Ravindra Gupta, a virologist at the University of Cambridge, UK, suggests antibodies are slightly less effective against the variant than against others. The team collected blood serum from nine people who had received one dose of the Pfizer vaccine and tested it against a harmless carrier virus modified to contain the SARS-CoV-2 spike protein, with the mutations from B.1.617.
Gupta’s team discovered neutralizing antibodies generated by vaccinated individuals were about 80% less potent against some of the mutations in B.1.617. Researchers also found that healthcare workers in Delhi vaccinated with the Oxford–AstraZeneca vaccine were reinfected mostly with the B.1.617 variant.
A German team tested serum from 15 people who were previously infected with SARS-CoV-2, and found their antibodies neutralized B.1.617 about 50% less effectively than previously circulating strains. When they tested serum from participants who received two doses of the Pfizer vaccine, they found antibodies were about 67% less potent against B.1.617.
According to vaccinologist Philip Krause, chair of the WHO working group on COVID-19 vaccines, if vaccine-resistant SARS-CoV-2 strains emerge, vaccines might need to be updated and regulators might balk at authorizing them without seeing updated safety and efficacy data. If new variants circulate alongside older strains, multivalent vaccines, effective against several lineages, might be needed.
“The not-so-good news is that the rapid evolution of these variants suggests that if it is possible for the virus to evolve into a vaccine-resistant phenotype, this may happen sooner than we like,” said Krause.
Mass vaccination could cause highly infectious variants
Geert Vanden Bossche, Ph.D., certified expert in biology and virology and seasoned vaccine developer who’s worked with GSK Biologicals, Novartis Vaccines, Solvay Biologicals and the Bill & Melinda Gates Foundation, argued in a letter to the WHO that mass infection prevention and mass vaccination with leaky COVID-19 vaccines in the midst of the pandemic will only breed highly infectious variants.
Vanden Bossche’s concerns center around the notion that a combination of lockdowns and extreme selection pressure on the virus induced by the intense global mass vaccination program might diminish the number of cases, hospitalizations and deaths in the short-term, but ultimately could induce the creation of more concerning mutants.
Selection pressure will cause greater convergence in mutations that affect the critical spike protein of the virus that is responsible for breaking through the mucosal surfaces of our airways, the route used by the virus to enter the human body. The virus will outsmart the highly specific antigen-based vaccines that are being used and tweaked, dependent on the circulating variants leading to an increase in serious and potentially lethal cases — in effect, an out-of-control pandemic.
This is the result of what Vanden Bossche calls “immune escape” — incomplete sterilization of the virus by the human immune system or following vaccination resulting in more people who have had COVID remaining susceptible to reinfection.
Immune escape induces vaccine companies to further refine vaccines that will add, not reduce, the selection pressure, producing ever more transmissible and potentially deadly variants.
“There can be no doubt that continued mass vaccination campaigns will enable new, more infectious viral variants to become increasingly dominant and ultimately result in a dramatic incline in new cases despite enhanced vaccine coverage rates,” Vanden Bossche said. He added that mass vaccination could “lead to complete resistance of circulating variants to the current vaccines.”
*
Komentar na indijsko študijo o profilaktični uporabi Ivermectina.
On May 7, 2021, during the peak of India's Delta Surge, The World Health Organization reported, "Uttar Pradesh (is) going the last mile to stop COVID-19."
The WHO noted, "Government teams are moving across 97,941 villages in 75 districts over five days in this activity which began May 5 in India's most populous state with a population of 230 million."
The activity involved an aggressive house-to-house test and treat program with medicine kits.
The WHO explained, "Each monitoring team has two members who visit homes in villages and remote hamlets to test everyone with symptoms of COVID-19 using Rapid Antigen Test kits. Those who test positive are quickly isolated and given a medicine kit with advice on disease management."
The medicines comprising the kit were not identified as part of the Western media blackout at the time. As a result, the contents were as secret as the sauce at McDonald's.
The WHO continued, "On the inaugural day, WHO field officers monitored over 2,000 government teams and visited at least 10,000 households."
This news story was published on the WHO Official Website in India. The website details the WHO’s work against COVID-19 in India, including a discussion about their “Online course for Rapid Response Teams.”
Such teams are the very government teams discussed above assigned to conduct the house-to-house test and treat program in Uttar Pradesh. In discussing the role of the Rapid Response Team (RRT), the WHO site reports,
“RRTs are a key component of a larger emergency response strategy that is essential for an efficient and effective response…WHO has produced and published this course for RRTs working at the national, sub-national, district, and sub-district levels to strengthen the pandemic response with support from the National Center for Disease Control, Ministry of Health & Family Welfare, Government of India, and the U.S. Centers for Disease Control and Prevention.”
The Rapid Response Teams derive support from the United States CDC under the umbrella of the WHO. This fact further validates the Uttar Pradesh test and treat program and solidifies this as a joint effort by the WHO and CDC.
https://www.who.int/india/news/detail/16-09-2021-online-course-for-rapid-response-teams
Perhaps the most telling portion of the WHO article was the last sentence, “WHO will also support the Uttar Pradesh government on the compilation of the final reports.”
None have yet been published.
Just five short weeks later, on June 14, 2021, new cases had dropped a staggering 97.1 percent, and the Uttar Pradesh program was hailed as a resounding success. According to ZeeNews of India, "The strategy of trace, test & treat yields results."
"The Yogi-led state has also been registering a steep decline in the number of Active COVID Cases as the figure has dropped from a high of 310,783 in April to 8,986 now, a remarkable reduction by 97.10 percent."
By July 2, 2021, three weeks later, cases were down a full 99 percent.
On August 6, 2021, India’s Ivermectin media blackout ended with MSN reporting. Western media, including MSN, finally acknowledged what was contained in those Uttar Pradesh medicine kits. Among the medicines were Doxycycline and Ivermectin.
On August 25, 2021, the Indian media noticed the discrepancy between Uttar Pradesh's massive success and other states, like Kerala's, comparative failure. Although Uttar Pradesh was only 5% vaccinated to Kerala's 20%, Uttar Pradesh had (only) 22 new COVID cases, while Kerala was overwhelmed with 31,445 in one day. So it became apparent that whatever was contained in those treatment kits must have been pretty effective.
News18 reported, "Let’s look at the contrasting picture. Kerala, with its 3.5 crore population - or 35 million, on August 25 reported 31,445 new cases, a bulk of the total cases reported in the country. Uttar Pradesh, the biggest state with a population of nearly 24 crore - or 240 million - meanwhile reported just 22 cases in the same period.
Two days ago, just seven fresh positive cases were reported from Uttar Pradesh. Kerala reported 215 deaths on August 25, while Uttar Pradesh only reported two deaths. In fact, no deaths have been reported from Uttar Pradesh in recent days. There are only 345 active cases in Uttar Pradesh now while Kerala’s figure is at 1.7 lakh - or 170,000."
"Kerala has done a much better job in vaccination coverage with 56% of its population being vaccinated with one dose and 20% of the population being fully vaccinated with a total of 2.66 crore - or 26.6 million - doses being administered.
Uttar Pradesh had given over 6.5 crore - or 65 million - doses, the maximum in the country, but only 25% of people have got their first dose while less than 5% of people are fully vaccinated. Given the present COVID numbers, Uttar Pradesh seems to be trumping Kerala for the tag of the most successful model against COVID."
This author reviewed the reasons behind Kerala’s failed treatment model in two articles, “The Lesson of Kerala” and “Kerala’s Vaccinated Surge.”
By September 12, 2021, Livemint reported that 34 districts were declared COVID-free or had no active cases. Only 14 new cases were recorded in the entire state of Uttar Pradesh.
On September 22, 2021, YouTube hosted a video by popular science blogger Dr. John Campbell detailing the Uttar Pradesh success story. He gave a breakdown of the ingredients and dosages of the magical medicine home treatment kit responsible for eradicating COVID in Uttar Pradesh. The same kit was also used in the state of Goa.
Dr. John Campbell broke India's Ivermectin Blackout wide open on YouTube by revealing the formula of the secret sauce, much to the dismay of Big Pharma, the WHO, and the CDC. Readers will want to watch this before it is taken down. See mark 2:22.
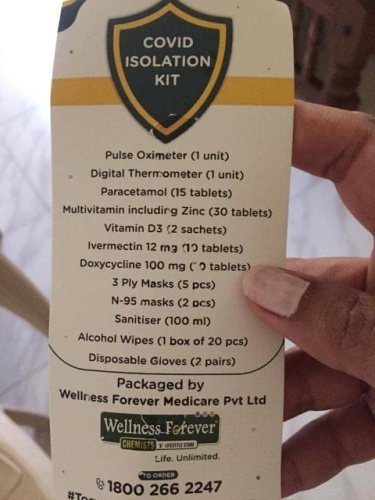
Each home kit contained the following: Paracetamol tablets [tylenol], Vitamin C, Multivitamin, Zinc, Vitamin D3, Ivermectin 12 mg [quantity #10 tablets], Doxycycline 100 mg [quantity #10 tablets]. Other non-medication components included face masks, sanitizer, gloves and alcohol wipes, a digital thermometer, and a pulse oximeter. See mark 2:33.
Campbell reports that the exciting things in the kit that grabbed his attention were: Zinc, Vitamin D3, Ivermectin, and secondary antibiotic treatment. "Interesting, that’s what the government decided to give." See mark 3:40
John Campbell has reviewed repurposed drugs for COVID before. He has interviewed both Dr. Tess Lawrie and Dr. Pierre Kory. Repurposed drugs hold the potential for benefitting many conditions, not the least of which include viruses and cancers.
https://www.amazon.com/Surviving-Cancer-COVID-19-Disease-Repurposed/dp/0998055425
Dr. Campbell noted that there had been no recent cases in 59 Uttar Pradesh districts. In addition, out of 191,446 tests completed in the previous 24 hours, only 33 samples were positive for a test positivity rate of only 0.01%. Dr. Campbell called this low number "staggering." See mark 5:05.
By September, cases had fallen dramatically. Out of the entire state of 200 million plus inhabitants, only 187 active cases were left compared to the peak in April of 310,783 cases. See mark 5:41.
Dr. Campbell attributes their success to many factors, including early detection and early treatment with kits costing a mere $ 2.65 per person. See mark 6:20.
Notice that Dr. Campbell does not mention a single person who had any toxicity from those ten 12 mg pills of Ivermectin - in the entire state of over 200 million. Not one poisoning was reported. No Indian poison control articles or telephone calls were reported. Out of millions of distributed medicine kits, each containing 120 mg of Ivermectin, not one person in Uttar Pradesh was reported to have had a problem with the drug.
Notice that Dr. Campbell at no time criticizes the medicine kit as "fringe" or ineffective. After all, it would be improper to accuse a WHO-sponsored program such as the Uttar Pradesh test and treat – coordinated by WHO – of being “fringe.”
Contrary to what little we receive - at great expense - from the government in the United States, these kits are efficient and contain gloves, a thermometer, and an oximeter. The last time I purchased an oximeter some ten years ago, it cost some $200.00. This entire kit – including the oximeter – costs only $2.65.
And notice that a government can purchase over one thousand home treatment Ivermectin containing kits for the price of one course of Remdesivir. Remdesivir runs $3,100, and it is an impractical drug as it must be given late in the disease during hospitalization. Moreover, it is a drug that does not save lives.
https://www.nejm.org/doi/full/10.1056/nejmoa2007764
https://www.nytimes.com/2020/10/15/health/coronavirus-remdesivir-who.html
On the other hand, the Ivermectin kits are highly correlated with eliminating COVID-19 in Uttar Pradesh. Indeed with less than 11% of their population fully vaccinated, the Uttar Pradesh model of test and treat is superior not only to Kerala, with a much higher percent vaccinated. Uttar Pradesh beats the UK, the US, and nearly everywhere else in the world in terms of the lowest active COVID cases.
Rather than turning a blind eye to Uttar Pradesh, perhaps it is time to analyze its success. It is time for all to realize that far from being dangerous, Ivermectin is safer than hand sanitizer or plain Tylenol, judging from the number of United States poison control calls.
Now is precisely the moment to point out that Dr. George Fareed, Dr. Peter McCullough, and Dr. Harvey Risch were correct in their U.S. Senate Testimony on November 19, 2020. They advised that early outpatient treatment was essential and would save hundreds of thousands of American lives if adopted. It wasn’t.
Now is the right moment to notice the onslaught of United States poison control articles attempting to smear Ivermectin, a drug proven safe and effective in the Uttar Pradesh test-and-treat program administered under the auspices of both the WHO and CDC.
It is appropriate to remind the reader that the WHO and CDC possess direct and recent knowledge of Ivermectin use for COVID-19 in India. Moreover, they know better than anyone the colossal effectiveness and overwhelming safety of Ivermectin used in those millions of Uttar Pradesh test and treat kits.
Perhaps it is also time to ask why exactly Dr. Tess Lawrie’s peer-reviewed meta-analysis was given an Altimetric score of 26,697, making it number eight out of some 18 million publications.
https://hopepressworks.org/f/ivermectin-meta-analysis-by-dr-tess-lawrie-nears-most-cited-ever
This rank is far better than the top 1%, which would only need a ranking of 180,000 for it to rank in the top 1%. It would only need 18,000 for it to rank in the top .1%. Ranking in the top .001% would mean #180. Therefore, at number eight, it is 8/180 of the top .001% or roughly the top 4.4% of the top .001%. This article ranks in the top 5% of the top .001%!
In other words, only seven articles in the world out of those 18 million are ranked higher.
This peer-reviewed paper is one of the most cited of medical references of all time – period. That should alert any reader – immediately - to its historical significance. Dr. Tess Lawrie is a 30-year veteran WHO evidence synthesis expert. Her conclusion is every bit as meaningful as the article's rank. Here are those words,
“Moderate-certainty evidence finds that large reductions in COVID-19 deaths are possible using Ivermectin. Using Ivermectin early in the clinical course may reduce numbers progressing to severe disease. The apparent safety and low cost suggest that Ivermectin is likely to have a significant impact on the SARS-CoV-2 pandemic globally.”
https://pubmed.ncbi.nlm.nih.gov/34145166/
Maybe it is time to ask why Dr. Pierre Kory’s peer-reviewed narrative review of Ivermectin ranks #38 out of the same 18 million publications.
He concludes, “Finally, the many examples of Ivermectin distribution campaigns leading to rapid population-wide decreases in morbidity and mortality reduction indicate that an oral agent effective in all phases of COVID-19 has been identified.”
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8088823/
If Dr. Lawrie’s paper is ranked in the top 5% of the top .001% of all such published medical articles of all time, then Dr. Kory’s is not far behind. His is 38/180 of the top .001% or the top 21% of the top .001%
Thus, both articles would rank in the rarified atmosphere of nearly one in a million.
Therefore, the reader must now ask why two magnificent independent reviews from two different continents, coming to the same conclusion, are both ignored by our world’s medical leaders?
Uttar Pradesh is one such population that experienced a considerable drop in COVID-19 morbidity and mortality months AFTER Dr. Kory’s article was published on April 22, 2021. Therefore, one must ask that if Ivermectin so predictably and safely eradicates COVID-19, then why is it not being systematically deployed over all the world, as Dr. Kory and Dr. Lawrie suggest?
Perhaps every reader needs to ask themselves this question - Why is it that BOTH Dr. Lawrie’s and Dr. Kory’s supremely-rated expert review articles, published in the medical literature on PubMed, the National Library of Medicine, are BANNED from Wikipedia?
Although India’s Ivermectin victory over COVID may have been lost on bent-on-vaccinating-everyone Big Pharma and Big Regulators, the message seems to have gotten through to the man on the street. If Google Trends is any indicator, interest in Ivermectin is exploding, and for good reason. We are all being systematically deceived by influential organizations in the name of profits.
A daily onslaught of media propaganda bombards us with messages attempting to steer us away from the safest and most effective treatments.
Interest in Ivermectin and India is only increasing and has now reached an all-time high. India’s conquest of COVID-19 is concealed no longer. The secret is out. And perhaps, at long last, that much-anticipated WHO Final Report detailing the most successful Pandemic campaign of any place on earth will be published.
https://www.amazon.com/Ivermectin-World-Justus-R-Hope/dp/1737415909
*
*
Uttar Pradesh indijska država uporablja Ivermectin in nima več COVIDa_
https://www.youtube.com/watch?v=j6cVbhxRKls
*
https://novazonaistine.blogspot.com/2021/10/justice-hope-kako-je-indija.html?spref=fb&fbclid=IwAR3f-bd_oTjeC2eb1QjJcUQ_RLBl-frBecZ4Ae3on3UBWy1fA1enZkeA_6I
*
Darija Lovšin: FB 2.11. 2021
Pismo natisnite, ga vložite v kuverto (lahko podpišete ali ne, po želji) in pošljite na Urad predsednika že jutri.
May 06, 2021
